Article Text

Abstract
The objective of this study was to evaluate the impact of quality improvement (QI) and patient safety initiatives and data disaggregation on racial disparities in severe maternal morbidity from hemorrhage (SMM-H).
Our hospital began monitoring and reporting on SMM-overall and SMM-H rates in 2018 using administrative data. In March 2019, we began stratifying data by race and ethnicity and noted a disparity in rates, with non-Hispanic Black women having the highest SMM rates. The data was presented as run charts at monthly department meetings. During this time, our hospital implemented several QI and patient safety initiatives around obstetric hemorrhage and used the stratified data to inform guideline development to reduce racial disparity. The initiatives included implementation of a hemorrhage patient safety bundle and in-depth case reviews of adverse patient outcomes with a health equity focus. We then retrospectively analyzed our data. Our outcome of interest was SMM-H prior to data stratification (pre-intervention: June 2018-February 2019) as compared to after data stratification (post-intervention: March 2019-June 2020).
During our study time period, there were 13,659 deliveries: 37% Hispanic, 35% White, 20% Black, 7% Asian and 1% Other. Pre-intervention, there was a statistically significant difference between Black and White women for SMM-H rates (p<0.001). This disparity was no longer significant post-intervention (p=0.138). The rate of SMM-H in Black women decreased from 45.5% to 31.6% (p=0.011).
Our findings suggest that QI and patient safety efforts that incorporate race and ethnicity data stratification to identify disparities and use the information to target interventions have the potential to reduce disparities in SMM.
- healthcare quality improvement
- obstetrics and gynecology
- patient safety
- quality improvement
- quality measurement
Data availability statement
No data are available. not applicable.
Statistics from Altmetric.com
- healthcare quality improvement
- obstetrics and gynecology
- patient safety
- quality improvement
- quality measurement
Introduction
Persistent racial and ethnic disparities in maternal mortality and morbidity exist in the USA. Compared with white women, black women are 3–4 times more likely to die during childbirth and have twice the risk of severe maternal morbidity (SMM).1 2 Non-Hispanic (NH) black women have had the fastest rate of increase in maternal deaths between 2007 and 2014 and have higher case-fatality rates from a range of conditions, although the leading causes of maternal death for black and white women are similar.3
SMM is much more common than maternal death, with nearly 100 cases of SMM for every death.4 SMM can be thought of as the unintended outcomes of the process of labour and delivery that result in significant short-term or long-term consequences to a woman’s health.5 To identify delivery hospitalisations with SMM, the Centers for Disease Control (CDC) developed a composite measure that uses administrative hospital discharge data and International Classification of Diseases (ICD) diagnosis and procedure codes, reflecting major complications in childbirth.6 The most common indicator of SMM, as defined by the CDC, is receipt of a blood transfusion of any product and/or amount, which has largely driven the increase in SMM over the years.7 Haemorrhage is the most common serious complication of childbirth8 and a leading cause of death on the day of delivery and during the first 6 days post partum.9 A significant proportion of SMM and mortality events are preventable, with haemorrhage being associated with the highest rate of preventability.10 Preventability of these events may be even higher among black women than white women, with improved quality of care often being considered the most important factor in prevention.11
In 2013, Texas established a Maternal Mortality and Morbidity Task Force to address the rising maternal mortality rate12 and began reviewing cases of maternal deaths in 2015. The 2018 Texas Maternal Mortality and Morbidity Task Force and Department of State Health Services (DSHS) Joint Biennial Report reported on the finding that black women were affected by pregnancy-related death more than any other race or ethnicity and that the pregnancy-related mortality rate for NH-black women was 2.3 times higher than the rate for NH-white women (13.9 vs 6.0 per 100 000 live births).13 Consistent with nationally reported morbidity and mortality data, the increased risk for maternal death among black women was present regardless of income, education, marital status or other health factors. Additionally, black women in Texas were also at higher risk of SMM involving haemorrhage.13 The Task Force found a number of provider and facility factors associated with maternal death, including failure to recognise risk status, delays in diagnosis and delays in implementation of appropriate treatment.13 As a result, the Texas DSHS launched a statewide initiative to implement the Alliance for Innovation on Maternal Health (AIM) Obstetric Haemorrhage patient safety bundle14 in 2018 and invited all Texas birthing hospitals to participate, referred to throughout the rest of the document as TexasAIM. AIM is a national data-driven maternal safety and quality improvement (QI) initiative that works to reduce preventable maternal mortality and severe morbidity across the USA. AIM works through state and community-based teams to align national-level, state-level and hospital-level QI efforts to improve overall maternal health outcomes.15
Our hospital, a not-for-profit academic affiliate with both private and academic obstetric practices, enrolled and participated in the TexasAIM obstetric haemorrhage learning collaborative. While implementing the AIM obstetric haemorrhage bundle, our hospital also decided to incorporate elements of the AIM safety bundle on reduction of peripartum racial and ethnic disparities16 to identify and eliminate any disparities in care that may exist in our hospital from haemorrhage. We used the framework set forth by the Institute for Healthcare Improvement (IHI) to guide our work. The IHI notes that a health equity improvement strategy requires data collection and stratification by race, ethnicity and language (REaL) to identify inequities, help set priorities and drive improvement activities.17 18 Our project aimed to evaluate the impact of a haemorrhage QI and patient safety initiative along with data disaggregation on racial disparities in SMM from haemorrhage.
Materials and methods
We report on our study design, data analysis and outcomes following the Standards for Quality Improvement Reporting Excellence 2.0 .19 Our hospital is a level IV maternal and neonatal hospital located in an urban medical centre. This designation is assigned by the Texas DSHS and indicates that our hospital provides the highest level of comprehensive care for pregnant and postpartum patients.20 With an annual delivery volume of approximately 6500 births, our hospital is staffed by both academic and private practice obstetric providers and certified nurse midwives and supports the training of one of the largest US obstetrics and gynaecology residency programmes.
Hospital gap analysis of obstetric haemorrhage patient safety bundle
The TexasAIM quality collaborative followed the IHI learning collaborative model in which three regional in-person learning sessions were held with intervening virtual action period calls.21 Our hospital participated in the Houston, Texas regional cohort and the first in-person learning collaborative was held in December 2018. Each hospital assembled an AIM team of five to six members to attend these sessions. Our team consisted of a physician clinical leader, who was also the hospital’s Chief Quality Officer for Obstetrics and Gynaecology and principal investigator of this study; a nurse clinical leader, who was also the hospital’s Associate Director for Labour and Delivery and Obstetric triage; a data specialist and two quality and safety specialists. A key focus of the first learning session was to perform a gap analysis of the AIM obstetric haemorrhage bundle. The AIM bundles are divided into four domains: readiness, recognition and prevention, response and reporting and systems learning. Each domain consists of a series of recommended bundle elements. For each bundle element, the gap analysis assessed whether it was in place and consistently executed at our hospital; in place and not working or not in place. Within this analysis, our team determined the gaps between our hospital’s practices and the bundle (online supplemental appendix 1). We identified seven bundle elements that either needed to be enhanced because they were in place and not currently working or needed to be developed and implemented because they were not in place at all. They included: (1) assessment of haemorrhage risk; (2) quantitative blood loss (QBL) measurement (ie, the use of weighing and blood collection devices to determine the actual amount of blood loss rather than a visual estimation); (3) unit education on protocols and unit-based drills with postdrill debriefs; (4) active management of the third stage of labour; (5) postevent debriefs to identify successes and opportunities; (6) multidisciplinary review of serious haemorrhages for systems issues and (7) support programme for patients, families and staff for all significant haemorrhages.
Supplemental material
Hospital Obstetric Haemorrhage Committee
Following the first learning collaborative session and gap analysis, our hospital AIM team then organised a hospital AIM Obstetric Haemorrhage Committee comprising workgroups for each bundle element requiring enhancement or development and implementation with a paired physician and nurse lead of each group. The AIM hospital physician and nurse clinical leader participated in each workgroup, assisting with resources and references and a timeline guide. Workgroups were encouraged to recruit additional members as appropriate. Workgroup meeting frequency was determined and scheduled by team leads, with a suggestion of at least every 2 weeks. The full AIM Obstetric Haemorrhage Committee met monthly, with each workgroup providing an update about progress, successes and barriers. Updates were shared at monthly hospital department meetings with all hospital providers and nurse leaders.
Quality measures
TexasAIM provided defined structure, process and outcome measures at the beginning of the collaborative. Hospitals were asked to submit structure and process data monthly, however TexasAIM was going to provide the outcome data. Prior to the first learning collaborative, DSHS provided participating AIM hospitals with their SMM data from recent years, both overall and from haemorrhage, based on hospital administrative data. The TexasAIM outcome measure was the SMM rate from haemorrhage (SMM-H), using definitions as defined by the CDC,6 with a goal of a 25% reduction. At the time, our hospital was not reporting on SMM data, so our quality team decided to abandon our internal composite quality measure and adopt reporting on overall SMM and SMM-H to have state and national comparisons and benchmarks.
The list of 21 indicators and corresponding ICD codes used to identify delivery hospitalisations with SMM can be used to track SMM when using administrative hospital discharge data from October 2015 and beyond.22 For overall SMM, the denominator is delivery admissions as defined by delivery procedure and diagnosis codes and excludes abortive procedure and diagnosis codes; the numerator is delivery admissions with any SMM diagnosis or procedure code. SMM-H rates use the same numerator as overall SMM, however the denominator only includes delivery admissions with a diagnosis of placenta previa, placental abruption, antepartum and/or postpartum haemorrhage and blood transfusion; the denominator excludes delivery admissions with sickle cell diagnosis codes.23 We met with our hospital Clinical Documentation Integrity team to inform them of this planned change and confirmed that we had a robust infrastructure for capturing accurate diagnosis and procedure codes for our patients.
Data disaggregation
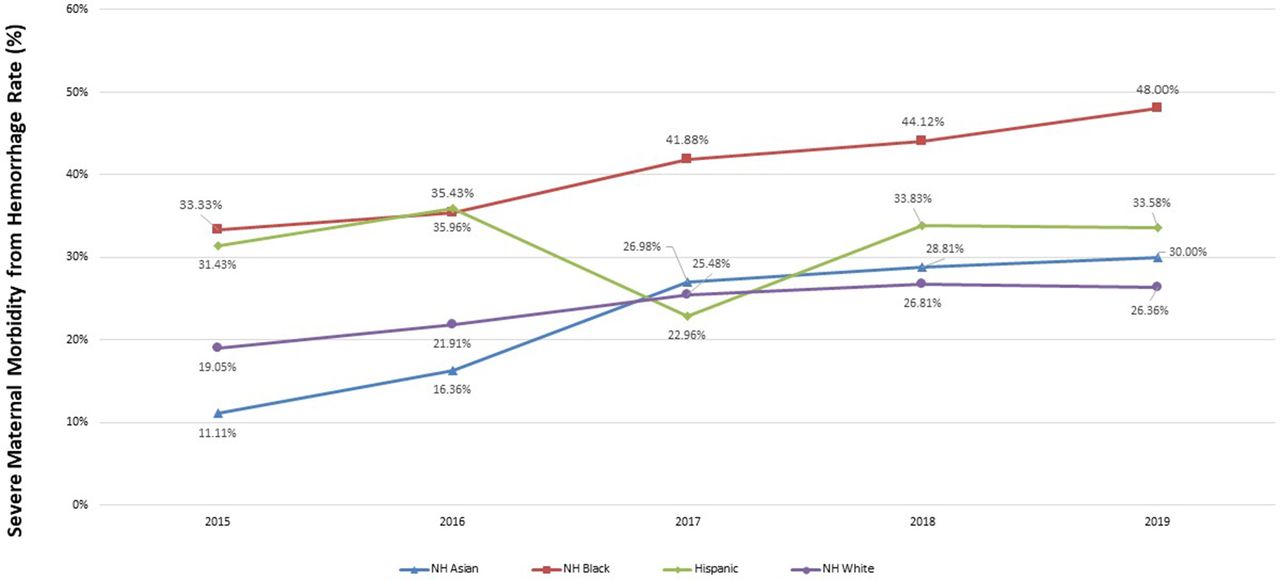
The hospital quality team started reporting on SMM and SMM-H data at monthly hospital department meetings beginning in January of 2019. Based on the national and state data regarding disparities in maternal morbidity and mortality for black women, we decided to overlay the AIM bundle on reduction of peripartum racial and ethnic disparities onto our haemorrhage efforts. We initially focused on the reporting and systems learning domain through disaggregation of data by monitoring outcome metrics stratified by race and ethnicity with regular dissemination to the department. For our March outcomes report, our quality team presented our SMM-H and SMM data since October 2015 in the form of run charts, stratified by race and ethnicity, to determine if we had disparities in outcomes (figure 1 and online supplemental appendix 2, respectively). For race and ethnicity classification, our hospital admissions team collects self-reported race and ethnicity data on all admitted patients and uses the Office of Management and Budget Standards,24 with ethnicity being either Hispanic/Latina or NH/Latina and race being categorised as American Indian or Alaska Native, Asian, black or African-American, white, Native Hawaiian or other Pacific Islander. For purposes of reporting our hospital outcomes, we adopted the following categories: NH-black, NH-white, Hispanic, NH-Asian and other. Based on this categorisation, we identified a disparity in our outcomes, with NH-black women having higher SMM and SMM-H rates compared with all other races and ethnicities delivering in our hospital. In fact, the rates in NH-black women were steadily increasing year over year with rates that were double those seen in our NH-white population.
Supplemental material

Rate of severe maternal morbidity from Haemorrhage by race and ethnicity: October 2015–February 2019 (created by the authors). NH, non-Hispanic.
Integration of bundle on reduction of peripartum racial and ethnic disparities
We continued to present stratified SMM and SMM-H data at monthly department meetings and incorporated discussions on national disparities in maternal morbidity and mortality and potential root causes, including implicit bias and lack of standardised clinical care. This education satisfied additional elements of the disparities bundle within the readiness and recognition domains. In an attempt to reduce the disparities in outcomes identified, bundle elements under development took health equity into consideration. This was primarily applied by the workgroups developing the postpartum haemorrhage (PPH) risk assessment and the multidisciplinary reviews of serious haemorrhages for systems issues. The PPH risk assessment workgroup decided to include black/African-American race as a medium risk factor for haemorrhage. Our rationale for doing this was based on the hypothesis that the increased morbidity in black women in our hospital was due to delayed recognition and response and that a systematic approach to creating a heightened awareness around their increased morbidity from haemorrhage may lead the healthcare team to intervene sooner (eg, earlier use of uterotonic agents). Additionally, the PPH risk assessment correlated with duration of postpartum oxytocin administration, and we developed an accompanying stratification for postdelivery management based on either the risk assessment performed on admission or the QBL at delivery (online supplemental appendix 3). We also restructured our quality and safety case reviews to include haemorrhage-specific questions and to consider the role of race, ethnicity, language and social determinants of health, using the framework set forth by the Council on Patient Safety’s SMM reporting forms.25 This approach to clinical case reviews satisfied one of the reporting and systems learning elements of the disparities bundle.
Supplemental material
Study design
In August 2019, our haemorrhage risk assessment, QBL and posthaemorrhage debriefs were implemented. In November 2019, the quality review committee held its first restructured meeting which included nurse reviewers and the fully expanded SMM case review format. Online supplemental appendix 4 illustrates the timeline of our interventions. We then conducted a retrospective cohort study around implementation of the obstetric haemorrhage bundle and data disaggregation to examine whether the interventions influenced reduction of morbidity from haemorrhage in our black population and the black-white disparity. We chose the date that SMM and SMM-H data were initially presented to our department stratified by race and ethnicity as the delineation between our baseline pre-intervention period and our post-intervention period because we noted a reduction in morbidity in black women with monthly discussion of the data even prior to full implementation of the bundle elements. We included all women with a delivery code in our hospital (excluding miscarriages and ectopic pregnancies) from June 2018 to June 2020. Our pre-intervention time period of June 2018 to February 2019 (before data disaggregation) was compared with our post-intervention time period of March 2019–June 2020 (after data disaggregation). The main outcome measure was the rate of SMM-H among black women. We also evaluated the overall SMM and the black-white disparity. P<0.05 was considered statistically significant. All descriptive and statistical analyses were performed using SAS, V.9.3 (SAS Institute, Cary, North Carolina, USA). The χ2 test was used for categorical outcomes and SMM data were displayed in run charts (Minitab V.17.3.1).
Supplemental material
Results
Table 1 summarises maternal demographic characteristics. During our study time period, there were 13 659 deliveries at our hospital: 4912 deliveries in the baseline group and 8747 deliveries in the intervention group. Of all deliveries, approximately 35% of women were NH-white, 20% NH-black, 37% Hispanic, 7% NH-Asian and 1% other. Compared with our baseline group, our intervention group had a slightly higher rate of NH-black and Hispanic women as well as a higher rate of women insured by Medicaid. Except for a slightly higher rate of multiple gestations in the baseline group, all other maternal demographic characteristics were similar.
Maternal characteristics
Table 2 shows the SMM and SMM-H rates as well as the associated increase or decrease in rates in the post-intervention group as compared with the pre-intervention group. The rate of SMM-H decreased significantly from 34.10% in the pre-intervention group to 26.67% in the post-intervention group, corresponding to an almost 22% reduction in rate (p<0.01). In the haemorrhage subgroup, there was an associated 26% reduction in transfusion codes (p<0.01), however there was no difference in transfusions of four or more units of packed red blood cells (PRBCs) between baseline and post-intervention groups (p=0.99).
Rates of SMM overall and from haemorrhage
When examining by race and ethnicity, the rate of SMM-H did not change significantly in NH-white women from pre-intervention to post-intervention phase (28.1% pre-intervention vs 25.7% post-intervention, p=0.55) or in NH-Asian women (31.8% pre-intervention vs 24.5% post-intervention, p=0.41). The rate of SMM-H in NH-black women, however, decreased significantly from 45.5% in the pre-intervention group to 31.6% in the post-intervention group (p=0.011) (figure 2). There was also a significant reduction in the rate of SMM-H in Hispanic women (33.2% pre-intervention vs 25.3% post-intervention, p=0.028).

Rate of severe maternal morbidity from haemorrhage (SMM-H) in non-Hispanic black mothers (created by the authors).
The overall rate of SMM in NH-black women decreased from 7.1% in the pre-intervention group to 5.1% in the post-intervention group (p=0.038) (online supplemental appendix 5). No other race or ethnicity experienced a significant change in the overall SMM rates. We saw a reduction in SMM-H (figure 2) and SMM (online supplemental appendix 5) among NH-black women immediately after presenting stratified data to the department and before completing implementation of the remaining bundle elements (haemorrhage risk assessment, debriefs and QBL measurement), which were fully implemented in August 2019.
Supplemental material
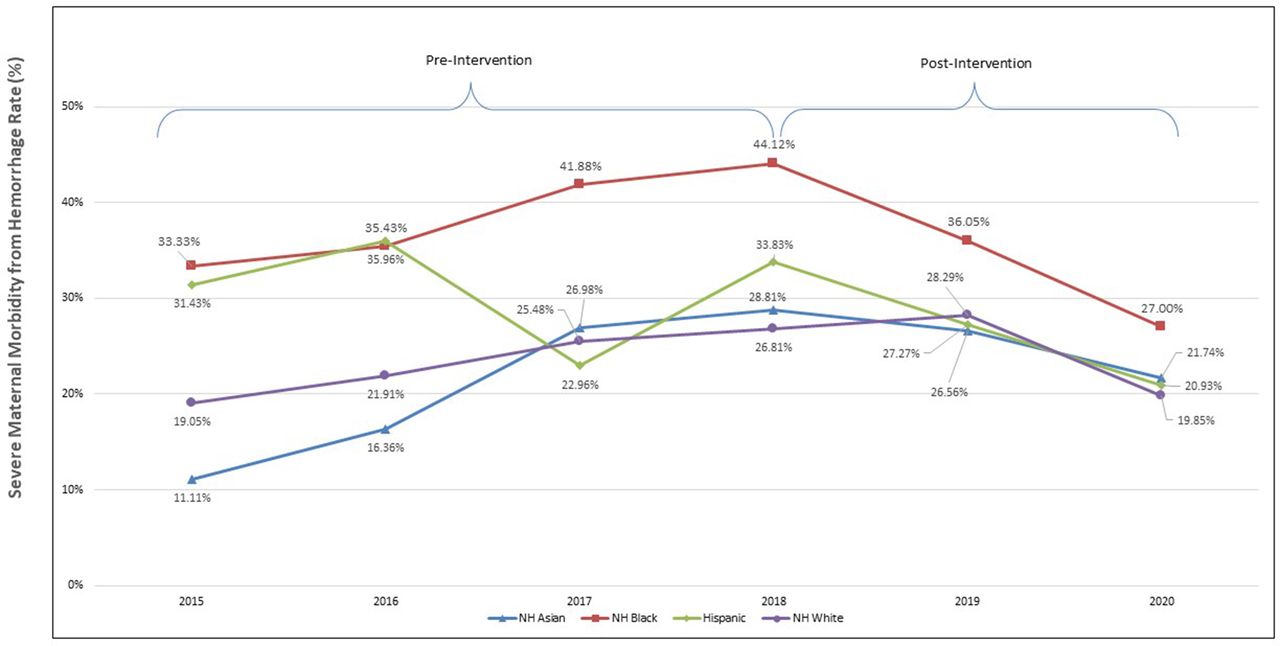
In the pre-intervention group, there was a statistically significant difference in the NH-black versus NH-white rate of both SMM and SMM-H (p<0.001 for both). This disparity remained significant post-intervention for overall SMM (p=0.008), however the NH-black versus NH-white difference in the haemorrhage subgroup was no longer statistically significant (p=0.138). Figure 3 shows the run chart of SMM-H among all races and ethnicities from October 2015 to the end of the post-intervention period.

{kind=link}
{kind=link}
{kind=link}
Rate of severe maternal morbidity from haemorrhage by race and ethnicity, October 2015–June 2020 (created by authors). NH, non-Hispanic.
Process measures were submitted to TexasAIM quarterly and included the compliance rate with measurement of QBL at delivery and performance of PPH risk assessment on admission. By quarter four of 2019, we maintained at least an 80% compliance rate with both interventions.
Discussion
Principal findings
In this retrospective cohort analysis of deliveries in our hospital, we showed that overall SMM and SMM-H decreased significantly in NH-black women and the NH-black versus NH-white disparity in morbidity from haemorrhage was eliminated following the implementation of QI and patient safety interventions that focused on standardising care around haemorrhage with a health equity framework. Our interventions were informed by results of data disaggregation at the outset of our project. This allowed us to consider root causes of the disparities, such as implicit bias and lack of standardised care, and factor them into our interventions that were under development. Of particular interest, we noted a reduction in SMM and SMM-H rates in black women delivering in our hospital immediately following data disaggregation and monthly departmental presentation, even before all haemorrhage bundle elements had been implemented. Additionally, we achieved a 22% reduction in SMM-H in the entire delivery population in the post-intervention phase as compared with baseline, which approaches the state goal of reducing morbidity from haemorrhage by 25% and was a statistically significant reduction in our population. This reduction was primarily attributed to a significant reduction in blood product transfusion of amounts <4 units of PRBCs since there was no change in the rate of massive transfusion in the post-intervention phase compared with baseline. We presume this is a direct consequence of earlier interventions to prevent and treat haemorrhage as a result of full implementation of the haemorrhage bundle elements.
Clinical implications
Our findings add to the body of work that highlights the impact of QI initiatives aimed at standardising delivery care as well as data disaggregation to allow hospitals and healthcare systems to become aware of disparities within their hospitals.26–28 When our haemorrhage risk assessment workgroup was developing our hospital-specific plan, they took the known disparities under consideration and decided to add black/African-American race as a medium risk factor. The risk factors in each category were selected based on either being known risk factors for haemorrhage or risk factors for complications from haemorrhage. For example, a woman with anaemia and/or thrombocytopenia on admission for delivery is not necessarily at increased risk for haemorrhage, however she is more likely to require a blood transfusion if she does experience a haemorrhage. That was the rationale in including black race as a medium risk factor: the recognition that black women who delivered in our hospital were experiencing more complications from haemorrhage, not that they were necessarily at increased risk for haemorrhage. Prior studies evaluating the association of maternal race and ethnicity and the risk of PPH have demonstrated that Hispanic ethnicity and Asian/Pacific Islander race are significant risk factors for atonic haemorrhage, independent of measured potential mediators.29 Interestingly, the study also demonstrated that black/African-American race was associated with slightly lower odds of atonic PPH in comparison with white race, but an increased odds of atonic PPH resulting in transfusion and hysterectomy.29 This suggests that African-American women haemorrhage from atony less often than do white women, but when they do, the haemorrhage tends to be more severe. Therefore, we anticipated that our inclusion of black race as a medium risk factor would lead to a heightened response when presented with heavier than expected bleeding, such as early use of uterotonic agents and longer duration of postpartum oxytocin.
Research implications
Our project design is unique in that we disaggregated our data at the outset of the QI initiative, thereby allowing us to prospectively work to identify strategies to provide equitable care and target interventions that could reduce or eliminate the specific disparity identified. Once identified, we presented the data to organisation leaders, and presented it to bedside clinicians who were actively engaged in direct patient care. This follows the IHI model that recommends using REaL data to stratify one strategic measure to build will and interest among leaders and clinicians. Organisations can gain experience in improving equity by first applying an ‘equity lens’ to existing improvement projects aligned with strategic priorities rather than chartering new projects with the specific focus to improve equity.18 This may also lend to a positive Hawthorne effect (behavioural change influenced by the knowledge that one is being observed) even before interventions are implemented since it would be expected that the recognition of disparities in one’s hospital would lead medical providers to have a more thoughtful approach when interacting with the patient population that is being negatively impacted by the disparity. In our study, there is evidence that simply sharing the data with the providers and staff of the disparity led to an initial reduction in SMM and SMM-H among black women.
Strengths and limitations
Our study is limited by the use of administrative data for outcomes, which carries the risk of both overcoding and undercoding. We felt confident, however, converting to this data metric after meeting with our Clinical Data Integrity team as they have well-defined criteria for assigning each SMM diagnosis and there was no variation in their methods over the study time period. We are also limited in our ability to determine the unique contribution of the bundle elements versus presenting disaggregated data to our observed reductions in morbidity and disparity. We feel that the two are essential to all QI efforts to eliminate disparities. Our study has several strengths. Our hospital admissions team collects self-reported race and ethnicity on all deliveries, which are generally regarded as the gold standard. The prospective monitoring of disparities throughout bundle implementation informed our efforts and would have allowed for different approaches through multiple plan-do-study-act cycles if we were not seeing a reduction in disparities from our initial efforts. Additionally, we feel that our results are generalisable in that our hospital has a very diverse population that is reflective of the demographic make-up of the city of Houston, Texas30 and the USA overall. Our targeted approach to outcome disparity recognition and reduction is also generalisable in that it can be applied to any health outcome disparity and QI initiative.
Conclusions
Overlaying the AIM disparities bundle onto all QI and patient safety initiatives and evaluating disaggregated baseline data to inform efforts is a QI approach that can be useful for reducing health disparities.
Data availability statement
No data are available. not applicable.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Institutional Review Board for Human Subject Research.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CD
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.