Article Text

Abstract
Introduction This paper describes the evaluation of a 2-day simulation training programme for staff designed to improve teamwork and inpatient care and compassion in an older persons’ unit.
Objective The programme was designed to improve inpatient care for older people by using mixed modality simulation exercises to enhance teamwork and empathetic and compassionate care.
Methods Healthcare professionals took part in: (a) a 1-day human patient simulation course with six scenarios and (b) a 1-day ward-based simulation course involving five 1-h exercises with integrated debriefing. A mixed methods evaluation included observations of the programme, precourse and postcourse confidence rating scales and follow-up interviews with staff at 7–9 weeks post-training.
Results Observations showed enjoyment of the course but some anxiety and apprehension about the simulation environment. Staff self-confidence improved after human patient simulation (t=9; df=56; p<0.001) and ward-based exercises (t=9.3; df=76; p<0.001). Thematic analysis of interview data showed learning in teamwork and patient care. Participants thought that simulation had been beneficial for team practices such as calling for help and verbalising concerns and for improved interaction with patients.
Areas to address in future include widening participation across multi-disciplinary teams, enhancing post-training support and exploring further which aspects of the programme enhance compassion and care of older persons.
Conclusions The study demonstrated that simulation is an effective method for encouraging dignified care and compassion for older persons by teaching team skills and empathetic and sensitive communication with patients and relatives.
- Simulation
- Team training
- Patient-centred care
- Communication
Statistics from Altmetric.com
Introduction
This paper describes a 2-day simulation training programme for healthcare professionals to improve teamwork and the quality of care for older people.
Older people (65+) are the greatest users of health services accounting for 70% of hospital bed days,1 60% of hospital admissions, 80% of emergency readmissions and 80% of hospital deaths.2
Recently, a number of high profile investigations into the quality of care provided to older people in hospital have highlighted serious shortcomings.3 ,4 An editorial in the BMJ5 argued that to improve the quality of care for older people, deficits in specific knowledge, skills and attitudes of healthcare staff need to be addressed. Related concerns about the absence of specialised training in the care of older people in some medical and nursing curricula have been expressed elsewhere.6 ,7
Simulation training
Caring for older people requires specialist skills in dealing with their complex healthcare needs, including increased vulnerability to a range of problems, such as infections, falls, incontinence and adverse drug reactions, and in providing quality care despite high rates of sensory and cognitive deficits and multiple comorbidities.8 ,9 Simulation training has been suggested as a partial answer to this problem; it provides an immersive, dynamic environment in which learners can participate actively and practice skills in a risk-free environment.10
Simulation training in postqualification nursing and associated professions has been slow to develop compared with simulation in medicine.11 ,12 Its use in nursing has been most common in medical and anaesthesiology contexts and with undergraduate students rather than for continuing education.10 The few published evaluative studies of simulation training for nurses report mixed results; for example, some studies have found that students thought the training was beneficial but felt apprehensive or anxious during it.13 ,14 Others have found that students reported a positive and enjoyable experience,15 an increase in confidence,14 increased knowledge15 ,16 and increased knowledge but no change in confidence.17
There are relatively few reports of simulation for training skills in the care of older people despite recommendations that this is a powerful way for students to engage with the experience of their older patients.18 Evaluation of a continuing education programme incorporating simulation for the core competencies of geriatric nursing found that scores on measures of knowledge, perceived quality of the training, perceived skills gained and the relevance of the skills to the clinical setting increased from pretest to post-test.8 Recently, Liaw et al19 reported the development of a checklist for rating skill acquisition in simulation for detecting deteriorating older patients, indicating continuing developments in the application of simulation in this area.
Simulation for NTS
Recognition of the role that breakdowns in communication and teamwork play in patient safety incidents has led to simulation being increasingly used for non-technical skills (NTS) training, which has roots in Cognitive Task Analysis and Crew Resource Management techniques developed in aviation.20 Although NTS is a general term, its application in healthcare (and elsewhere) has tended to focus on features of cognitive performance such as situational awareness, planning and decision making.21 ,22 We argue that NTS should be defined more broadly in healthcare to include compassionate and empathic communication with patients. Skilled patient communication is as important for the quality of care (clinical effectiveness, patient safety and patient experience) as the skills usually defined as non-technical, and should be seen as critical NTS for nurses.
For older people, especially those with comorbidities, eliciting reports of concerns and changes is crucial as is empathetic nursing and maintaining patient dignity. Effective teamwork also requires highly developed communication skills. The value of simulation training for combining professional knowledge23 and raising inter-disciplinary awareness has been highlighted.24 It is, however, rare for members of the same team to train together, as is common in other industries such as aviation.25
Although Mitchell et al26 note the importance of social communication skills, there have been few reports of simulation being used specifically to enhance these, except in psychiatric nursing.27 We are not aware of previous studies specifically addressing compassionate care through NTS simulation training with debriefing to allow staff to explore the feelings and emotions associated with the quality and safety of care.
Modality
Different types of simulation used in healthcare include static part-task trainers, simulated patients (actors or standardised patients) and computer-enhanced manikins.28
Yaeger et al29 suggest a tripartite classification of simulation fidelity: low (skills practice in isolation), moderate (minimal cues to suspend disbelief) and high (immersive and hands-on). Importantly, assessments of relatively low fidelity simulators show effectiveness for the acquisition of nursing skills.30 Other important dimensions which affect learning are the environmental and psychological aspects of the simulation.31 The choice of simulation modality and fidelity should be underpinned by learning objectives32 and it should not be assumed a priori that high fidelity simulation will always be more effective than low or medium fidelity.33
A key principle in simulation is that learning is facilitated via construction of an active learning environment rather than simple delivery of content.34 ,35
Outcomes and sustainability
Theoretical models provide a systematic framework within which the various outcome measures can be identified, but few simulation studies have used a theoretically driven evaluation.28 ,36 Measured outcomes from simulation education or training can be qualitative36 ,37 but historically are more usually quantitative based on multiple choice questionnaires.31 Levett-Jones et al38 argue that multiple choice questionnaires are convenient to administer and relatively uncomplicated to analyse. Very few studies include longitudinal follow-up with participants after they have returned to practice and there is therefore little evidence about how the skills learned in simulation are integrated into clinical practice.28 Thus, questions remain about transfer to practice39 and the sustainability of knowledge over time40 and this has been a relatively neglected area of simulation research.28 ,41
Aims and objectives
This study evaluated the simulation training component of a comprehensive development programme (the PRO-CARE programme) incorporating different modules and teaching methods. The broad aim of the PRO-CARE programme was to improve the quality of care in a department of ageing and health consisting of three care wards.
The simulation aspect: (a) involved members of the inter-professional team; (b) used mixed modalities incorporating human patient simulation (HPS) in a high-fidelity simulation centre and ward-based simulation (WBS) exercises; (c) addressed empathetic and communication skills; and (d) evaluated independently using mixed methods including follow-up 7–9 weeks post-training. Specific learning objectives were to:
-
Increase the effectiveness of teamwork by improving communication skills
-
Increase patient-centred care, including sensitivity to privacy and dignity, by increasing participants’ understanding of how the ageing process impacts sensory, motor, cognitive and psychological functioning
-
Increase knowledge and skills for effective and empathetic communication with patients and relatives.
The Integrated Model of Training Evaluation and Effectiveness (IMTEE)42 was used to design the evaluation; the model identifies learners’ reactions, post-training self-efficacy, cognitive learning, training performance, transfer performance and organisational results as key outcomes.
Methods
Simulation training
This study took place in a tertiary hospital trust providing a range of specialist older persons’ services. An independent review of nursing in the older persons’ unit identified the need for a focus on continual improvement and more holistic, patient-centred care. The broader 2-week PRO-CARE programme, designed to meet these needs, involved closure of each of the unit's three wards in turn, allowing their inter-professional teams to attend dedicated simulation training days as a group (see the Discussion section). The simulation training consisted of a 1-day session in a fully equipped high fidelity simulation centre using HPS scenarios and a 1-day session of WBS using a mixture of role plays, exercises using part-task trainers and an ageing suit to simulate the experience of being older. Each day ran multiple times to accommodate all staff on the unit in groups of n=20–30.
The HPS course consisted of six scenarios (table 1) using a combination of manikins and actors over the course of a day. Each lasted approximately 15 min, followed by a 45 min facilitated debrief concentrating on NTS. Staff participated directly in at least one scenario and observed all other scenarios via video link so that everyone could contribute to each debrief. Debriefs were structured and consisted of a descriptive, analysis and application phase43 and were developed using previous guides.44 ,45 Discussions were facilitated by clinicians and trained professionals from the simulation centre and included a focus on reflective clinical practice.46
Description of 11 training modules using human patient simulation (HPS) scenarios and ward-based simulation (WBS) exercises
The WBS course consisted of five 1-h exercises with inter-professional involvement (see table 1). Scenarios and exercises were designed through inter-professional collaboration among senior nursing and medical staff, HPS specialists and educationalists. They were intended to cover a range of common acute and chronic issues and to allow the healthcare assistants (HCAs), nurses and physiotherapy staff to play a significant role before requiring medical input. Each exercise had an integrated debrief encouraging reflective practice and focusing on NTS.
The scenarios and exercises are shown in table 1.
Evaluation
The evaluation used mixed methods and was designed using the IMTEE to identify key outcome measures.42 Full ethical approval was obtained for the evaluation. Evaluation data consisted of observations, confidence ratings and interviews. Five observers from the research team rotated to directly observe simulated activities over 7 days in total. HPS observations included reviews of video/audio data from scenarios and debriefs. Observations were based on a pro forma adapted from key literature47 ,48 and involved notes on goals and objectives, resources used, participants, activities (role play; practical tasks; scripted scenarios) and within-session interactions (eg, emotional responses).
Simulation participants were given premodule and postmodule questionnaires using a 7-point rating scale to assess self-confidence on key competencies (eg, ‘communicating effectively with colleagues’; ‘identifying the needs of the older patient and their relatives’) with a reliability for nine items of α=0.95. All participants were approached for survey on a voluntary basis (table 2).
Number of participants in training and evaluation outcome measures by profession
Three trained interviewers conducted semistructured indepth interviews 7–9 weeks after the course to explore participants’ recall of the exercises, retained lessons and reflections on post course clinical practice.
Interviews addressed aspects of the broader PRO-CARE training programme, but interview schedules contained specific questions about simulation modules and their impact. Thematic data reported in this analysis relate directly to what staff reported about the HPS and WBS simulation. Sampling was purposive and interviewees were stratified to ensure representation across the professional groups (table 2).
Analysis
Observational data were gathered in note form and written to computer files.49 Interviews were analysed using thematic techniques50 using QSR NVivo data analysis software. A selection of eight interviews was independently cross-coded with code lists reaching 92% agreement; minor differences were discussed until consensus was reached. Confidence ratings data were analysed using SPSS V.19.0 (IBM, New York, USA).
Participants
Table 2 shows the numbers of participants who attended the training, the number who completed rating scales and the number of interviewees and their professional group.
Results
Observational strand
Analysis of fieldwork notes showed that the programme was in general well designed, delivered, facilitated and attended. Participants reported enjoyment of specific scenarios and exercises and were appreciative of the time and effort invested in them. Teaching was interactive and participant-centred with a variety of scenarios, role play exercises, practical activities and discussions.
Human patient simulation
Participants’ ability to engage in the HPS simulation scenarios was influenced by (a) how the scenario had unfolded and (b) the ability of those conducting debriefing to moderate discussions. Facilitating the debriefs to elicit cognitive learning was difficult when scenario participants’ clinical knowledge or skill had been challenged. Some people felt ‘under examination’ in terms of their clinical knowledge; others were wary of being seen to criticise their colleagues. The sessions worked best when scenarios had been handled well by the participants, allowing debrief participants to relax and discussions to focus on points aligned with the learning aims and objectives.
A few key observations can be made about ‘best practice’ during debrief sessions which can serve as a guide for ongoing work of this nature. Debriefs worked best when:
-
the purpose of debriefing was outlined from the outset
-
clinical points of interest were dealt with swiftly to enable a focus on the learning objectives
-
participants were encouraged to relate events to their own experience
-
different voices were encouraged but not to judge or criticise peers
-
time was allowed for a summary of key learning points at the end.
Ward-based simulation
Staff comments and reactions throughout the WBS exercises and at summary sessions indicated that the interactive and varied programme ‘on-the-ward’ helped them to maintain interest and enjoyment. The practical role play exercises allowed peers to construct their own meanings of events as they interacted and discussed the process. Participants said it had been good to get immediate feedback from actors and team members. Key learning points highlighted by debriefing included: how to communicate with relatives (welcome their perspective, gather information, be clear and calm, aim for resolution); being aware of individual differences and preferences in individual patients (treat patients as individuals); and appreciating the impact of ageing (physical, cognitive and social functioning).
Confidence ratings
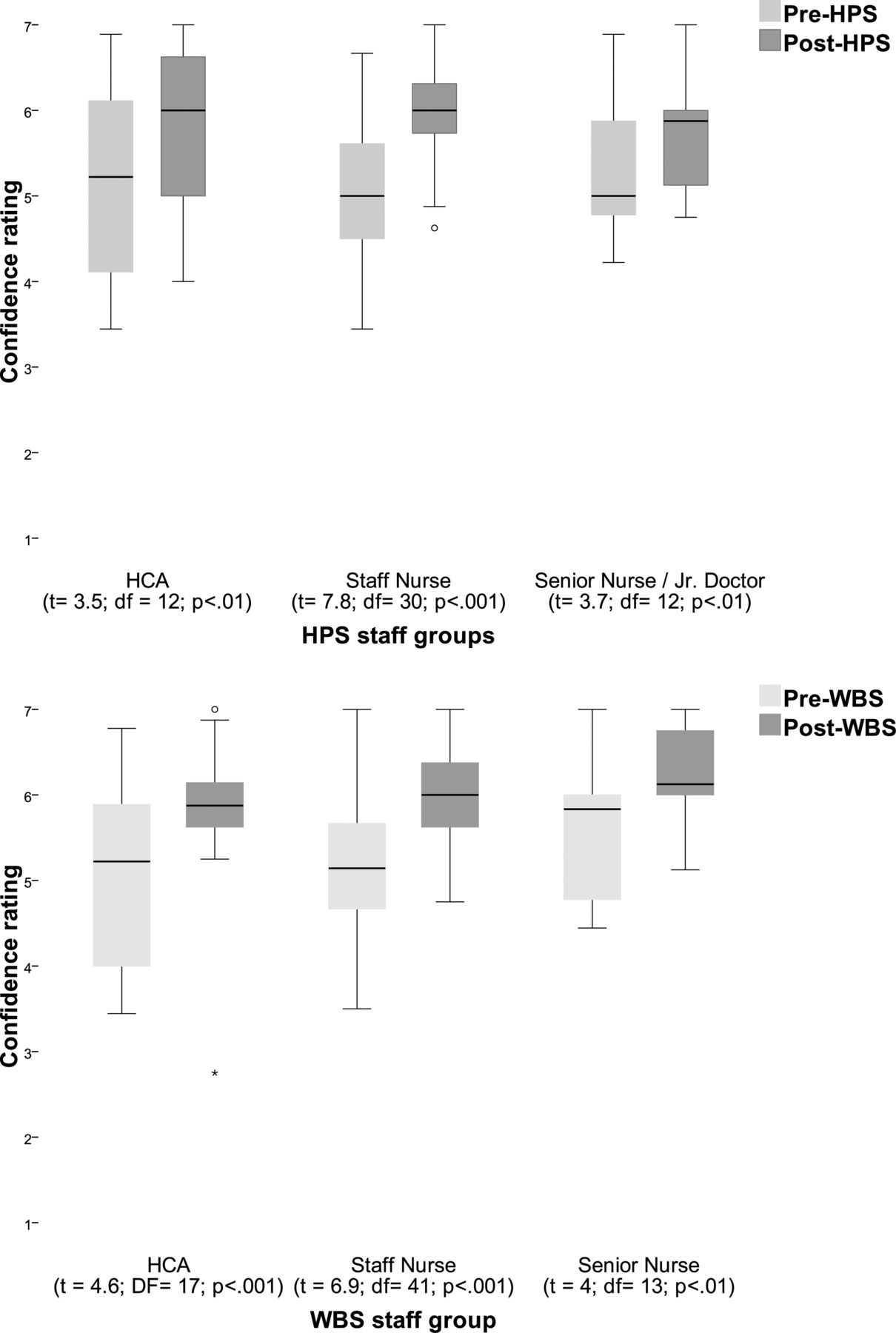
Figure 1 shows mean confidence (combined for all items) before and after the HPS and WBS scenarios by staff group.

{kind=link}
Mean and range confidence scores before and after training by staff group. HCA, healthcare assistant; HPS, human patient simulation; WBS, ward-based simulation.
For HPS (see top panel of figure 1), there was a broadly uniform baseline confidence score and a significant increase in confidence across all staff grades. There was one outlying score where a mid-grade nurse was lower than the 95th percentile after the course. Overall, mean confidence for all participants before the HPS sessions was 5.1 (SD 0.9) and mean confidence after was 5.92 (SD 0.7) which shows a significant increase (t=9; df=56; p<0.001; 95% CI 0.63 to 1).
For WBS (see lower panel of figure 1), there was a significant increase in mean confidence ratings for the whole group after the sessions (t=9.3; df=76; p<0.001; 95% CI 0.6 to 0.95). Mean confidence for all participants before the training was 5.2 (SD 0.88) and mean confidence after was 6 (SD 0.65). Individual t tests for each staff group also showed a significant increase in confidence. Three Allied Health Professionals (see table 2) are not included in figure 1 due to small numbers, but their mean scores increased from 4.5 to 6 after the course (t=7.2; df=2; p<0.05; 95% CI 0.6 to 2.3).
Interviews
Analysis of follow-up interview data showed that learning was centred on the two key themes of teamwork and patient care, including empathetic understanding and communication.
Teamwork
Participants reported that the course had increased role clarity between nurses and HCAs, lessening the tensions between working as a team and fulfilling individual responsibilities. The majority of participants reported feeling more able to raise concerns with senior staff and less likely to ‘keep quiet’ to avoid tension (some had spoken out before and found the experience difficult).
At follow-up, respondents reported that teamwork was strengthened via a clearer understanding of roles and boundaries and heightened awareness of the impact of their actions on others. Table 3 shows themes which emerged during analysis of teamwork data, illustrated by quotes from participants.
Teamwork themes and illustrations
Most participants thought the simulated exercises had been beneficial for practising such aspects of teamwork as calling for help, verbalising concerns and putting across particular points of view. HCAs in particular reported being empowered to raise concerns, communicate confidently and approach colleagues where necessary.
Caring
The main challenge before the course was finding time to communicate effectively with patients. Specific issues inhibiting communication included disagreements caused by the allocation of tasks and the confidence of specific nurses/HCAs in their own communication skills. Table 4 shows themes which emerged during analysis of patient care data, illustrated by quotes from participants.
Patient care themes and illustrations
Postcourse interviewees reflected on spending more time getting to know patients and how this enhanced the patient experience, and reported perceived clearer communication with patients and relatives and between team members.i
Finally, a number of challenges around sustainability were identified at interview. Staff turnover (and use of agency staff) could mean key messages were not sustained. In periods of high workload, the tension between being supportive to the team and performing one's own duties needed to be recognised and managed. Where the programme had encouraged junior staff to be open and challenge others, this needed clear guidance and support to maintain clear lines of supervision, leadership and accountability.
Discussion
This study evaluated whether the aims of an innovative simulation training programme for care teams were fulfilled. Innovative aspects of the study included: the use of simulation to train team working, patient/relative communication and empathetic and sensitive care; a theoretically based evaluation which included follow-up interviews 7–9 weeks post-training to investigate transfer into practice; and the closure of wards to facilitate the attendance of clinical teams who work together.
The mixed method evaluation was based on the IMTEE42 and thus evaluated a range of outcome measures. In summary, the precise findings from simulation training were:
-
Learners had strong positive emotional reactions to the course, but reported some anxiety and apprehension about the high fidelity simulation
-
Learners’ self-confidence on clinical competencies increased post-training
-
Knowledge for achieving better care was learned and retained at follow-up 7–9 weeks post-training.
These findings are in accord with previous studies that have identified nurse apprehension about high fidelity simulation13 ,14 and increased post-training self-efficacy among nurses exposed to high fidelity simulation.51
This study extends those of other studies of simulation in nursing by providing additional evidence that the knowledge acquired was retained at follow-up 7–9 weeks post-training and had positive effects on practice. The study shows that the skills required for communication and cooperation can be trained using simulation. NTS training for nurse education can be defined broadly to include team communication, patient interaction and empathy, in addition to traditional conceptualisations which emphasise cognitive skills such as situation awareness and decision making.21
Transference and sustaining compassionate care
Staff showed an emotional connection to the learning objectives and a renewed determination to communicate meaningfully with their patients (these findings are qualitative rather than experimental as tends to be the case elsewhere).52 This is an important step because high quality communication goes beyond the transmission and reception of information and becomes ‘real dialogue’.53 Compassionate care is at the core of the NHS constitution54 and championed by the Nursing and Midwifery Council and the General Medical Council, yet it has been argued that nursing training has become increasingly academic43 with a loss of core values such as compassionate care.55
In this study, the learning was reported to have had a positive effect on practice at follow-up 7–9 weeks post-training, in contrast to some studies which have shown deterioration in nurses’ simulation acquired knowledge at around 4–8 weeks,56 4 months57 and 6 months.58 However, we also found challenges in maintaining momentum, especially the need for postprogramme support from senior staff to maintain changes.
Debriefing and learning
We have reported that HPS debriefing can be challenging when scenarios are perceived to have been clinically problematic (with associated defensiveness about performance) and where junior team members may be wary of implied criticism of colleagues.
Meaningful learning requires the translation of simulated events to personal experience59 which must be facilitated by those conducting the sessions so that reflection can involve ‘honest self-assessment, open communication, and an understanding of how one's actions or decisions led to a particular outcome’.34 ,60
Effective debriefing must be robust enough to overcome the fact that scenarios rarely play out in exactly the same way and debriefs therefore have to allow for different ‘interpersonal communications, emotions or points of focus’, especially where, as in this case, staff at different levels are involved.61
Strengths and limitations
Inter-professional involvement
A strength of the study was that members of existing teams who provided care on each ward participated in the training together, including doctors, HCAs, nurses and allied health professionals. Although inter-professional training is often cited as an aim of simulation for NTS, in practice it is usually not practical for an existing team to participate in the training, which clearly presents challenges in forming a shared understanding of team goals and practices. In this study, the involvement of teams who work together had both positive and negative aspects. The fact that experiences and insights were shared during the training potentially contributed to the transfer of these skills into practice. However, the existing and ongoing personal relationships between team members may also have inhibited debriefing as participants were sensitive to team members’ feelings and the need to maintain good collegiate relationships.
A potential limitation was the lack of involvement of agency staff, students and limited involvement of junior doctors. Effective inter-professional working is likely to be enhanced by the involvement of the widest possible range of team members in training exercises.62
Evaluating the programme
The study had a number of methodological strengths, including independent, unbiased evaluators, the use of mixed quantitative and qualitative methods, and follow-up at 7–9 weeks post-training. The follow-up interviews, in providing an assessment of the effectiveness of the training from the staffs’ perspective, effectively extended the debrief period by inviting reflections on learning, the clinical validity of the simulation scenarios and practice, and how the learning had been implemented in practice. This opportunity for reflection allowed nurses to consider simulation outcomes in light of performance (rather than simply in light of simulation) and is a way of ensuring that the essential aspects of the clinical setting that shape practice, but are not necessarily represented in the simulation, are taken into account.63
The limitations of the methods included the absence of objective measures of performance during and post-training, and the lack of a control group which did not receive the training. The study was not able to include a control group because the aims of the PRO-CARE programme were to train all staff in the unit, but the before and after design, and the triangulation of the results using mixed methods provide reassurance that the results are robust. Reliance on nurses’ self-reports of the effects of the training is potentially subject to bias. Although methodologically challenging, future studies should develop objective measures of performance for NTS, including patient communication and empathy. Finally, the simulation training was part of the extensive, multi-faceted PRO-CARE programme. We took care to collect data about all aspects of the programme and have reported only the data relating to simulation in this paper, but it is difficult to isolate the effects of the simulation training alone.
In order to meet the demand of providing safe and high-quality care under tighter regulation of professional standards, the use of simulation training within nursing education will likely be increased64 ,65 and we need innovative ways of evaluating the effectiveness of what is in effect a complex intervention.66 This might, for example, involve creative use of ethnographic and qualitative methods to investigate in depth the role of simulation in the process of clinical skill acquisition.28 ,42
Finally, it is relatively rare for leadership in clinical institutions to release (and remunerate) entire clinical wings for inter-professional education. This study involved inter-professional teams attending dedicated simulation training days as a group, via closure of wards and use of temporary beds elsewhere. Costs in this case were justified on the basis of (a) using the periods to refurbish the unit, (b) projected reductions in major complaints and injurious falls and (c) increased patient and staff satisfaction.
Conclusions
This paper reports the results of an evaluation to examine the effectiveness of a novel, mixed fidelity, inter-professional simulation training programme. Although the study did not include a control group the design included mixed methods, the results of which were confirmatory, and before and after measures of confidence. Measures of learners’ reactions, post-training self-confidence and transfer of skills into practice showed that the programme had an overall positive effect with reported improvement in teamwork and communication, empathetic and sensitive communication with patients and relatives, and dignity and privacy in personal care. These results confirm the benefits of simulation training to improve the quality and safety of care for older people, and show that simulation can be used for training a broad range of non- technical nursing skills, including patient communication and empathy. This study indicates that there is scope for using different simulation modalities and a wide range of nursing scenarios to address skill deficits and improve teamwork. Although there are difficult logistical challenges in enabling whole teams to train together, this was an important aspect of the PRO-CARE programme, and these challenges need to be overcome if organisations wish to significantly improve care. As discussed above, the costs of the training need to be balanced against the organisational benefits and cost savings of increasing care quality. Potential solutions to the logistical difficulties include more frequent but shorter training sessions and the use of in situ simulation67 in which a simulated scenario is set up within the ward environment, thus enabling work to continue. Areas to address in future similar programmes include addressing learners’ anxiety about simulated tasks, widening inter-professional participation, ensuring post-training support and designing further metrics to show evidence of organisational improvement.
Longer term evaluation of the effects of the training is planned using hospital safety and patient satisfaction data.
Acknowledgments
Darlene Romero; Katrina Cooney; Elaine Gill; all participating staff and training programme facilitators.
References
Footnotes
-
Contributors HJ conducted the needs assessment and initiated the programme; PJ led the simulation design; SK and BT designed individual scenarios and exercises and facilitated the sessions; RS designed and oversaw aims and objectives for the care of older people; LT and PJ designed and led the debriefs; NK and KT designed interviews and led the qualitative analysis; JA and AR designed and led the evaluation and the quantitative analysis; AR wrote the first draft of the paper. All contributed to the writing of the final paper.
-
Funding This work was funded by Guy's and St Thomas’ NHS Foundation Trust (GSTT) and supported by the UK National Institute for Health Research (NIHR).
-
Disclaimer The views expressed in this publication are those of the authors and not necessarily those of GSTT, UK National Health Service, NIHR or the UK Department of Health.
-
Competing interests None.
-
Ethics approval King's College, London; SSHL/10/11-38.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
↵i Patient and carer/relative interviews (n=25) were conducted as part of the wider PRO-CARE study. Detailed analysis is beyond the scope of this paper as data did not necessarily relate to the simulation exercises. However, patients and carers/relatives broadly confirmed staff perceptions during the postsimulation period of improved team working and empathetic and compassionate communication.