Article Text

Abstract
Background Oncology care is delivered largely in ambulatory settings by interdisciplinary teams. Treatments are often complex, extended in time, dispersed geographically and vulnerable to teamwork failures. To address this risk, we developed and piloted a team training initiative in the breast cancer programme at a comprehensive cancer centre.
Methods Based on clinic observations, interviews with key staff and analyses of incident reports, we developed interventions to address four high-risk areas: (1) miscommunication of chemotherapy order changes on the day of treatment; (2) missing orders on treatment days without concurrent physician appointments; (3) poor follow-up with team members about active patient issues; and (4) conflict between providers and staff. The project team developed protocols and agreements to address team members’ roles, responsibilities and behaviours.
Results Using a train-the-trainer model, 92% of breast cancer staff completed training. The incidence of missing orders for unlinked visits decreased from 30% to 2% (p<0.001). Patient satisfaction scores regarding coordination of care improved from 93 to 97 (p=0.026). Providers, infusion nurses and support staff reported improvement in efficiency (75%, 86%, 90%), quality (82%, 93%, 93%) and safety (92%, 92%, 90%) of care, and more respectful behaviour (92%, 79%, 83%) and improved relationships among team members (91%, 85%, 92%). Although most clinicians reported a decrease in non-communicated changes, there was insufficient statistical power to detect a difference.
Conclusions Team training improved communication, task coordination and perceptions of efficiency, quality, safety and interactions among team members as well as patient perception of care coordination.
- Team Training
- Patient Safety
- Teamwork
- Quality Improvement
- Ambulatory Care
Statistics from Altmetric.com
Introduction
Outpatient oncology care is a team endeavour. The intricate diagnostic and therapeutic algorithms, complex and potentially dangerous treatment regimens, and necessary coordination of multimodality and extended courses of treatment require effective interdisciplinary and inter-professional communication and coordination for the successful care of the patient. Although therapeutic advancements, coupled with rapid innovations in information technologies, have created the potential for superior treatments and outcomes, they are accompanied by a magnified risk for adverse events when precipitated by failures of coordination and communication. Physicians, nurses, pharmacists and other healthcare staff long have worked together in teams, yet only relatively recently, motivated by the Institute of Medicine report (2003), have academic programmes and healthcare organisations begun to provide formal interdisciplinary training to promote team behaviours.1–3
Other complex, high-risk industries, notably aviation, nuclear power and the military, have used the concepts of crew resource management to ensure safety and quality.4–6 These concepts entail creating environments that support team members’ ability to develop a shared vision and mental model of their work, ask for and offer relevant information, communicate proposed actions, advocate specific concerns and effectively manage conflict.7–11 To date, areas of healthcare that have adapted these concepts have been largely limited to geographically-contained settings, such as emergency departments, labour and delivery suites, intensive care units and operating rooms, where team members are consistent and co-located in time and place.12–19 Outpatient oncology, however, like other medical subspecialties, possesses characteristics which are quite different, making communication, coordination and collaboration both critical and more difficult. Team members are dispersed, practicing in different physical locations and at different times. Team members are frequently transient, with individual physicians sharing the care of different patients with a variety of infusion nurses, clinic assistants, nurse practitioners or other physicians in series or parallel fashion. The same is true of the other members of the team. These characteristics produce a collection of ‘virtual teams’ that make it challenging to exchange messages of clarification, monitor each other's behaviour, maintain a shared mental model and provide substantive and timely feedback. To address the complexity and risks of delivering care in this environment, we adapted the concepts of crew resource management, applied successfully in other industries and other medical settings, to develop and implement a team training programme in our academic ambulatory oncology centre.
Our primary aim was to reduce the risk of error in the processes of ordering, dispensing and administering chemotherapy in our outpatient adult oncology setting. We hypothesised that implementation of the team training concepts would require new agreements, tools and behaviours among team members, as well as a redesign of current systems, to support the changes.20 Our secondary aim was to improve the practice environment and team satisfaction through the more effective team communication and collaboration that would be realised by applying crew resource management principles in our setting.
Methods
Study site
A pilot oncology team training programme was developed and implemented between August 2008 and March 2009 in the ambulatory clinical practice and treatment areas of the Dana-Farber Cancer Institute (DFCI), a US National Cancer Institute-designated comprehensive cancer centre. We initiated the team training programme in the Breast Oncology Center (BOC), the largest of the solid-tumour disease centres. In 2009, BOC patients logged more than 24 079 exam visits and more than 13 400 infusion visits (occurring on a different floor), accounting for 16% of all exam and 14% of all infusion patients treated in the ambulatory practice of the DFCI.
Programme development
A steering committee of senior clinical leadership, BOC physicians, nurse practitioners, programme and infusion nurses, pharmacists and clinical and administrative support staff was convened and received 16 h of formal training in the concepts of team training. A physician/nurse consulting team was hired to prospectively observe the clinical practice, infusion unit and ‘back office’ administrative support environment and to conduct interviews with members of the interdisciplinary team. The goal was to identify areas vulnerable to communication failures that might introduce patient risk, interfere with the ability to perform critical tasks or detract from a positive practice environment.
Using a modified failure mode and effects analysis, the BOC steering committee, meeting weekly for 6 months, evaluated data from the observations and interviews and reviewed its members’ personal experiences in the practice environment to identify risks for error, determine how team training concepts might be employed to address those risks, develop tools to support teamwork behaviours and establish performance metrics.
This combination of direct observation and key informant interviews, combined with analyses of the centre's adverse event reporting system, helped the steering committee identify and prioritise areas of vulnerability for which they designed interventions:
-
Uncommunicated changes in chemotherapy agent or dose by the clinician to the infusion nurse on the day of treatment (‘non-communicated change orders’) undermined a shared mental model, diminished trust and feelings of respect between team members, and impaired each member's ability to advocate for patient safety with other members of the care team.
-
Missing orders for patients scheduled for chemotherapy on days they were not scheduled to see their physicians (missing orders for ‘unlinked’ appointments) reduced situational awareness, undermined a shared mental model, and engendered frustration for both infusion nurses and patients at the resultant delays in obtaining orders.
-
Incomplete follow-up and communication with other team members on pending issues, tests or changes in patient status prevented cross-monitoring, as well as team members’ ability to have a shared mental model or to advocate for patient safety.
-
Dysfunctional communication and unresolved conflict between team members. Such conflicts occurred for several reasons. In some cases, the lack of appreciation for how one team member's workflow adversely affected other team members’ ability to perform their jobs, or that these workflows might even jeopardise patient safety, created a culture of blame and frustration. In others, hierarchical or unchecked disruptive behaviours created barriers to effective and respectful communication. In addition, geographic dispersion of team members posed challenges to streamlined, effective, timely communication of critical information.
Each of these vulnerabilities contributed to conflicts between team members, undermined a shared mental model, and impaired team members’ ability to cross-monitor each other's behaviour or to advocate for patient safety. Team training with its emphasis on developing shared mental models, cross-monitoring, situational awareness and effective conflict resolution was an attractive approach to address these issues.
These areas of vulnerability were prioritised based on the magnitude of the associated risk and the frequency with which the risk occurred in the practice environment. Other vulnerabilities that were considered, but not chosen for the first implementation, were put into a ‘parking lot’ to be addressed later.
Interventions
For each identified risk area, the BOC steering committee made agreements about roles, responsibilities and behaviours of each team member. Tools were developed and systems modified to enhance situational awareness and a shared mental model among team members, and to support implementation of the agreements.
Non-communicated change orders
Changes in chemotherapy orders are common in ambulatory oncology. Agents may be changed because of disease progression, or dosages held or decreased because of toxicity. Failure by a clinician to communicate last-minute chemotherapy order changes to the infusion nurse and pharmacist have resulted in patients being treated with incorrect drugs or at inappropriate dosages. Several electronic and manual double-checks exist to prevent such events. However, these systems occasionally fail.
The committee first developed a shared definition of a change order, which included hold orders, new patients’ initial orders, new regimens or drug orders, re-initiation of therapy after a prolonged break, additional non-chemotherapy orders entered on the day of treatment (eg, electrolyte replacement) and/or dose reductions. Members agreed that change orders must be accompanied by direct and timely verbal communication between the clinician and the infusion nurse, and subsequently between the nurse and the pharmacist.
A tool was developed to facilitate provider–nurse communication whereby the provider was given a daily list of the phone numbers and names of the nurses who would be treating the patients they saw in clinic each day. Team members committed to the following workflow for change orders: (1) Ordering clinicians would never be put on hold when calling a change order to the infusion unit and (2) Ordering clinicians would call the infusion nurse and enter the change order while still in the exam room with the patient to avoid distraction and inadvertent omission upon leaving the exam room. Checklists for change order communication were created to ensure that only critical information was conveyed. If the patient's nurse was not immediately available, a partner nurse would take the call, verify the information with appropriate check-back and assume responsibility to relay the information to the patient's primary nurse.
In addition to the change order communication protocol outlined above, the committee agreed upon specific guidelines for telephone, paging and email communications to facilitate provider–nurse communication, while avoiding frequent, unnecessary interruptions. They also agreed upon reasonable response times to pages and determined an algorithm for conflict resolution and escalation to senior clinical leadership if pages were not returned within the agreed upon timeframe. This paging algorithm provided a shared expectation of communication processes among team members.
Missing orders for unlinked visits
Many chemotherapy treatments are administered more frequently than is necessary for patients to see their providers. For example, patients may receive treatment weekly, but only see their physician every 3 or 4 weeks. Orders for these unlinked visits, that is, infusion visits at which chemotherapy is administered but a physician visit does not occur, are usually written electronically in advance, for a several-week cycle of treatment. Missing orders for unlinked visits occur routinely, usually due to patient or provider schedule changes. If orders are missing, nurses need to page providers to enter orders, introducing delays and frustration for patients and staff alike. Clinicians may be off site when paged, particularly on weekends, and unable to enter orders. This delays care and requires the nurse to obtain orders from a covering colleague who may be unfamiliar with the patient. The pharmacist on the committee noted that preparatory planning occurred in pharmacy 2 days prior to scheduled infusion visits. Using this opportunity to note the absence of orders 48 h prior to scheduled, unlinked visits, the pharmacist agreed to send reminder emails to the appropriate clinicians. This allowed the primary providers ample time to enter the missing orders and update the plan of care at a time when they could conveniently access patient records and the order entry system, ensuring a shared mental model and situational awareness for team members.
Incomplete follow-up on pending tests and changes in clinical status
Timely follow-up of the voluminous laboratory tests and radiological scans in oncology has significant treatment and prognostic implications for patients. Further, patients frequently experience symptoms or changes in their clinical status that prompt calls to clinicians, both during and outside of usual business hours. It is important that these test results and clinical changes be shared with the clinical team to maintain a shared mental model and avoid overlooking critical information or duplicating efforts.21 To minimise these risks, the committee agreed that each physician–nurse practitioner/physician assistant team and its clinical administrator meet weekly (or at least biweekly) to facilitate shared knowledge about recent patient events and follow-up on critical information. The administrator was charged with scheduling the weekly team meeting and providing a list of patients who had been scheduled to see the physician and/or nurse practitioner/physician assistant over the preceding 4 weeks and the week ahead. The team reviewed each patient on the list and discussed any ‘no shows,’ test results, changes in status, hospitalisations or other important issues, and determined who would follow-up on each issue and report back to the group. Creating the shared mental model around the patient's plan of care allowed team members to advocate for safety and cross-monitor each other on the plan of care.
Dysfunctional communication and conflict resolution
The committee adopted the use of the situation, background, assessment and recommendation (SBAR) technique to facilitate concise, effective communication exchanges. In addition, the describe, express, specify, consequences script (DESC) and the ‘Two-Challenge Rule’ were identified as tools to facilitate conflict resolution between team members.10 ,22 The Two-Challenge Rule encourages team members to express a safety concern twice, if the first attempt was not satisfactorily addressed. SBAR may be used in the discussions around chemotherapy change orders whereas the DESC script is useful for conflict resolution when agreed upon communication standards are violated. The DESC scripts have been particularly helpful to support staff in structuring conversations they felt were difficult to initiate. Coached by their managers in using this format, several of them emerged from these conversations feeling validated, respected and more fully a part of the clinical team.
Implementation
A curriculum containing the concepts of crew resource management, and incorporating the agreed upon behaviours and tools, was developed with the assistance of outside consultants. The team training concepts were implemented using a train-the-trainer model. BOC physician–nurse pairs from the train-the-trainer group trained all BOC faculty, nursing and support staff in six mandatory 2-h sessions of approximately 20 people (total ∼115 attendees) over a 2-week period. The first half of each training session focused on team training principles and supporting data. The team training curriculum included detailed information, supported by evidence and literature, on the role of leadership, communication techniques, developing shared mental models and situational awareness, and error reduction strategies such as cross-monitoring and advocating for safety. The second half of the course focused on the agreements and interventions adopted by the group. Each intervention was introduced with an actual case-based scenario that was drawn from the care of BOC patients, and illustrated a communication failure and its consequences. A ‘kick-off’ date was established for implementation of the new tools and agreements once all clinicians and staff were trained.
Evaluation and measurement
A mixed-methods evaluation approach was used to assess a variety of measures that the steering committee hypothesised to be related to the implementation of teamwork training. The group hypothesised that team training would reduce the rate of non-communicated change orders, improve the timeliness of orders for unlinked chemotherapy visits, improve patients’ perception of teamwork among their care team, and enhance staff members’ perceptions of quality, safety, and teamwork. The group also hypothesised that the intervention would reduce the number of safety events that resulted from teamwork problems.
Prior to training, the steering committee collected baseline data for 2 weeks regarding the frequency of non-communicated change orders by the clinician to the infusion nurse. Nurses were interviewed daily about whether any change orders occurred for each of their breast cancer patients and, if so, whether the change had been verbally communicated. Six months following implementation we repeated this measurement using the same methodology.
To assess timely order entry for unlinked visits, pharmacists used the electronic chemotherapy order system to determine the frequency with which patients with unlinked infusion appointments did not have orders written at the time of arrival for their treatment. This measurement was obtained at baseline, prior to the initiation of email reminders from pharmacy staff, and continued at 2-week intervals.
To ascertain patient perception of teamwork, patients’ responses to the Press-Ganey patient satisfaction survey item ‘Degree to which your care was well coordinated among your doctors/ other caregivers’ were compared for 6 months prior and 6 months following team training implementation. Patients are randomly sampled and asked to rate their perceptions on a scale of 0–5. Scores are subsequently converted to a score of 0–100 by Press-Ganey.
Six months after implementing team training, we conducted an anonymous survey of all BOC staff to determine if the agreed upon behaviours were being maintained and to measure staff perceptions of the effect of team training's key programmatic components. The surveys also ascertained participants’ perceptions about team training's effect on quality, safety and efficacy of care and its impact on the quality of team members’ interactions.
Finally, all patient safety incident reports filed at the DFCI related to the care of BOC patients for 6 months prior to and 6 months following team training implementation were analysed by non-BOC members of the Department of Quality Improvement and Risk Management who judged whether adherence to the team training agreements might have avoided these events.
Analyses were largely descriptive. Staff perception data were collected through anonymous online surveys. Statistical analyses of measures of patient satisfaction and timelines of chemotherapy orders for unlinked appointments were conducted using Stata 9.1 (StataCorp, College Station, Texas, USA). This project was determined in advance by the Dana-Farber Harvard Investigational Review Board (IRB) to be a quality improvement project and therefore exempt from IRB review.
Results
The team training programme was formally implemented on 9 March 2009 after 20 physicians, nurse practitioners/physician assistants, 47 nurses, four pharmacists/pharmacy technicians and 35 support staff (clinic assistants, practice coordinators, clinical research coordinators, administrative personnel) each had completed a 2-h training session. In total, 92% of eligible clinicians/participants completed training, with exceptions due to excused leaves only. Attendance was promoted by the active involvement on the steering committee of the organisation's associate chief medical officer (also a BOC medical oncologist) and vice-president for adult nursing and clinical services, as well as the participation of formal and informal leaders of the BOC. Training sessions were generally interactive and well attended.
On review of the prespecified performance measures, the results were mixed. There was insufficient power to detect a significant difference in the incidence of non-communicated order changes in the BOC prior to and 6 months following implementation of team training. The rate was low at baseline (1.9%) and during follow-up (1.5%). Nevertheless, 100% of providers (physicians, nurse practitioners, and physician assistants) reported it was easier to communicate change orders and the vast majority had a better understanding of when and how to call for a change order (table 1). Similarly, infusion nurses reported a decrease in the frequency of non-communicated change orders and more than three-quarters reported a decrease in the necessity to page clinicians (table 2).
Provider perception of communication effectiveness (affirmative responses)
Infusion nurses' perception of communication effectiveness (affirmative responses)
The incidence of missing chemotherapy orders for unlinked visits decreased from 30% at baseline to 2% within 2 weeks of implementing the pharmacy screening and email reminder system (p<0.001 Pearson χ2) (figure 1). This level has been sustained since team training implementation.

‘Unlinked appointments’: patients with orders in system prior to arrival to the infusion unit, pre-email and post-email reminder, 2009.
Press-Ganey patient satisfactions scores demonstrated an improvement in patients’ perception of the ‘Degree to which your care was well coordinated among your doctors/other caregivers’ from 93.5% for the 6 months prior to team training to 97.4% for the 6 months following team training implementation. This trend in patient-reported perception of the care team's ability to effectively coordinate care has continued to increase over time.
Staff perception surveys also demonstrated a consistently positive impression of the effect of team training on the efficiency, quality and safety of patient care (table 3).
Staff perceptions of team training by discipline (affirmative responses)
Survey response rates exceeded 65% for all professional groups. In all, 86%, 93% and 92% of infusion nurses reported team training had improved the efficiency, quality and safety of patient care, respectively. Physicians, nurse practitioner and physician assistants reported similar results with 75%, 82% and 92% finding that team training had resulted in improved efficiency, quality and safety of patient care. Support staff surveys demonstrated analogous findings (90%, 93% and 90%). In addition, all groups (infusion nurses, providers and support staff) found that team training improved relationships among team members (85%, 91%, 92%) and that members treated each other more respectfully (79%, 92%, 83%). Staff surveys documented additional evidence of enhanced communication and ability to express concerns and ask for help, decreased unnecessary calls and pages, and benefits of team meetings (tables 1⇑–3).
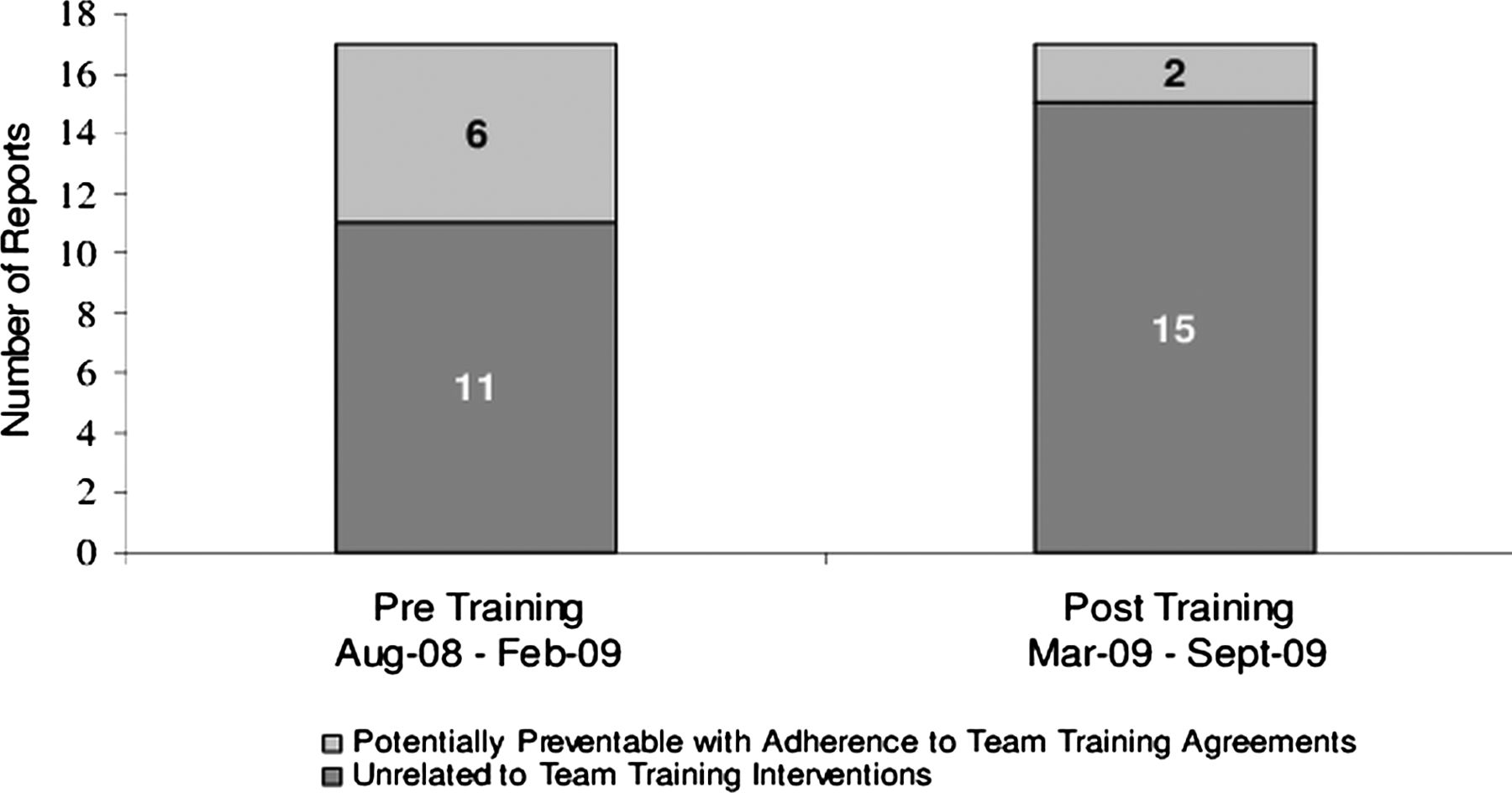
Analysis of safety reports for the 6 months prior to and 6 months following team training implementation was conducted by the Director of Patient Safety, who was not involved in the pilot implementation. This analysis showed 17 reports of adverse events or near misses. Six of these 17 reports involved communication events that, theoretically, could have been prevented by the specific team training interventions implemented. During the 6 months following team training implementation, another 17 reports were filed. Two of these events were judged to be avoidable if there had been strict adherence to the team training behavioural agreements (figure 2). The total number of safety reports filed is not evaluable against the team training intervention because we constantly encourage staff to file reports. However, the causal factors inherent in the safety events filed were analysed and judged against the team training interventions. For example, in one case, had the ordering provider verbally communicated the change in chemotherapy dose to the treating nurse, the wrong dose would likely not have been prepared by the pharmacy, thereby avoiding a near miss in administration.

{kind=link}
{kind=link}
Safety reports 6-month preteam and post-team training intervention.
Discussion
Outpatient oncology presents significant challenges to providing high-reliability patient care. Given complicated treatment algorithms with potentially dangerous multi-drug regimens, geographically and temporally dispersed multidisciplinary team members, and the multitude of necessary and critical handoffs, ambulatory oncology is an environment that is particularly vulnerable to failures in communication and coordination. At a certain level, this environment challenges even the concept of team-based care. Against these challenges, this breast oncology teamwork training programme demonstrates that team training concepts and methods are applicable in this high-risk, complex setting. To our knowledge, this initiative is the first such application in oncology or any other outpatient subspecialty setting.
Aside from demonstrating the feasibility of team training in ambulatory oncology, the project illustrated the challenge of measuring the impact of this type of intervention, an observation noted by other investigators of teamwork.23 The demonstrated success in obtaining orders for unlinked infusion visits improved the process of care, increasing efficiency for staff, reducing pages and interruptions for providers, decreasing patient wait times for treatment and improving utilisation of nursing, pharmacy and infusion chair resources. Press-Ganey patient-reported perceptions of teamwork also improved, reflecting a change discernible to patients.
There was no appreciable difference in the incidence of non-communicated order changes. This finding was not surprising, given the relatively low baseline incidence of these occurrences before team training (less than 2% of patients). Though the frequency of these events was low, the risk of harm from such events is sufficiently high to warrant intervention. When patients’ care plans are shared through effective verbal communication, a shared mental model results, team members’ ability to advocate on behalf of patients is enhanced and conflict is reduced. The staff satisfaction data demonstrated increased communication among members, increased ability to share concerns and improved staff perception of patient safety.
Given the infrequency of the events, however, there was insufficient power to detect a clinically meaningful, or statistically significant, difference in the frequency of non-communicated change orders in this pilot intervention. In fact, it would have required a sample size of almost 30 000 patients to demonstrate a 25% relative improvement on the baseline rate. It was instructive that, prior to team training, clinicians and infusion nurses did not even share a common definition of a ‘change order,’ with some individuals believing that initiation of any chemotherapy constituted such an order and others defining a change order as occurring only when an ongoing chemotherapy regimen was changed. Without a common lexicon, providers and infusion nurses could not have shared a common mental model or expectation of behaviour. Because the group had lacked a common definition for change orders during the preimplementation data collection phase, this lack of clarity could have resulted in under-reporting of non-communicated change orders in the baseline data collection. Though also infrequent at baseline, the decreased number of reported post-training adverse events that were potentially avoidable by adherence to team training agreements may be an indicator of the positive impact of team training on the quality and safety of care.
This systems-based approach, anchored in the principles of team training, allowed the BOC staff to view their team members with a different lens. The hierarchy was flattened as the staff were educated about how errors can occur and that each member was expected to speak up to advocate for safety. Standardised verbal communication about change orders created shared mental models and an understanding of the care plan changes that allowed staff the opportunity to advocate for safety concerns. Process redesign such as that for ensuring the presence of orders for unlinked patients at the time of their appointments reduced pages and increased operational efficiencies and provider and patient satisfaction. Conflict management tools enabled staff to resolve conflict when defined communication agreements failed. By large majorities, providers found it easier and more efficient to verbally communicate a change order, and thus were more likely to communicate them. Infusion nurses reported a decreased need to page providers and this was corroborated by providers’ reporting a decreased number of pages. Further, infusion nurses reported they were more likely to receive a timely response to their pages, a finding that may be related to the universally reported improvement in relationships (85% of infusion nurses, 91% of providers, 92% support staff) and the increased feelings of respect reported by all respondents (79% of infusion nurses, 92% of providers, 83% of support staff). Such an improvement in relationships, particularly by such a low-cost, low-tech intervention is notable.
Involvement by all stakeholders in the care processes—physicians, advanced practice providers, infusion nurses, pharmacists and support staff—was critical to the adoption and success of the team training intervention. The steering committee adapted the concepts and tools used by more ‘self-contained’ teams to promote a shared mental model and situational awareness of the environmental risks. Participation in the process by peers from each role facilitated acceptance by each group. Engagement of formal and informal leaders from each group augmented this acceptance. Actual case-based scenarios, illustrating commonly encountered communication failures and their consequences, facilitated identification with the events and promoted a sense of urgency because they illustrated reality. In addition, buy-in was elicited from all participants by appealing to their self-interest with the promise that simplifying care processes, defining expectations and enforcing accountability could improve quality of work life through practical outcomes, such as decreasing the number of pages received, increasing responsiveness to pages, diminishing conflicts between staff members and improving communication.
Institutionally, this pilot was heralded by our executive leadership and Board of Trustees. Subsequently, these leaders mandated spread of the team training programme to all other disease centres at our main campus, into our four community satellites, across the paediatric service and, most recently, to critical interactions and handoffs between the ambulatory and inpatient oncology service. Few quality improvement initiatives in our organisation, or others, become the standard for the entire system.
This pilot project had several limitations. The project was conducted in a single disease group in a single comprehensive cancer centre, making the reproducibility of these experiences and results unclear. Dissemination of the best practices from this pilot to 11 other disease programmes in our centre is ongoing, motivated by the success in the BOC pilot and a subsequent mandate by senior leadership and the board of trustees. Despite improvements in patient and staff perceptions of teamwork, and the objective improvements in process measures that we observed, it remains challenging to demonstrate unequivocal benefits in clinical outcomes. Intuitively, improved teamwork has a positive effect on clinical care, but discerning a measurable difference in clinical outcomes is difficult, particularly when the frequency of the measured outcome of the intervention (serious medical errors) is very low at the outset. However, the improvements that we report in measurable outcomes over this short time period suggest that the risk of teamwork-related errors may continue to diminish over time. The project team continues to measure these outcomes, and in a larger group of providers and patients, as this programme is disseminated throughout our organisation. Refresher courses have been developed and implemented; a proposal for an instructional video on team behaviours at our institution was recently funded and is now in the planning phase.
Despite the stated limitations, there are few, if any, interventions so clearly associated with dramatic improvements in staff perception of benefit, particularly with regard to improving relationships and respect among coworkers. This outcome, in addition to the others observed, and the importance of preventing the potentially serious consequences of errors made in this setting make team training in outpatient specialty care a promising innovation that warrants further research and development.
Acknowledgments
The authors thank the Controlled Risk Insurance Company/Risk Management Foundation for its support of this pilot.
References
Footnotes
-
Contributors CAB: initiating project, designing trial, designing data collection tools, implementing trial, analysing data, drafting paper, revising paper, approving paper. The author is also a guarantor. AHG: initiating project, designing trial, designing data collection tools, analysing data, drafting paper, revising paper, approving paper. The author is also a guarantor. SNW: initiating project, designing data collection tools, writing the statistical plan, analysing data, drafting paper, revising paper, approving paper. The author is also a guarantor. MJK: designing data collection tools, monitoring data collection, analysing data, revising paper. The author is also a guarantor. AP, HJB, BF, NAH, CS, EEH, AEK, LC and EPW: implementing trial. SL: designing data collection tools, monitoring data collection. AHS: implementing trial, monitoring data collection. MS: designing trial. SM: designing trial, drafting paper, revising paper, approving paper. The author is also a guarantor.
-
Funding Controlled Risk Insurance Company/Risk Management Foundation CRICO/RMF provided funding for the physician/nurse consultant team that assisted us on this project.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.