Article Text

Abstract
Objective Computerised order sets have the potential to reduce clinical variation and improve patient safety but the effect is variable. We sought to evaluate the impact of changes to the design of an order set on the delivery of chlorhexidine mouthwash and hydroxyethyl starch (HES) to patients in the intensive care unit.
Methods The study was conducted at University Hospitals Bristol NHS Foundation Trust, UK. Our intensive care unit uses a clinical information system (CIS). All drugs and fluids are prescribed with the CIS and drug and fluid charts are stored within a database. Chlorhexidine mouthwash was added as a default prescription to the prescribing template in January 2010. HES was removed from the prescribing template in April 2009. Both interventions were available to prescribe manually throughout the study period. We conducted a database review of all patients eligible for each intervention before and after changes to the configuration of choices within the prescribing system.
Results 2231 ventilated patients were identified as appropriate for treatment with chlorhexidine, 591 before the intervention and 1640 after. 55.3% were prescribed chlorhexidine before the change and 90.4% after (p<0.001). 6199 patients were considered in the HES intervention, 2177 before the intervention and 4022 after. The mean volume of HES infused per patient fell from 630 mL to 20 mL after the change (p<0.001) and the percentage of patients receiving HES fell from 54.1% to 3.1% (p<0.001). These results were well sustained with time.
Conclusions The presentation of choices within an electronic prescribing system influenced the delivery of evidence-based interventions in a predictable way and the effect was well sustained. This approach has the potential to enhance the effectiveness of computerised order sets.
- Evidence-Based Medicine
- Cognitive Biases
- Implementation Science
- Critical Care
- Decision Support, Computerized
Statistics from Altmetric.com
- Evidence-Based Medicine
- Cognitive Biases
- Implementation Science
- Critical Care
- Decision Support, Computerized
Background
Computerised physician order sets have been in use for some time. Systematic reviews have shown that the use of order sets can lead to positive outcomes but high quality evidence of benefit is lacking.1 The design of these systems is not well studied and many are used with a configuration that may not be optimal for the implementation of desired interventions. One possible limitation of the effectiveness of order sets may be that they have not been designed with behavioural principles in mind.
In their influential book Nudge: improving decisions about health, wealth, and happiness,2 Thaler and Sunstein argue that better decisions are encouraged by providing clear and well-designed choices. The term ‘choice architecture’ describes the configuration of choices. A nudge is ‘any aspect of the choice architecture that alters behaviour in a predictable way without forbidding any options or changing economic incentives’.2 The use of nudges has shown promise in non-medical settings including savings for retirement3 and organ donation decisions4 but there are few studies that evaluate the impact of behavioural insights on routine clinical care.
Chlorhexidine mouthwash has been shown to reduce the rate of ventilator associated pneumonia in ventilated critically ill patients.5 It is a low cost intervention with widespread acceptance among clinicians. Hydroxyethyl starch (HES) is an intravenous fluid used to support the circulation. HES was found to be the most commonly used colloid for resuscitation on the intensive care unit (ICU) in an international survey published in 2010.6 There has been increasing concern regarding the safety of HES solutions for fluid resuscitation in intensive care patients in recent years culminating in two large randomised studies showing a higher rate of renal failure when using starch solutions compared with crystalloids.7 ,8
In this study, we sought to evaluate the impact of redesigning the choice architecture within an electronic prescribing system on the delivery of chlorhexidine mouthwash and HES in critically ill patients on the ICU at University Hospitals Bristol.
Methods
Setting
The study was conducted in a mixed medical and surgical ICU at University Hospitals Bristol NHS Foundation Trust, UK. This is a tertiary ICU with over 1200 admissions per year.
The ICU has used the ‘Innovian solution suite’ clinical information system (CIS), an electronic charting and prescribing system produced by Draeger (Germany), since 2007. In order to streamline junior doctors’ workflow, we have configured a prescribing template with some commonly used drugs and fluids preprescribed. Admitting doctors can choose to use the template when compiling the electronic drug chart at admission. They populate the final electronic drug chart by selecting which drugs from the template not to give (see figure 1).
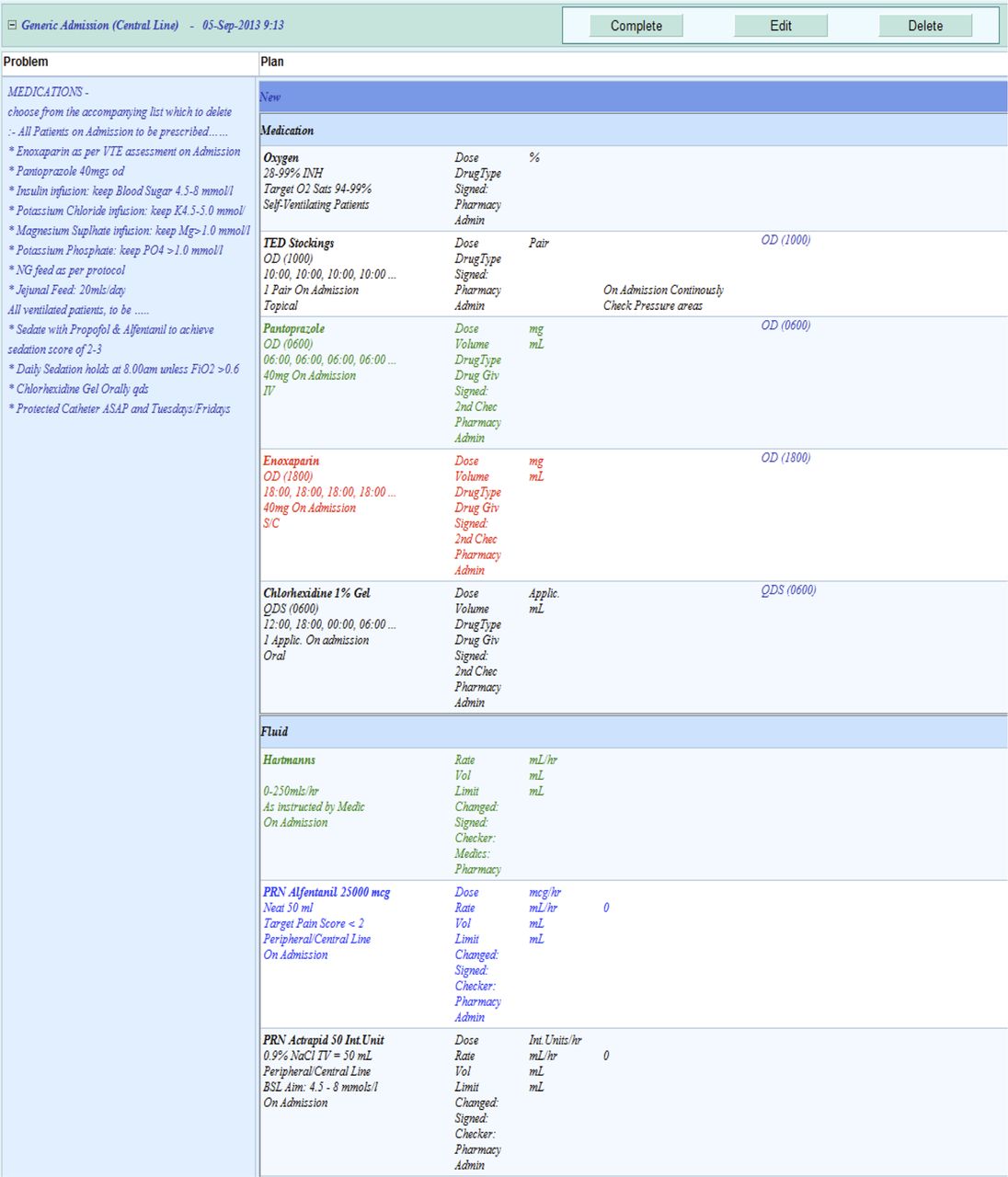
Screen shot showing the current prescribing template (after the change to chlorhexidine and fluid options). Note that prescribers are asked to delete from the list those interventions that are not required.
If the clinician chooses not to opt out of prescribing any of the drugs or fluids on the template, then all those drugs and fluids will populate the final drug chart and will be available for delivery to the patient. It is also possible to prescribe all the drugs and fluids contained on the template manually by selecting them from menus elsewhere on the electronic prescribing system but this involves more effort and time.
The drugs and fluids available from the template have been changed at several points over the last 5 years. Voluven 6% (a HES solution) was included on the template, alongside other fluid bolus options, from March 2007 to April 2009 (see figure 2). Unless physicians opted to remove Voluven 6% from the template, it would appear on the electronic drug chart to be delivered ‘as required’ on instruction from a physician as one of three options for fluid resuscitation.
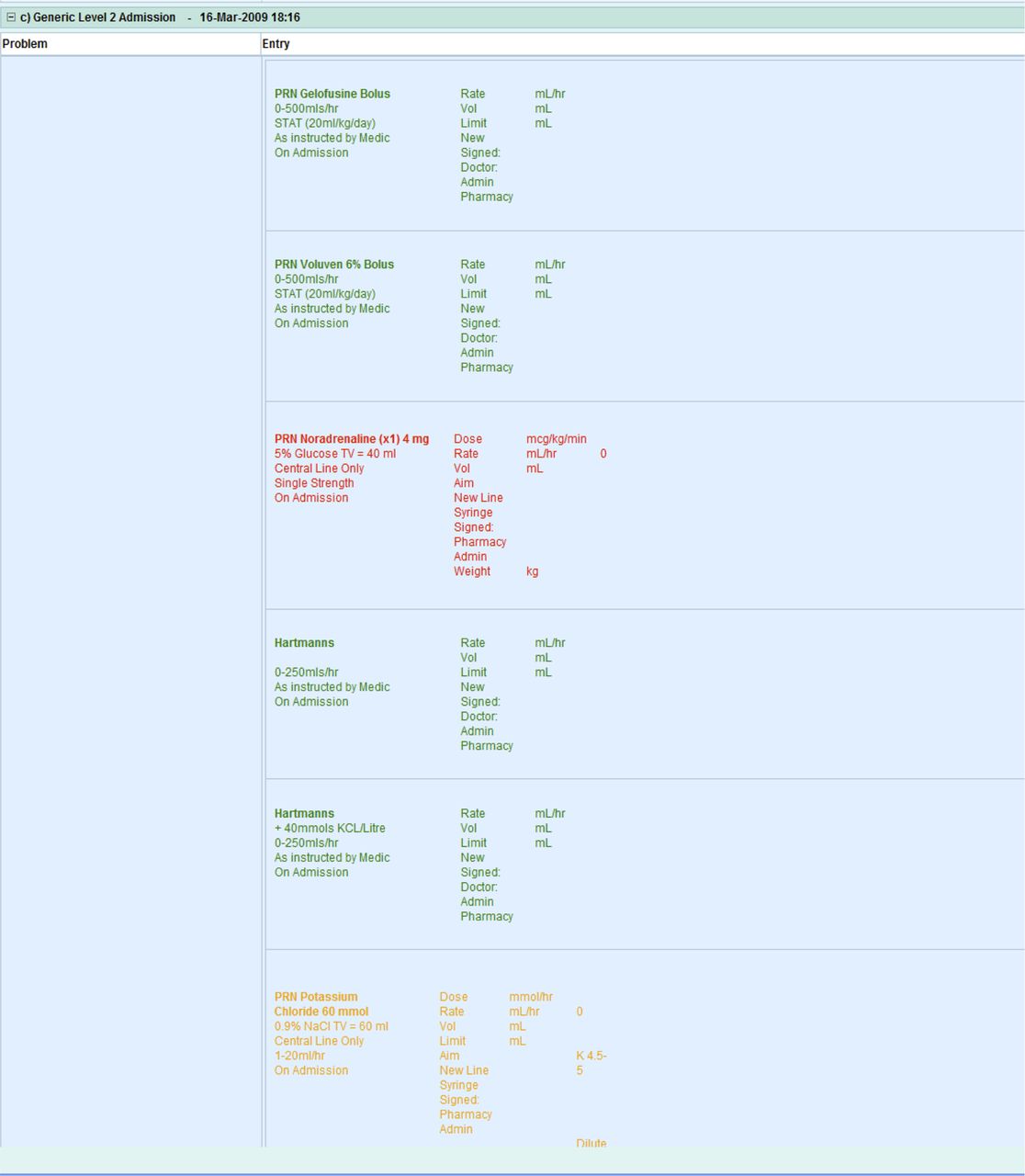
Screen shot showing the fluid section of the prescribing template prior to removing Voluven 6% as an option. Note the other aspects of the template, including the instruction to delete those interventions not required, are as shown in figure 1.
After April 2009, Voluven 6% could still be prescribed but this involved searching for it manually on the electronic system; it was no longer available as a default option alongside the other fluid bolus options on the template (see figure 1). At that time, there was insufficient professional consensus to completely remove HES from the prescribing system.
Chlorhexidine mouthwash has been available to prescribe manually since November 2008 (when it became possible to use the CIS to prescribe drugs) and it was added to the prescribing template as a default in January 2010 (see figure 1). Paper drug charts were used prior to November 2008 and this period was not included in the analysis. The use of chlorhexidine mouthwash four times per day has been included in our ventilator care bundle throughout the duration of this study.
We performed a retrospective before and after evaluation of the effect of these changes to default prescribing options on the delivery of each intervention. All data were gathered from our CIS database.
Patients and interventions
For the chlorhexidine group, we considered consecutive patients receiving positive pressure ventilation via an endotracheal tube or tracheostomy. Chlorhexidine mouthwash should be prescribed four times per day in a ventilated patient according to our ventilator care bundle. The intervention was considered as prescribed if it was present on the drug chart four times for each 24 h the patient was ventilated. Data from November 2008 to November 2012 were available for analysis. Chlorhexidine mouthwash was included on the prescribing template in January 2010. The ‘before change’ group was analysed as November 2008–December 2010 and the ‘after change’ group was analysed as February 2010–November 2012.
For the HES intervention we included all patients in the ICU. Voluven 6% was considered as delivered if it had been prescribed and documented as given on the electronic drug chart. The total volume of Voluven 6% infused was calculated each month. The total volume of HES delivered may be influenced by the number of patients on the ward, so we calculated an average volume delivered per patient in the ICU per month. We also collected data on how many patients each month actually received Voluven 6% and expressed this as a percentage of all patients on the unit each month. Data from March 2007 to September 2012 were available for analysis. Voluven 6% was removed from the prescription template in April 2009 for all new admissions. The ‘before change’ group was analysed as March 2007–March 2009 and the ‘after change’ group was analysed as May 2009–September 2012.
All data were anonymised prior to analysis. The institutional review board approved the study as a service evaluation and waived the requirement for ethical review.
Statistics
For the chlorhexidine intervention, Fisher's exact test was used to compare the proportion of eligible patients prescribed chlorhexidine before and after the intervention.
For the HES intervention, a two-tailed Student t test was used to compare mean volume of HES per patient per month before and after the intervention and Fisher's exact test used to compare the proportion of patients per month receiving HES.
Results
Chlorhexidine intervention
In total, 2231 ventilated patients were identified as appropriate for treatment with chlorhexidine, 591 before the intervention and 1640 after. Before the intervention, 327/591 (55.3%) patients were prescribed chlorhexidine; after the intervention, 1483/1640 (90.4%) were prescribed chlorhexidine; p<0.001 by Fisher's exact test (see table 1).
Preintervention and postintervention delivery of chlorhexidine mouthwash and hydroxyethyl starch (HES) solution
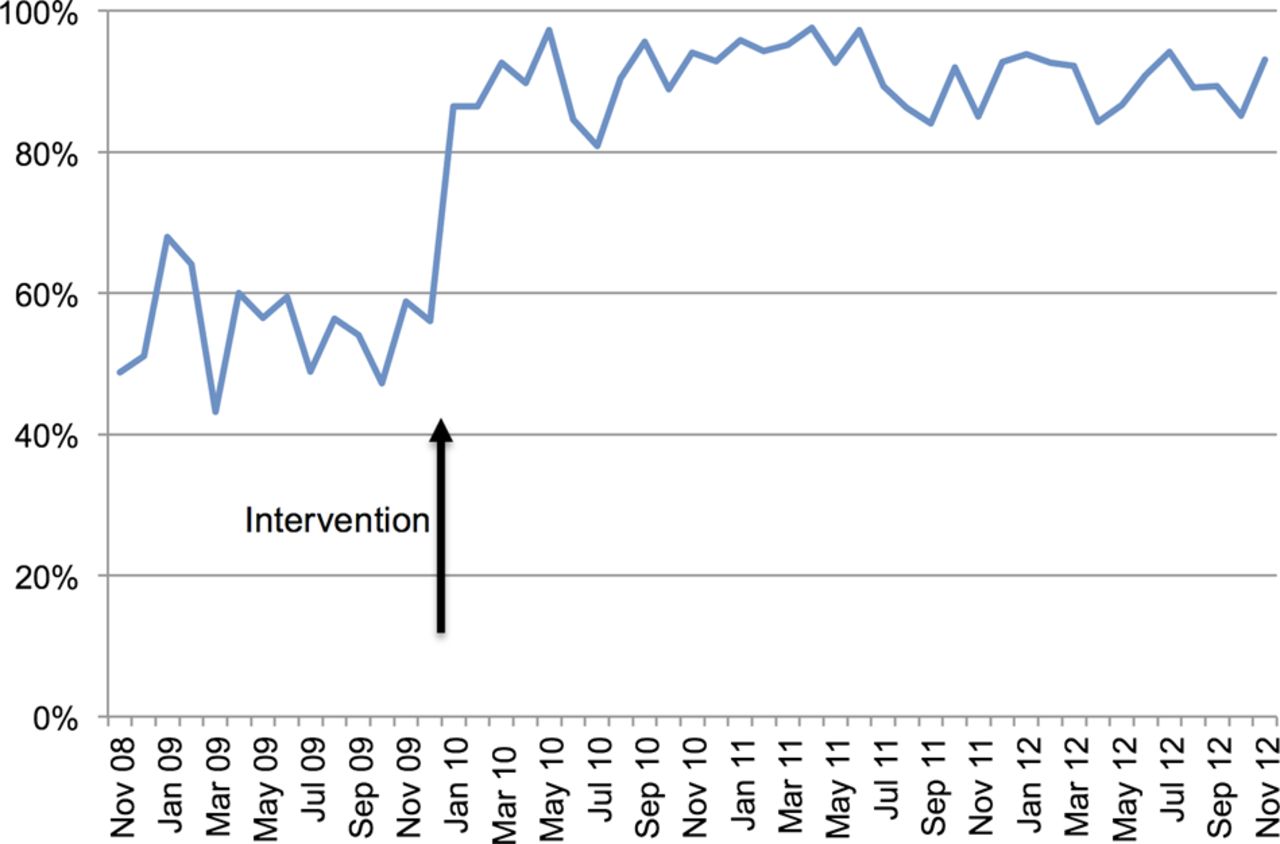
The increase in chlorhexidine prescription rate was well maintained with time (see figure 3).

Graph showing the percentage of eligible patients prescribed chlorhexidine mouthwash four times per day. The arrow indicates the inclusion of chlorhexidine on the prescribing template.
HES intervention
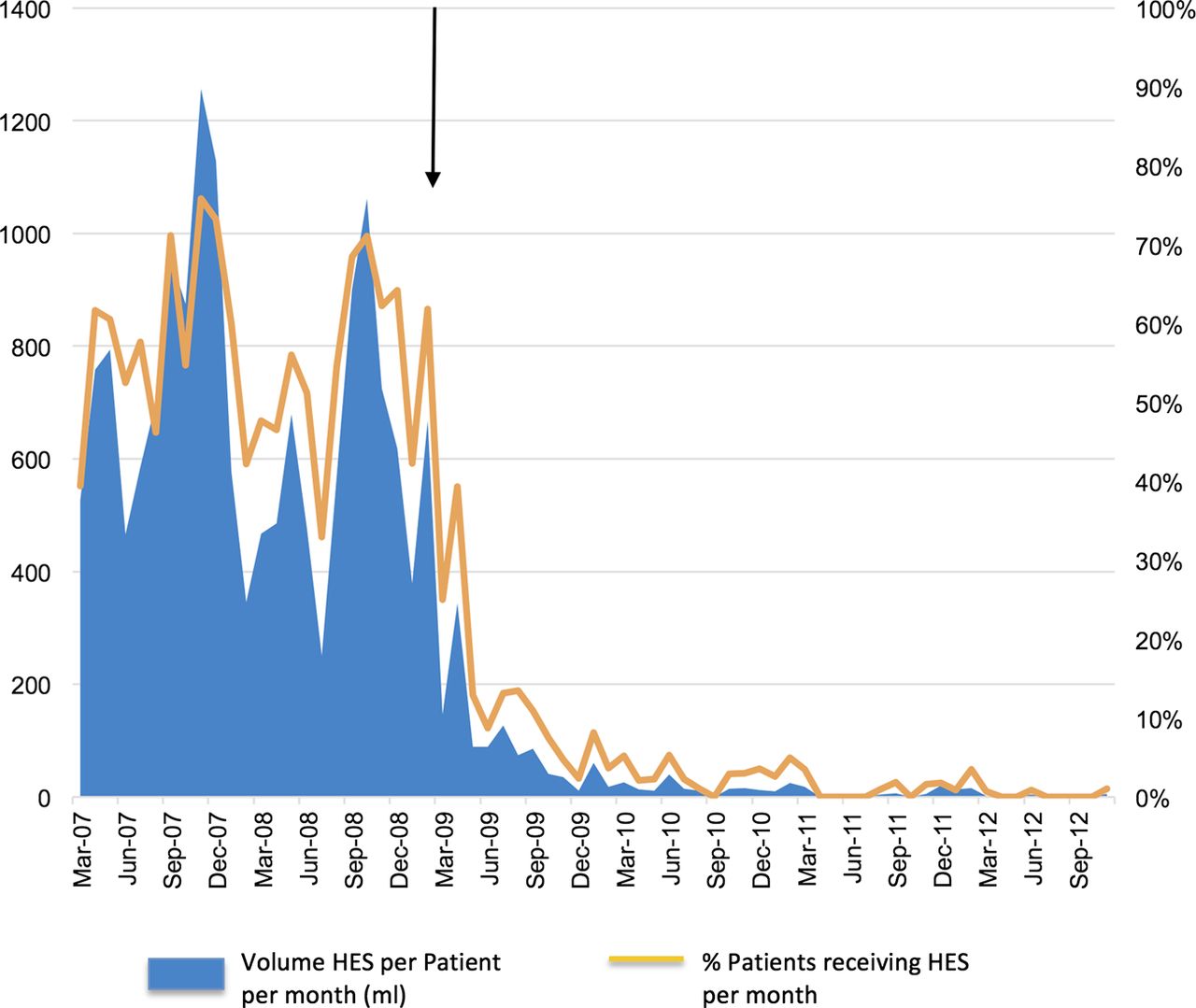
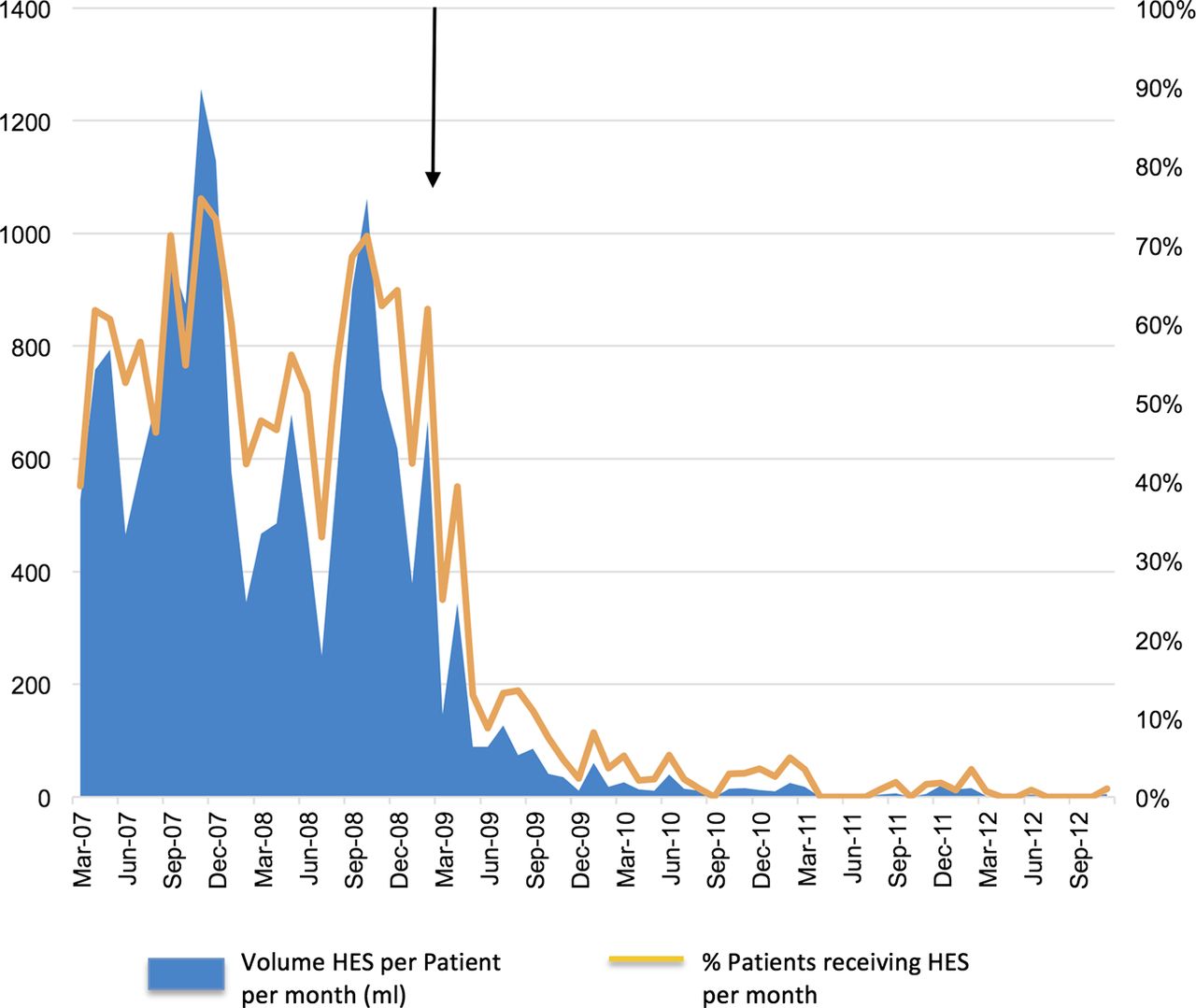
In total, 1453.76 L of HES were prescribed over the test period: 1371.51 L (630 mL/patient) before the intervention and 82.25 L (20.45 mL/patient) after the intervention; p<0.0001 by two-tailed Student t test. The percentage of patients receiving HES fell from 54.1% to 3.1%; p<0.001 by Fisher's exact test (see table 1).
The reduction in HES delivery was well maintained with time (see figure 4).
Discussion
This study demonstrates a highly significant increase in the reliability of delivered interventions after redesigning the choice architecture in a computerised order set to maximise benefit for patients. This was demonstrated for both a potentially beneficial and potentially harmful intervention and the effect was well maintained with time.
Chlorhexidine delivery was part of our ventilator care bundle throughout this study. Prescribing of chlorhexidine remained poor despite this until our intervention when there was a marked improvement (see figure 3). There were several attempts to change HES prescribing behaviour prior to removing it as an option in the prescribing template. These included a journal club and several consultant presentations on the potential harm of HES. It is interesting to note that HES use falls after the publication of a major study demonstrating harm in January 20089 but increases again shortly afterwards (see figure 4). Only when the option to deliver HES was removed from the template did use fall dramatically. Although HES appeared as a default on the template prior to the intervention, clinicians still had to make an active choice to deliver it as a fluid bolus when required.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Graph showing the delivery of hydroxyethyl starch (HES) solution to patients in the intensive care unit preintervention and postintervention. The arrow indicates the removal of Voluven 6% as an option on the prescribing template.
Delivering high quality, reliable and safe healthcare involves influencing the decisions that clinicians make and changing their behaviour. Traditional approaches often assume that clinicians behave as ‘rational actors’ by responding to information and acting on their preferences to maximise benefit for patients, but there is mounting evidence that clinicians can fail to act on their intentions: Lung protective ventilation is underused despite a documented intention to implement it.10 A survey of sedation practice in ventilated patients showed the underuse of evidence-based practice but importantly demonstrated that physicians intended to deploy it.11 A nationwide survey of adherence to recommended best practice guidelines in severe sepsis showed poor compliance, with clinicians perceiving compliance to be much higher than it actually was.12 Clearly, aiming to change clinicians’ intentions with new evidence, education and guidelines is not always effective in changing care at the bedside.
Computerised order sets have been used in hospitals for some time but high quality evidence of benefit is lacking.1 While it is known that the use of defaults can enhance the effectiveness of order sets,13 few studies have specifically evaluated this approach. Jacobs et al14 found that simple design changes including the use of defaults and changes to the framing of information significantly reduced variation in asthma care. The quantity, quality and cost of laboratory tests ordered at admission for a range of paediatric diseases was found to vary significantly depending on the availability of preselected order sets, including opt in and opt out options, in a theoretical model of an electronic health record.15
Policy makers in the UK have realised the importance of choice architecture in designing effective public policy.16 In healthcare, the use of behavioural insights has largely focused on the decisions made by the public in order to promote healthier lifestyles17 but the effectiveness of these interventions has been poorly evaluated.18 While there are many potential targets for this approach to modifying clinician behaviour, for example, configuring ventilators to deliver lower tidal volumes unless a clinician acts to change them, performing a daily sedation hold by default in ventilated intensive care patients or requiring antibiotics to be represcribed after a predetermined ‘stop date,’ there are very few clinical studies that directly examine the effect.
One randomised study demonstrated a significant change in sedation practice for routine endoscopy when the choices for the delivery of sedation were altered.19 Clinicians were presented with prefilled syringes of two different sizes containing the sedative midazolam and then instructed to use as much sedation as required. When smaller syringes were presented, the dose administered was significantly lower.
An important limitation of our study is that the interventions were not randomised and the before and after effects reported originate from one ICU. As with any before and after design, our results may be influenced by other unmeasured factors. The internal validity of the results may have been influenced by ongoing quality improvement efforts such as the ventilator care bundle and traditional attempts to reduce HES use. It would have been interesting to compare chlorhexidine and HES use with other ICUs over the same time period but this was outside the scope of this study.
HES use fell after the template change and this occurred well in advance of the publication of two large randomised studies demonstrating harm7 ,8 and so it is unlikely that an increased awareness of harm influenced the results.
We analysed all eligible care episodes over several years and included thousands of patients. By analysing the drug and fluid charts directly, the data in this study represent a very close approximation of the actual care delivered to our patients. Many quality improvement studies report intermittent sampling data gained from self-reported paper-based check lists that may overestimate compliance.
Conclusions
In this study, the delivery of evidence-based interventions was greatly enhanced after the application of behavioural insights to a computerised order set. This is approach has the potential to improve outcomes at minimal cost.20
Acknowledgments
We are very grateful to David Bryant and Anja DeBurgh-Williams who obtained the data used in this study.
References
Footnotes
-
Contributors CPB, MJCT, JSB and THG designed the study. CPB and KJD wrote the manuscript. KJD undertook the statistical analysis.
-
Competing interests None.
-
Ethics approval Institutional review board.
-
Patient consent The requirement for patient consent was waived by the institutional review board.
-
Provenance and peer review Not commissioned; externally peer reviewed.