Article Text

Abstract
Background The increasing fragmentation of healthcare has resulted in more patient handoffs. Many professional groups, including the Accreditation Council on Graduate Medical Education and the Society of Hospital Medicine, have made recommendations for safe and effective handoffs. Despite the two-way nature of handoff communication, the focus of these efforts has largely been on the person giving information.
Objective To observe and characterise the listening behaviours of handoff receivers during hospitalist handoffs.
Design Prospective observational study of shift change and service change handoffs on a non-teaching hospitalist service at a single academic tertiary care institution.
Measurements The ‘HEAR Checklist’, a novel tool created based on review of effective listening behaviours, was used by third party observers to characterise active and passive listening behaviours and interruptions during handoffs.
Results In 48 handoffs (25 shift change, 23 service change), active listening behaviours (eg, read-back (17%), note-taking (23%) and reading own copy of the written signout (27%)) occurred less frequently than passive listening behaviours (eg, affirmatory statements (56%) nodding (50%) and eye contact (58%)) (p<0.01). Read-back occurred only eight times (17%). In 11 handoffs (23%) receivers took notes. Almost all (98%) handoffs were interrupted at least once, most often by side conversations, pagers going off, or clinicians arriving. Handoffs with more patients, such as service change, were associated with more interruptions (r=0.46, p<0.01).
Conclusions Using the ‘HEAR Checklist’, we can characterise hospitalist handoff listening behaviours. While passive listening behaviours are common, active listening behaviours that promote memory retention are rare. Handoffs are often interrupted, most commonly by side conversations. Future handoff improvement efforts should focus on augmenting listening and minimising interruptions.
- Transitions in care
- Patient safety
- Communication
- Hospital medicine
- Checklists
Statistics from Altmetric.com
Introduction
The increasing fragmentation of healthcare has resulted in more patient care transitions and hospitalists are increasingly used to accommodate gaps in clinical care. The number of hospitalists in academic hospitals has risen dramatically in the past 10 years, largely due to the implementation of resident duty hour regulations.1–4 Hospitalised patients may be handed-off between doctors, an average of 15 times during a 5-day hospitalisation.5
In the face of increasing handoffs, hospitalists have played leading roles in advancing care transitions. The importance of handoffs is emphasised as one of the core competencies of hospital medicine by the flagship organisation for hospitalists, Society of Hospital Medicine (SHM).6 Many groups, including the SHM and the Joint Commission, have been working to set guidelines for safe and effective handoffs.7 ,8 Few studies have focussed on hospitalists’ behaviours during patient care handoffs; however, those studies which have done so demonstrated these handoffs are plagued with similar problems as resident handoffs.9 As a result of the greater focus on handoff quality among practising hospitalists and residents, education and instruments to formally evaluate handoffs are needed.
Most handoff studies focus on the sender, or person giving information, but the receiver is also a crucial participant.10 The receiver must confirm their successful comprehension of information and ensure transfer of professional responsibility.11 Prior work at our institution demonstrated that critical information during a handoff was not effectively transferred from the departing clinician to the receiving clinician, despite recommended sending conditions, such as dedicated time, room and protection from interruptions.12 Furthermore, the departing clinician incorrectly believed they had successfully communicated the most important information necessary for patient care nearly 60% of the time.12 Recent literature has called for a shift from a handoff as a transfer of information to a co-construction of the oncoming provider's understanding of the patient; however, no studies exist that examine specifically the behaviour of the receiver during the handoff.13 Given the significance of receivers in the transfer of information and the paucity of data on effective listening behaviours, we aim to observe and characterise the listening behaviours of handoff receivers on an academic non-teaching hospitalist service.
Methods
Setting
This study was conducted at a single, academic tertiary care institution. The Section of Hospital Medicine at the University of Chicago Medical Center is comprised of 17 faculty physicians and five mid-level practitioners (nurse practitioners and physician assistants), and staffs a non-teaching multi-specialty service of solid-organ transplant (excluding heart), oncology and overflow general medicine patients. In addition, section faculty also staff traditional housestaff-covered teaching services. Fourteen of the 17 academic clinicians staff the uncovered or non-teaching service and were eligible for participation in this study.
The non-teaching service consists of one team, staffed by two of 14 possible physicians, and 2 or 3 mid-level practitioners. Physicians rotate on the service for 1 or 2 weeks at a time. The patient census ranges from 2–12 patients per team with 0–10 new patients admitted every day. Overnight, the service is covered by either a faculty hospitalist or moonlighting subspecialty fellow. Handoffs between outgoing and incoming providers were observed assessing both shift and service changes on Monday mornings (shift change), Tuesday mornings (service change) and Friday afternoons (shift change). A shift change is defined as the transfer of care between clinicians previously caring for the patients on the service (eg, physician returning at 7:00 after leaving at 17:00 the previous day), whereas a service change is the transfer of care to a new set of clinicians assuming care for patients that they have not previously cared for (eg, physician starting service and picking up new panel of patients).6 Tuesday morning was selected to represent a service change; Monday and Friday shift changes were selected secondary to the highest number of mid-level and physician based faculty available for the handoff and also as these generally represented peak (Monday AM) and nadir (Friday PM) of patient census. In addition, on Friday afternoon, clinicians sign out individually to the incoming physician, who covers the service from 15:00 until 22:00 and transfers the patients to the incoming night physician. These handoffs consistently occurred at a dedicated time (7:30, 16:30), in a dedicated room. On Mondays and Tuesdays, the sender (night physician who was a hospitalist or a moonlighting subspecialty fellow) and the entire incoming team (two physicians, two-three NPs/PAs) are present for the handoff. The night shift physician shift is from 19:30 until the following 7:30; the day shift clinicians begin at 7:30 until 17:00 and the mid-shift occurs from 15:00 until 22:00. All clinicians have access to a Word-based signout document which includes clinical data such as hospital course, medications and code status. All providers (hospitalists, nurse practitioners, physician assistants and moonlighters) were approached to participate. Written consent was obtained from all participants after a brief introduction to the study. This study was approved by the University of Chicago Institutional Review Board.
Data collection
Overview
Two third-party research assistants (EG, PS, observed handoffs with a focus on physician listening behaviours, using a newly developed paper-based tool, the HEAR (Handoff Evaluation Assessing Receivers) checklist (see online supplementary appendix A). Observers noted the listening behaviour of the single covering physician. Timing was measured on the same wall clock to the nearest minute. Time of the handoff was from handoff start, including all interruptions, until the completion of the handoff. The individual observed was chosen by the observers based on which provider had been observed least frequently in the recent past.
Developing the HEAR checklist
The HEAR checklist was developed following a review of relevant listening literature, including prior handoff, organisational, psychological, cognitive science and medical literature.14–20 Our literature review demonstrated that listening styles vary between individuals and do not necessarily relate to quality of the listening. In fact, the spectrum of outward displays of listening correlate to actual comprehension of information to varying degrees.14 Passive listening behaviours, such as head nodding, indicate listening but do not confirm the receipt of information as strongly as active listening behaviours, such as note-taking and read-back.17 It is important to consider that note-taking has been shown to enhance memory, and read-back is recommended by the Joint Commission.7 ,17 Interruptions have been shown to prevent proper transfer of information and can cause adverse patient events.14 ,21
The checklist is a paper-based tool to be completed by a third-party observer during the handoff. The checklist was piloted on the hospitalist service in June 2010 and was modified based on real-time observations. Modifications included dividing side conversations by topic and qualifying interruptions to reflect what was causing the disruption.
The HEAR checklist has three domains: (1) displays of understanding, (2) processing information, and (3) interruptions/distractions. The ‘displays of understanding’ domain documents the presence or absence of passive listening behaviours such as affirmatory statements (eg, ‘uh-uh, yes, okay, I see’) and head nodding. The ‘processing information’ domain quantifies and qualifies active listening behaviours such as read-back, access to a written copy of the signout, note-taking and question asking. Questions were divided into directly-related questions (ie, clarification and ‘next-step’ questions and indirectly-related (ie, systems-based and ‘other’ questions). Clarification questions were defined as requests for repeating information already conveyed in one form (ie, verbal or paper) such as ‘and to clarify the patient will be getting a CT today?’ ‘Next-step’ questions are higher level, requiring information synthesis, or for information not yet conveyed in any form. Systems-based questions relate to hospital systems issues; for example, ‘the lab doesn't run those tests on the weekend do they?’ ‘Other’ questions refer to questions unrelated to patient care. The third domain, ‘interruptions/distractions’, tallies and characterises interruptions during the handoff. Interruptions include side conversations, pagers and clinicians entering the room. There is additional space for qualitative observer comments. Investigators noted the number of patients handed off and handoff duration.
The HEAR checklist is intended to be utilised as an instrument to assess the quality of listening behaviours displayed and not to generate a numeric score of listening behaviour.
Observer training
Observers utilising the HEAR checklist were trained using education developed from listening psychology and handoff literature and via expert review of scenarios during the pilot phase of the checklist. The observers viewed between 9 and 12 handoffs during the pilot and modification period for the checklist. Observers were trained on behaviours to expect such as read-back and affirmatory statements. Observers discussed their observations weekly with the research team focussing on questions that emerged during observations.
Concurrent validity of HEAR checklist
To assess the concurrent validity of the HEAR checklist, we compared it with another measure of handoff quality that we have previously used, the Handoff Clinical Evaluation Exercise (CEX) (see online supplementary appendix B). This instrument was developed and is based upon a previously-validated, real-time educational evaluation tool, the Mini-CEX.22 The Handoff CEX instrument includes assessment of five domains, including: organisation, communication skills, content, clinical judgment, humanistic qualities and overall handoff competence.23 Each domain is scored on a 9-point scale that includes unique role-based anchors for the highest and lowest scores of each domain. For example, the unsatisfactory anchor for the communication domain included ‘understanding not confirmed, no time for questions’ whereas the superior anchor included ‘understanding confirmed, questions elicited’. The Handoff CEX instrument asks evaluators to rate overall handoff performance and its components on a 9-point scale. Senders and receivers evaluate each other using Handoff CEX forms.
Finally, participants perception of workload was assessed using a constructed response item on the Handoff CEX: ‘On a scale of 1–10 (1 being not bad at all and 10 being your worst night at the hospital), how would you rate your workload this shift?’ End of shift clinicians were asked to rate their workload on the CEX after the completion of the handoff.
Data analysis
Quantitative analysis
Data from the HEAR checklists were analysed using descriptive statistics and two-sided t-tests, to compare passive and active listening behaviours and shift versus service change. Active and passive listening behaviours were dichotomised into ‘done’ and ‘not done’ in order to utilise two-sided t-tests. Correlation coefficients were utilised to discern relationships between different observed factors, specifically handoff communication quality and other observable listening behaviours. Concurrent validity of domains were assessed comparing the results obtained using the HEAR checklist to the Handoff CEX ratings of the same handoff using Spearman's correlation coefficients. Statistical analysis was performed using Stata V.11 (Stata Corp, College Station, Texas, USA).
Qualitative analysis
An inductive approach, with no apriori hypotheses, was used to identify themes in the side conversations and questions recorded by the observers during the handoff process.24 The units of analysis were sentences and phrases. Four investigators (EG, PS, JF, VA) discussed and determined themes. Reconciliation of all discrepancies was achieved by discussion among the reviewers to achieve 100% consensus.
Results
From June through November 2010, forty-eight handoffs (88% of handoffs scheduled for observation) were evaluated representing 19 different individual receivers. All 14 of the 14 eligible physicians (100%) and all five eligible mid-level providers (100%) were approached and consented for participation in this study. Seventy-nine percent of physicians (11/14) and all five (5) NP/PA clinicians were observed at least once. The median number of patients discussed in each handoff was eight patients (IQR 4–12) and the mean time per handoff was 12.2 min (SD±9.1 min). Roughly half of handoffs observed were shift change (52%) with the other half being service change (48%) (see table 1).
Characteristics of hospitalist handoffs observed from June-November 2010 (n=48)
Shift change handoffs, which occurred on Monday mornings and Friday afternoons, were grouped in the analysis as the commonality was that the receiver of the handoff had prior familiarity with the patients on the service. Not surprisingly, more patients were discussed in service change handoffs (9.5±4.6) than in shift change handoffs (6.5±3.6) (p=0.03), and the duration of the handoff was nearly twice as long for service change, at 16.5 min (SD±8.9) than shift change at 8.6 min (SD±8.1) (p=0.02).
Listening behaviours
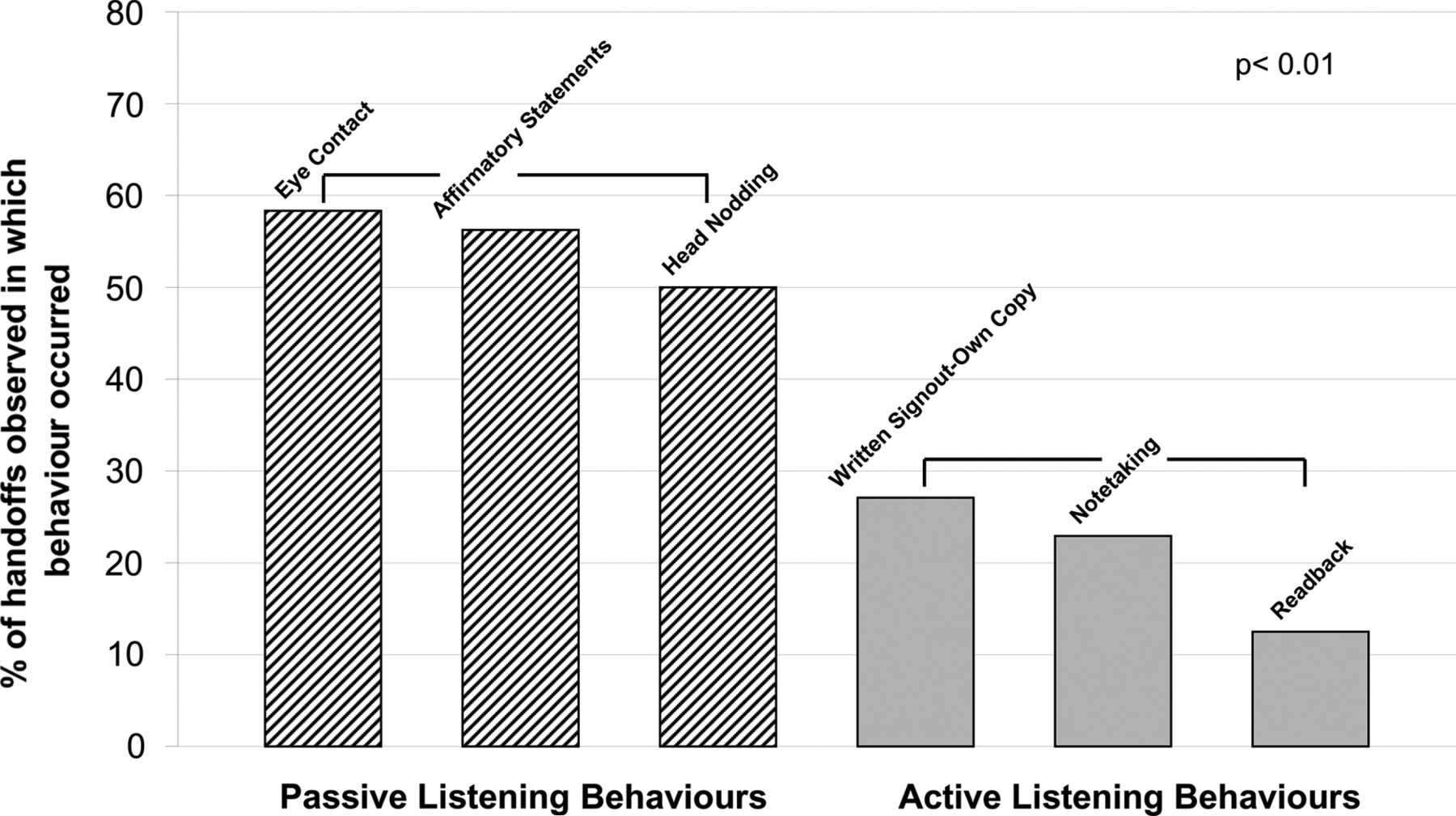
In the 48 handoffs observed, passive listening behaviours occurred with greater frequency than active listening behaviours (see figure 1). In the ‘displays of understanding’ domain, the passive listening behaviours of affirmatory statements, head nodding and eye contact occurred in 56, 50, and 58 percent of handoffs, respectively. The active listening behaviours occurred less frequently than passive listening behaviours (p<0.01). In the 48 handoffs, read-back occurred eight times (17%). In 13 (27%) handoffs, the receiver had their own copy of the written signout on which they could follow along. In 11 handoffs (23%) the receivers took notes (see figure 1).

Listening Behaviors Observed During Hospitalist Handoffs.
The mean number of questions asked per handoff was 2.1, with 67% directly related to handoff content and 33% related to systems issues (Mean of 1.38 vs 0.69 per handoff, p=0.0046) (see table 2). Of the directly related questions, 65% were clarification questions and 35% were ‘next-step’ anticipatory questions (p=0.026) (see table 2).
Characteristics of questions asked during hospitalist handoffs
Interruptions
Almost all (98%) handoffs observed had at least one interruption and the median number of interruptions per handoff was 3, range (0–12). The most frequent interruptions were side conversations (72%), pagers going off (53%) and clinicians arriving for handoff (50%). The clinicians arriving were either members of the oncoming team not being observed, or those on one of the other uncovered services sharing the common workspace. In some instances, the off-going physician may have elected to handoff to a mid-level provider without the accompanying MD-level faculty member present because of time constraints and when that clinician arrived, they would ultimately participate in the receipt of the handoff but would not be observed by the research staff. Side conversations occurred at least once in over half (59%) of handoffs, with a median of three side conversations per handoff and range of 0–5. Side conversations ranged in content from personal (eg, relating to social topics with no significance to job responsibility); professional well being (eg, relating to clinician job satisfaction and commiseration over job stress) and systems-based (eg, relating to hospital or infrastructure issues) (see table 3).
Qualitative analysis of side conversations observed in hospitalist handoffs
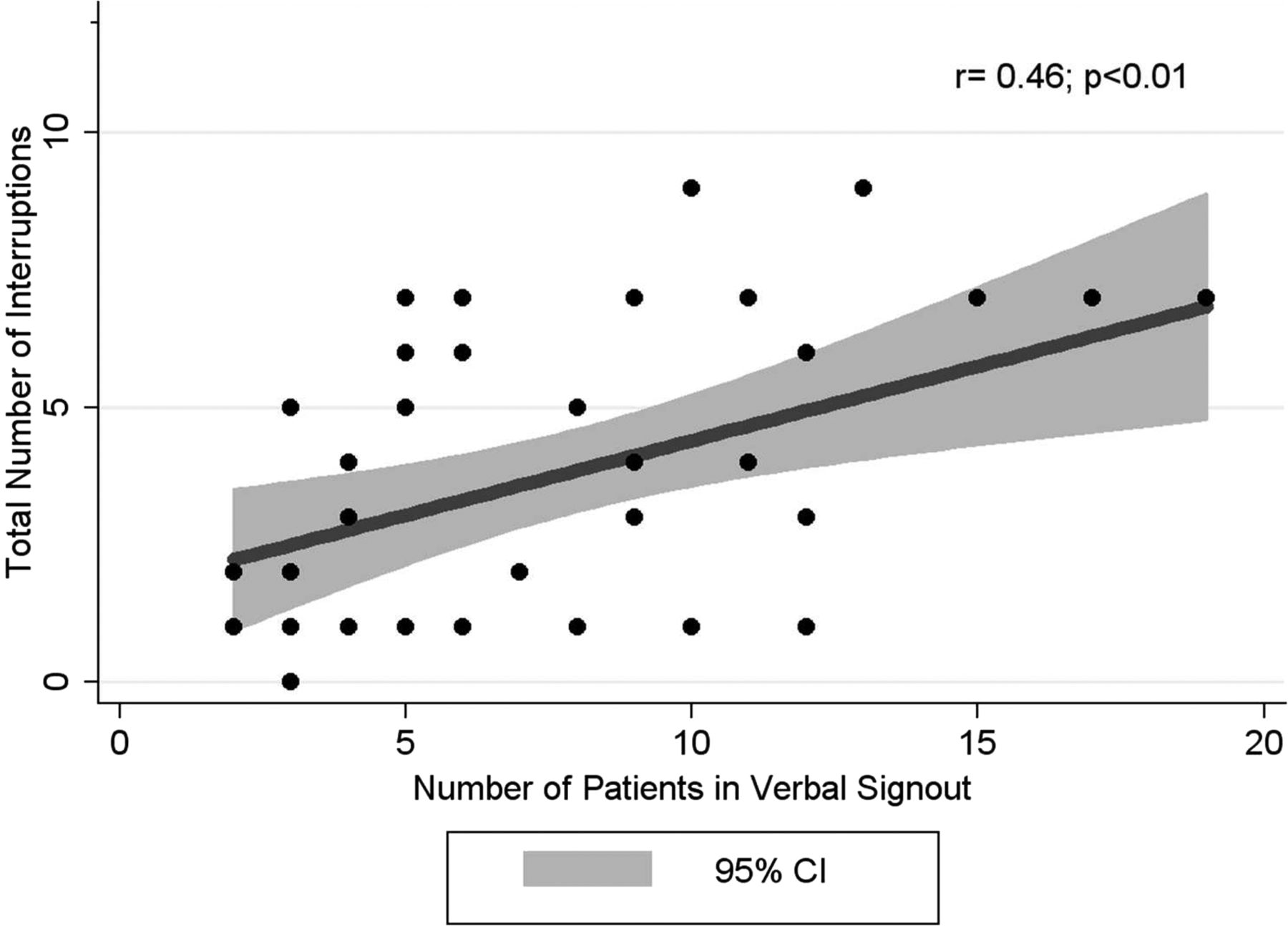
Of note, handoffs with more patients discussed often had greater numbers of interruptions (r=0.46, p<0.01, see figure 2). Although not significant, handoffs with more patients were weakly correlated with more questions asked as well (r=0.29, p=0.07). Similarly, because service change had more patients discussed, there were more interruptions during service change during shift change, with 5.4 interruptions per handoff (95% CI 4.1 to 6.7) during a service change versus 2.8 interruptions per handoff (95% CI 2.0 to 3.6) during a shift change (p<0.01).

{kind=link}
{kind=link}
Total Interruptions Observed Versus Number of Patients in Verbal Signout.
Concurrent validity
Concurrent validity of the HEAR checklist was established by examining pair-wise correlations with the domains of the Handoff CEX, another measure of handoff quality. Briefly, the Handoff CEX instrument includes assessment of five domains, including: organisation, communication skills, content, clinical judgment, humanistic qualities and overall handoff competence.23 A positive and trend toward significant correlation was observed between use of passive listening behaviours and four of the domains on the Handoff CEX: (1) perceived communication skills (r=0.30, p=0.03); (2) clinical judgment (r=0.26, p=0.07); (3) patient focus (r=0.34, p=0.09); (4) overall assessment (r=0.27, p=0.06). Additionally, the number of directly related questions asked by the receiver was positively correlated to clinical judgment ratings on the CEX (r=0.2, p=0.07). Lastly, there was a negative correlation between the total number of interruptions recorded on the HEAR checklist and the rating of the setting by the senders using the Handoff CEX (r=−0.22, p=0.02).
Discussion
While prior studies of handoffs examine the sender's ability to communicate, this is the first to focus on listening behaviours. We found that active listening behaviours (ie, note-taking, access to written signout and read-back), recommended strategies that have been shown to enhance memory, are infrequent in practise.7 ,17 Like other studies, we also observed that handoffs are characterised by frequent, potentially modifiable interruptions.16 We have also demonstrated the feasibility of the use of the HEAR checklist as a tool to provide communication skill feedback to receivers of patient care handoffs, in order to improve their future practise.
Despite the emphasis on active listening behaviours, it is important to consider why they are not often done during handoffs. These findings are consistent with other studies showing lower rates of read-back among residents.25 While passive listening behaviours signal potential comprehension, they do not confirm receipt of information.26 Our analysis revealed a positive correlation between passive listening behaviours and perceived communication skill, which in fact does not confirm receipt and understanding of information provided. Therefore, it is important to promote the use of active listening behaviours during handoffs and encourage these behaviours to be the goal in handoff behaviours. Another possibility for the low rate of read-back is that participants have reported that requesting a colleague to read-back may be perceived as ‘patronising.’ Teaching read-back earlier in training in graduate medical education as a receiver-initiated component of the handoff could improve acceptance of this technique.
One positive finding is that asking questions occurred in all handoffs, with clarification questions asked the most frequently, followed by ‘next-step’ questions and system-based questions. Clarification questions are important to ensure that proper information transfer has occurred. However, ‘next-step’ questions occurred with much less frequency. These questions indicate an active listener attempted to assess clinical rationale from the sender. Future education stressing the importance of asking questions and the type of questions may be helpful in counselling receivers to take a more active role in the handoff process.
Most observed handoffs were interrupted at least once, which is consistent with prior work.16 Side conversations occurred often and varied in subject from personal to professional well-being to systems-based issues. It is important to consider the motivation for side conversations. One possibility is that side conversations may not be inherently bad, and may serve an important professional function. Handoffs have previously been shown to have multiple functions, ranging from the information transfer to physician commiseration.27 For example, one noted side conversation involved the receivers praising the night attending on their work the previous shift. Although these conversations may enhance team building, they also can interfere with the effective transfer of information when they occur during the handoff. The second most common interruption was from pagers going off. The hospitalist service currently does not have a no-page policy during handoffs, which has been instituted for residents in our institution's paediatrics residency programme and for nurses at many institutions during high risk care transitions.12 ,28 The third major source of interruption was clinicians arriving during the handoff. This is likely due to insufficient overlap in shifts between the incoming and outgoing staff.
These most frequent interruptions are potentially intervenable. Although they may serve a purpose for collective venting and team building,27 discouraging side conversations during the handoff period could be addressed through education and culture change, with time separate from the handoff reserved for commiseration and non-patient care issues. In addition, clinicians arriving for handoff could be reduced through schedule modification, constructing a small amount of overlap time added to each shift in order to prepare for the handoff and ensure participants are in place at the designated start time. Pagers going off could be addressed by instituting a no-page policy during the handoff, which has been shown to work in nursing literature, modelled from the sterile cockpit rule instituted in the aviation industry.29 ,30 The Federal Aviation Administration guidelines state that ‘(n)o flight crewmember may engage in … any activity during a critical phase of flight which could distract any flight crewmember from the performance of his or her duties or which could interfere in any way with the proper conduct of those duties. Activities such as eating meals, engaging in nonessential conversations within the cockpit and nonessential communications between the cabin and cockpit crews (are not permitted).’30 Given the potential consequences of interruptions on patient care tasks,21 and viewing handoffs as a ‘critical phase of flight,’ making a concerted effort to protect the environment from both internal and external interruptions is warranted.
There are several limitations to this study. Our data reflect a single-institution experience and only one service, limiting generalisability. Our sample size is also small. Although we examined concurrent validity of the HEAR checklist, we did not measure other forms of validity, such as the predictive validity of the HEAR checklist on handoff-related outcomes. Furthermore, the HEAR checklist aims to capture listening styles, which vary based on the individual, level of experience, as well as group influences. Finally, the presence of observers during the handoff could cause an alteration in behaviours and impact the perceived quality of the physician's communication skills.31 However, this initial study of listening behaviours during patient handoffs may provide a useful starting point for future intervention studies or studies that link handoff quality to outcomes.
In conclusion, the HEAR checklist is a feasible tool to observe and characterise physician listening behaviours during patient handoffs. Although effective, active listening behaviours are encouraged by national organisations, they occur infrequently. Receivers most often ask clarification questions during the handoff, followed in frequency by the more active ‘next-step’ questions. Handoffs are often interrupted, most routinely by side conversations, pagers going off, and clinicians arriving for the handoff, all of which are potentially modifiable. Future work should focus on teaching effective listening behaviours and discourage side conversations during the transfer of patient information. In addition, systems improvements such as protected time from non-emergent pages and overlapping shift time for a dedicated handoff period should be adopted.
Acknowledgments
We would like to thank the hospitalists and NPA’s at the University of Chicago Section of Hospital Medicine for their enthusiasm and participation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix A
- Data supplement 2 - Online appendix B
Footnotes
-
Funders We acknowledge funding from the Agency for Healthcare Research & Quality (1 R03HS018278-01) ‘Development and Validation of a Tool to Evaluate Hand-off Quality’ (PI Arora); The National Institute on Aging Short-Term Aging-Related Research Program (5T35AG029795), and the Pritzker Scholarship & Discovery Program.
-
Prior presentations Prior presentations of the data include the 2010 Pritzker Summer Research Program Forum, 2011 Society of Hospital Medicine Annual Meeting in Dallas, TX, 2011 Midwest SGIM Meeting in Chicago, IL, 2011 Midwest Hospital Medicine Meeting in Chicago, IL, 2011 University of Chicago Medical Education Day.
-
Competing interests None.
-
Contributors JMF had full access to the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: EAG, VMA, SSB, JMF. Acquisition of data: PGS, SSB, EAG. Analysis and interpretation of data PGS, SSB, EAG, VMA, JMF. Drafting of the manuscript: EAG, SSB, PGS, JMF, VMA. Critical revision of the manuscript for important intellectual content: PGS, SSB, EAG, VMA, JMF. Statistical analysis: EAG, JMF, VMA. Obtained funding: VMA, JMF. Administrative, technical or material support: PGS, SSB, EAG, VMA, JMF. Study supervision: JMF, VMA.
-
Ethics approval Institutional Review Board of the University of Chicago Dvision of the Biological Sciences.
-
Provenance and peer review Not commissioned; externally peer reviewed.