Article Text

Abstract
Background Veteran suicides have increased despite mental health investments by the Veterans Health Administration (VHA).
Objective To examine relationships between suicide and acute inpatient psychiatric bed occupancy and other community, hospital and patient factors.
Methods Retrospective cohort study using administrative and publicly available data for contextual community factors. The study sample included all veterans enrolled in VHA primary care in 2011–2016 associated with 111 VHA hospitals with acute inpatient psychiatric units. Acute psychiatric bed occupancy, as a measure of access to care, was the main exposure of interest and was categorised by quarter as per cent occupied using thresholds of ≤85%, 85.1%–90%, 90.1%–95% and >95%. Hospital-level analyses were conducted using generalised linear mixed models with random intercepts for hospital, modelling number of suicides by quarter with a negative binomial distribution.
Results From 2011 to 2016, the national incidence of suicide among enrolled veterans increased from 39.7 to 41.6 per 100 000 person-years. VHA psychiatric bed occupancy decreased from a mean of 68.2% (IQR 56.5%–82.2%) to 65.4% (IQR 53.9%–79.9%). VHA hospitals with the highest occupancy (>95%) in a quarter compared with ≤85% had an adjusted incident rate ratio (IRR) for suicide of 1.10 (95% CI 1.01 to 1.19); no increased risk was observed for 85.1%–90% (IRR 0.96; 95% CI 0.89 to 1.03) or 90.1%–95% (IRR 0.96; 95% CI 0.89 to 1.04) compared with ≤85% occupancy. Of hospital and community variables, suicide risk was not associated with number of VHA or non-VHA psychiatric beds or amount spent on community mental health. Suicide risk increased by age categories, seasons, geographic regions and over time.
Conclusions High VHA hospital occupancy (>95%) was associated with a 10% increased suicide risk for veterans whereas absolute number of beds was not, suggesting occupancy is an important access measure. Future work should clarify optimal bed occupancy to meet acute psychiatric needs and ensure adequate bed distribution.
- mental health
- hospital medicine
- health policy
- report cards
Data availability statement
No data are available. All data are subject to the rules of availability assigned by the US Department of Veterans Affairs.
Statistics from Altmetric.com
Introduction
Suicide is the 10th leading cause of death in the USA. From 2005 to 2017, the age-adjusted suicide rate increased by 44%, with 43 390 adult suicide deaths occurring in 2017. Of these, 6139 (13.9%) were veterans, who are 22% more likely to die by suicide than age-matched and gender-matched non-veterans.1 Individual factors that increase suicide risk include financial or legal difficulties, physical or mental illnesses and access to firearms.2–5 Less is known about community and healthcare system factors that may be associated with suicide risk.
Inpatient psychiatric treatment is an important component of suicide prevention. Hospitalisation allows for identification and management of psychiatric and physical illnesses, coordination of care between providers and facilitation of access to support services, and provides time for personal or psychiatric crises to stabilise. However, despite the stable prevalence of many established suicide risk factors (eg, depression) and increasing incidence of suicide,6 there was a 25% reduction in the number of acute psychiatric beds per capita (from 28 to 21 beds per 100 000) in the USA from 2003 to 2016.7
While the optimal number of beds is unknown, a recommendation from the Treatment Advocacy Center is 40–60 public psychiatric beds per 100 000 as a minimum standard for reasonable psychiatric care in the USA.8 Prior work has sought to determine the relationship between the number of beds and population suicide rates. One study found that changes in suicide rates from 1999 to 2013 were not associated with the number of inpatient psychiatric beds or mental health spending at the state level.9 They theorised that per-capita bed availability may not be as important as how those beds are used with respect to treatment of acute psychiatric illnesses.
However, a shortage of beds leading to high occupancy rates may contribute to increased suicide risk among patients if it leads to higher thresholds for psychiatric admission or decreased thresholds for treating patients in other settings (eg, outpatient, community). For example, a patient with elevated suicide risk who presents to a Veterans Health Administration (VHA) emergency department (ED) may be admitted for inpatient psychiatry treatment when beds are available. Alternatively, if those beds are occupied or nearly occupied, that same patient may be discharged home, admitted to other inpatient wards with less psychiatric treatment expertise or transferred to community facilities with varying degrees of mental health resources or ability to coordinate with VHA services. News reports have identified that bed shortages may be associated with veteran suicides.10
High occupancy and a shortage of acute care treatment in EDs, intensive care units (ICU) and hospital wards have been referred to as ‘hospital strain’. A systematic literature review of 52 observational and experimental studies from 1999 to 2015 concluded that hospital strain is associated with increased mortality and worse health outcomes.11 These are complex relationships and the potential causal pathway may be very different for EDs12 13 and ICUs14 15 than acute psychiatric units.
The aim of this study was to examine the relationship between the incidence of veteran suicide and acute inpatient psychiatric bed availability using occupancy as a measure of hospital strain and community access. Our hypothesis was that acute psychiatric bed occupancy, rather than absolute number of beds, would be associated with risk of suicide at the hospital level.
Methods
Data sources
This is a longitudinal analysis with repeated measures testing the association between inpatient psychiatric bed occupancy at VHA hospitals with incidence of suicide among veterans enrolled in VHA care combining VHA administrative data with publicly available data. Veteran suicide, the primary outcome of interest, was obtained from the Department of Defense/VHA Suicide Data Repository in collaboration with the National Death Index (NDI).16 NDI data include all causes of death, regardless of where it occurs. Each death was assigned to the VHA hospital associated with the location where the patient received primary care since this is where they would be hospitalised if needed. Veteran clinical characteristics were obtained from the VHA Corporate Data Warehouse and aggregated at the hospital level. VHA hospital-level characteristics were collected from Veteran Support Services Center (VSSC), including total number of VHA psychiatric beds and occupancy reported for each month of observation and aggregated for each quarter. Community characteristics of non-VHA total acute psychiatric bed numbers and community mental health spending were gathered from the Area Health Resource File,17 US Census Bureau and American Community Survey18 and State Mental Health Agency spending reports.19 20 The Strengthening the Reporting of Observational Studies in Epidemiology statement checklist guided the reporting of our work.21
Study population
The study population included all veterans enrolled in VHA primary care for at least 1 year between 1 January 2011 and 31 December 2016, identified in VA Primary Care Management Module files. We used the VHA ‘market’, a geographical construct composed of US counties defined as ‘an aggregated geographic area having a sufficient population and geographic size to both benefit from the coordination and planning of health care services and to support a full healthcare delivery system (ie, primary, mental health, inpatient, tertiary, and long term care)’.22 This resulted in 111 unique geographic markets consisting of VHA hospitals with acute psychiatric beds across 50 US states. Each veteran was assigned to the VHA hospital located in the VHA market where they received primary care. Patients were considered at risk for the primary outcome (suicide) during their years enrolled in VHA, as this is a requirement to be admitted to one of the 111 VHA hospitals, resulting in a cohort of 6 714 439 veterans over 6 years.
Patient variables including age, race, gender, homelessness and rurality of residence (using rural-urban commuting area codes dichotomised into urban and rural) were aggregated to the hospital quarter.23 The proportion of patients with any mental health diagnoses was identified from outpatient and inpatient International Classification of Diseases Ninth Revision (ICD-9) and ICD-10 diagnosis codes in the prior year and included in the model. Community variables attributed to each VHA hospital market included non-VHA acute psychiatric beds, mental health spending and VHA hospital beds per capita.
Statistical analysis
The primary hospital-level exposure variable of interest was VHA inpatient acute psychiatric bed occupancy. Occupancy in each VHA hospital was reported as a percentage, and is calculated as the average daily census (ADC) over a given period divided by the number of available beds on the last day of a given period.
 .
.
For this analysis we used months, the smallest unit of time available in VSSC Bed Cube data. ADC was calculated as the fiscal year to date (FYTD) bed-days of care (BDOC) divided by the number of calendar days for the given period.

Because more than one patient can occupy a bed per day, it is possible for the ADC to be greater than the number of operating beds over a given period, and for occupancy to be greater than 100%. In such cases, occupancy was capped at 100%. The referent category of ≤85% occupancy was selected based on an established standard by the Royal College of Psychiatrists recommending occupancy of ≤85% to ensure ready access to local admission.24 Time, measured in quarters of a year, was included as a covariate in the models because of the known increased risk of suicide over time and seasonal suicide variation. With 111 hospitals over 6 years and four-quarters, there were a maximum total of 2664 hospital quarters included in the analysis.
All summary statistics were reported as either mean with SD for continuous variables or percentage and count for categorical variables. Hospital-level analyses modelled the relationship between hospital and market characteristics and suicide using a generalised linear mixed model. Suicide rate was modelled as number of suicides per quarter following a negative binomial distribution with a random intercept for each hospital and with the log of the quarter-specific count of unique veterans as an offset. An incident rate ratio (IRR) is reported, with a marginal effect25 calculated using recycled predictions with bootstrapped 95% CIs to report the number of additional suicides per quarter. All tests of significance used α=0.05. We calculated the E-value26 to quantify the minimum strength of association on the risk ratio scale that an unmeasured confounder would need to have with both the outcome (suicide) and exposure (occupancy), while simultaneously considering the measured covariates, to negate the observed outcome–exposure association. Authors had full access to and take responsibility for the data integrity. Analyses were conducted using SAS statistical software V.9.2 Proc Glimmix, R (R Foundation for Statistical Computing, Vienna, Austria; V.2.5.1) ggplot or Stata V.15 (StataCorp. 2017, College Station, Texas) margins.
Results
Of the 6 714 439 veterans enrolled in primary care in VHA between 2011 and 2016, a total of 13 273 (0.2%) died by suicide. Mean age of the study cohort was 65.0 years; 71.6% were White; 92.3% were male; and 33.0% resided in rural areas (table 1). During the study period, the number of deaths by suicide increased from 2193 in 2011 to 2464 in 2016. Accounting for the increased number of veterans enrolled in primary care, the national incidence of suicide among enrolled veterans increased from 39.7 to 41.6 per 100 000 person-years, or a 4.8% increase. Across the 111 VHA hospitals with inpatient psychiatric beds, the incidence of suicide for any given quarter ranged from 0 to 53.4 per 100 000 enrolled veterans.
Sociodemographic characteristics included in statistical models
The absolute number of acute VHA inpatient psychiatric beds decreased by 12.6% from 4419 in 2011 to 3860 in 2016. When normalised to the enrolled veteran population, the VHA national average across all 111 VHA hospitals decreased by 18.7% from 80.6 in 2011 to 65.5 per 100 000 enrolled veterans in 2016. Mean psychiatric bed occupancy measured by quarter decreased by 2.8% from 68.2% (IQR 56.5%–82.2%) in 2011 to 65.4% (IQR 53.9%–79.9%) in 2016. Of the 2664 hospital quarters of observation over the 6-year period, 2150 (80.7%) had a mean occupancy ≤85%, 182 (6.8%) had an occupancy of 85%–90%, 152 (5.7%) were 90%–95%, 145 (5.4%) were ≥95% and 35 (1.3%) were missing. Distribution of occupancy by hospital is displayed in figure 1A.
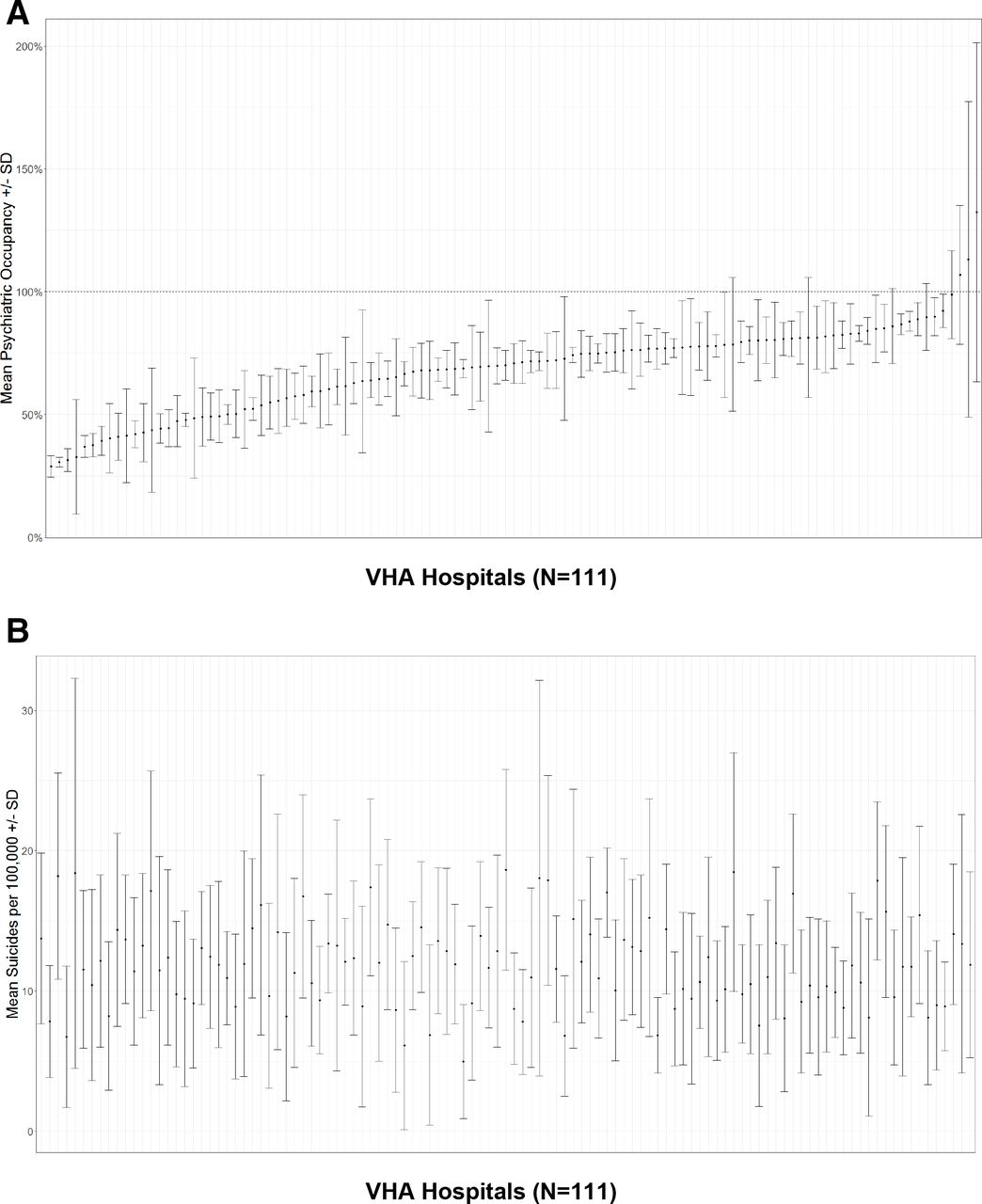
(A) Mean and SD for acute psychiatric bed occupancy percentage by Veterans Health Administration (VHA) hospitals (2011–2016). VHA hospitals (n=111). (B) Mean and SD for suicides/100 000 by VHA hospitals (2011–2016) corresponding to (A). VHA hospitals (n=111).
Compared with VHA hospitals with an acute psychiatric bed occupancy of ≤85%, the IRR of suicide for hospitals with occupancy ≥95% was 1.10 (95% CI 1.01 to 1.19) (figure 2). This is an estimated marginal effect of 0.45 additional suicides (95% CI 0.01 to 0.88) per quarter or 1.78 per year. The IRR was not significantly different for acute psychiatric bed occupancy of 85.1%–90% (IRR 0.96; 95% CI 0.89 to 1.04) or an occupancy of 90.1%–95% (IRR 0.96; 95% CI 0.89 to 1.05) compared with occupancy ≤85%. Lower suicide risk was observed for each 5% increase in Black veterans (IRR 0.95; 95% CI 0.93 to 0.97) served by the hospital. Higher suicide risk was observed for veterans aged 45–54 and 55–64 relative to age <35. Across the nine US Census Bureau divisions, we observed higher incidence rates in the Mountain, Pacific, West South Central, East South Central and South Atlantic compared with New England. Suicide increased over time and was highest in spring and summer compared with winter. Changes in VHA psychiatric beds, non-VHA (ie, community) psychiatric beds, spending on community mental health per capita and proportion of veterans with a mental health diagnosis at the healthcare facility were not associated with the incidence of suicide among veterans enrolled in VHA care.

{kind=link}
{kind=link}
Incident rate ratio (IRR) of suicide risk at the hospital level modelled against occupancy adjusting for population and community covariates, US Census Division and time (2011–2016). Population covariates=black race, mental health diagnoses, homelessness, age, rurality and US Census Division. Community covariates=Veterans Health Administration (VHA) and non-VHA psychiatric beds, State Mental Health Agency (SMHA) spending.
Discussion
In a national study of 6.7 million veterans engaged in primary care in VHA, acute psychiatric bed occupancy (>95%), and not beds per capita, was associated with a 10% higher incidence of death by suicide. Extrapolated over the 6-year study period across the 145 hospital quarters with occupancy >95%, this hospital strain contributed an estimated excess of 64.5 suicides. Unlike prior studies suggesting an inverse relationship between suicide and absolute number of hospital beds per capita,9 27 28 we observed that when controlling for the number of VHA and non-VHA hospital beds, hospital occupancy was independently associated with suicide. This relationship is clinically plausible because EDs and mental health professionals may make different decisions on whether to admit a patient for suicidal ideation or other mental health diagnosis depending on inpatient psychiatric bed availability. Ideally, hospital admission should be independent of bed availability, but the decision is subjective and often voluntary. If a bed is not available, a patient may be discharged home, admitted to a non-psychiatric unit or transferred to another hospital. In that instance, suicide may not necessarily be prevented during hospitalisation,29 but the hospitalisation may have been an opportunity to reduce the risk for suicide through coordination of intensive outpatient psychiatric care after discharge.
The reduction in number of acute psychiatric beds in VHA over the study period should be interpreted in the context of bed use, non-VHA standards and prevalence of psychiatric bed availability. The higher per-capita rate of psychiatric beds in VHA (80.6/100 000 in 2011) likely reflected many unused beds. If a 20-bed unit is only occupied at 50% capacity, then the additional 10 beds are of little value in that market region. In terms of absolute bed numbers, the VHA national average of 65.5/100 000 veterans in 2016 is still three times the US national average of 22/100 000, closer to the Organisation for Economic Co-operation and Development average of 71/100 000, and above the UK’s National Health Service recommended 50/100 000.24 Ultimately, demand for beds is affected by market forces, seasonal variation, pandemics, outpatient mental health services and other public health emergencies. The number of beds is dependent on multiple factors including a fixed amount of physical space and equipment, regulated numbers of hospital beds and adequate physician, nurse and support staff.
Community (ie, geographic market surrounding VHA hospitals) factors of non-VHA psychiatric beds and per-capita spending on mental health were not associated with risk of veteran suicide. Because veterans enrolled in primary care have access to colocated mental health services through primary care mental health integration programmes30 31 and have been shown to have a high reliance on VHA for mental health services,32 it is not surprising that these factors were not associated with suicide risk. Regardless, VHA does coordinate with community care through the CHOICE and MISSION Acts for mental health services.33
Regional differences in suicide risk were adjusted for in the model and consistent with prior studies34 with the greatest risk in the Mountain and Pacific Census divisions. Suicide risk also increased over the study period, in spring and summer months, and in veterans aged 45–64, all of which have been previously reported.1 3 35 Black race was associated with a lower risk of suicide, consistent with prior studies.36
Most prior work has attempted to identify individual patient risk factors for intervention, while hospital or system-level factors may have a significant potential impact on reducing suicide rates. VHA has invested considerably in mental health and suicide prevention through suicide hotlines, mental health staffing ratio targets, integration of mental health into all primary care points of care, community outreach programmes and evidence-based prediction models.37–39 Further evaluation of hospital occupancy and ensuring adequate number of beds to meet regional demand may be another avenue for intervention.
The findings should be interpreted with the following limitations. The veteran population is different than the general population in numerous ways and thus might not be generalisable. One important factor is familiarity with firearms, but firearm ownership data are not available to include in the analysis and this relationship is complex.40 Occupancy calculations were made on a monthly basis and aggregated at the quarter due to low number of suicides in smaller units of time, potentially limiting the precision of the analysis. Regardless, healthcare systems that experience high rates of hospital occupancy should develop more precise measures of occupancy to monitor this potential risk factor. Only veterans actively engaged in VHA primary care were included. Since not all the roughly 20 million US veterans are enrolled or eligible for VHA healthcare, we limited our cohort to those receiving care and thus able to be admitted to VHA hospitals. Nurse staffing data were not available and nursing shortages can result in temporary closure of inpatient beds. The exact timing of a suicide was not linked to a precise potential lost opportunity for admission. There is a potential for unmeasured confounding. Based on the E-value, we estimate that the magnitude of association, on the risk ratio scale, between an unmeasured confounder and both suicide and high inpatient occupancy would need to be greater than 1.43 to negate these results. Of the covariates, only US Census Division had IRRs >1.43 (Mountain (1.95), Pacific (1.53) and West South Central regions (1.53)), with most being less than 1.1, suggesting it would take a strongly associated unmeasured confounder to negate the observed results. Finally, the data only go through 2016, the last year available at the time of the analysis.
In conclusion, hospital occupancy, not the number of hospital beds per capita, appears to be a potential risk factor for veteran suicide. Measuring hospital occupancy and establishing occupancy benchmarks should be included in patient safety reports as psychiatric bed overcrowding joins overall hospital,11 ED12 and ICU14 occupancy as a risk for higher mortality. Future work should consider regional variation and identification of potential high-risk populations or regions who may benefit from greater investment in mental health services with the aim of preventing suicide.
Data availability statement
No data are available. All data are subject to the rules of availability assigned by the US Department of Veterans Affairs.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Institutional Review Board and the Research and Development Committee.
References
Footnotes
Contributors All authors contributed to the planning, conduct and reporting of the work presented. PJK is responsible for the overall content as guarantor. Planning: PJK, MBH, RT. Conduct: PJK, NMM, MRA, BH, MPJ. Reporting: PJK, MRA, BH, NMM, MBH, MBJ, RT.
Funding This material is based on work supported (or supported in part) by the Department of Veterans Affairs, Veterans Health Administration, VA Office of Rural Health and the Office of Research and Development, and Health Services Research and Development (HSR&D) Service through the Comprehensive Access and Delivery Research and Evaluation (CADRE) Center (CIN 13-412).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.