Article Text

Abstract
Background and objective Handoff communication errors are a leading source of sentinel events. We sought to determine the impact of a handoff improvement programme for nurses.
Methods We conducted a prospective pre-post intervention study on a paediatric intensive care unit in 2011–2012. The I-PASS Nursing Handoff Bundle intervention consisted of educational training, verbal handoff I-PASS mnemonic implementation, and visual materials to provide reinforcement and sustainability. We developed handoff direct observation and time motion workflow assessment tools to measure: (1) quality of the verbal handoff, including interruption frequency and presence of key handoff data elements; and (2) duration of handoff and other workflow activities.
Results I-PASS implementation was associated with improvements in verbal handoff communications, including inclusion of illness severity assessment (37% preintervention vs 67% postintervention, p=0.001), patient summary (81% vs 95%, p=0.05), to do list (35% vs 100%, p<0.001) and an opportunity for the receiving nurse to ask questions (34% vs 73%, p<0.001). Overall, 13/21 (62%) of verbal handoff data elements were more likely to be present following implementation whereas no data elements were less likely present. Implementation was associated with a decrease in interruption frequency pre versus post intervention (67% vs 40% of handoffs with interruptions, p=0.005) without a change in the median handoff duration (18.8 min vs 19.9 min, p=0.48) or changes in time spent in direct or indirect patient care activities.
Conclusions Implementation of the I-PASS Nursing Handoff Bundle was associated with widespread improvements in the verbal handoff process without a negative impact on nursing workflow. Implementation of I-PASS for nurses may therefore have the potential to significantly reduce medical errors and improve patient safety.
- Hand-off
- Communication
- Nurses
- Patient safety
Statistics from Altmetric.com
Introduction
Up to 70% of serious errors and sentinel events in hospitals are caused by miscommunications,1 of which handoff errors are a leading source.2 Handoffs of care between clinical providers have consequently emerged as a major focus in the patient safety movement. The current crisis regarding handoffs is due in part to the changing work schedules of physicians-in-training (residents) and nurses. In an effort to recruit new nurses and retain existing staff as well as to avoid the potential for fatigue-related error, many hospitals are now offering flexible work hours that include shifts of variable length with many nurses choosing to work a combination of these shifts. Many nurses elect to work less than 40 hours per week leading to high rates of handoffs for each individual patient. Additionally, to support the need for staffing, nurses often are requested to assume patient care duties across several units, often without prior knowledge of patients or typical care practices on that unit.3–5
While some literature supports the value of resident handoff tools both in improving patient safety and efficiency of care,6–11 rigorous studies of nursing handoffs have been more limited.12–15 Studies that have been conducted have identified problems in the data transmission process due to lack of standardisation13 16–19 as well as deficiencies in infrastructure to support handoffs, technology limitations, and a high rate of interruptions and miscommunications.17 19–21 While numerous problems have been identified, however, there is a lack of robustly designed studies examining the impact of nursing handoff interventions.12 13 15 Researchers have therefore called for additional research to provide empirical evidence on the nursing handoff process, and for more rigorous studies of nursing handoff interventions.14 15 22
To address this gap, our pilot study sought to gather further information regarding barriers and facilitators of nursing handoffs, as well as to outline potential strategies for improving the handoff process. In prior work, we found that implementation of a bundle of interventions built around the mnemonic I-PASS (I: Illness Severity, P: Patient Summary, A: Action List, S: Situation Awareness and Contingency Plans, S: Synthesis by Receiver) was associated with a reduction in medical error rates and improvements in communications for resident physicians at change of shift.10 However, the I-PASS framework has not previously been studied in an intensive care unit (ICU) setting and studies examining its use for other specialties and provider types such as nurses remain limited.23 We hypothesised that implementation of a modified I-PASS Handoff Bundle for nurses working in an ICU would lead to improvements in verbal communication and a reduction in handoff interruptions, without a negative impact on nursing workflow.
Materials and methods
Study design
After approval by the institutional review board, we conducted a prospective intervention study to evaluate the effects of the I-PASS Nursing Handoff Bundle. Preintervention data were collected from June 2011 through March 2012, followed by a 6-month wash-in period during which the intervention was introduced, with postintervention data collected from October through November 2012. During the intervention, all nurses received I-PASS handoff training (as described below) and were asked to use I-PASS handoff processes while working on the study units. However, only nurses who provided written informed consent contributed time-motion workflow data or had their verbal handoffs observed. All nurses working on the study unit were asked to complete a survey regarding their perceptions of the handoff process and perceived barriers to improvements in the handoff process; completion of this survey implied consent to participate in this aspect of the study.
Setting
The setting for the study was a 29-bed medical and surgical ICU with an average nursing ratio of 1 nurse to 2 patients. All nurses working on the study unit worked 12-hour shifts starting and/or ending at 07:00/19:00. At baseline, there was no standardised nursing handoff programme in place for verbal handoffs. The typical format for verbal handoffs was in person and typically took place outside the patient’s room. No handoffs occurred over the phone or via tape recording. Typically, nurses completed an unstructured verbal exchange at the end of shift without any transmission of written information. Informal handoffs also occurred during times of coverage for brief breaks or lunch or dinner breaks.
Intervention
The I-PASS Nursing Handoff Bundle included educational training on best practices for verbal communication, verbal handoff I-PASS mnemonic implementation, and visual materials to provide reinforcement and sustainability. To adapt the bundle components from the materials previously developed for the resident physician I-PASS Handoff Bundle,24 25 we applied Kern’s six-step approach to curriculum development26 including conducting a needs assessment, writing goals and objectives, designing educational activities, implementing and evaluating the curriculum, and revising and refining the curriculum as needed. The curriculum was developed based on several educational theories including social cognitive learning theory (suggesting that individuals learn by observing others and reacting to environmental cues) and experiential learning theory (suggesting that individuals learn through active experience, reflection and adaptation of future behaviours).
In-person training was performed in collaboration with designated unit educators on the study unit. This training instructed nurses on the important elements of handoffs including: unambiguous transfer of responsibility, the importance of protected time and space when conducting handoffs, how to minimise interruptions except in emergent situations, and how to use a standardised, structured format which begins with a high-level overview or patient summary and then proceeds with an agreed-upon specific order in which patient information would be relayed. Nurses were also educated on the importance of having and providing up-to-date, accurate and relevant information, as well as the need to conduct handoffs at an appropriate pace. The importance of closed loop communication was also stressed to help nurses achieve a shared mental model. This included encouraging nurses to solicit read-back of salient points and to prompt the receiver to ask clarifying questions.
A key component of the bundle and training included standardisation of the verbal handoff process using the I-PASS format that served as a standardised framework for verbal handoffs and has previously been described for use in resident physician change of shift handoffs.10 24 27 We conducted several focus groups with front line nurses working on the study unit, charge nurses, nurse educators and nurse managers in order to tailor the resident I-PASS handoff mnemonic for use by nurses in the ICU setting. Primary adaptations included standardisation of the Patient Summary field to provide suggested structure and content relevant for nurses (table 1).
A sample verbal nursing handoff using the I-PASS handoff mnemonic
We recognised that successful implementation of the I-PASS Nursing Handoff Bundle would require fundamental changes to the ways in which providers communicate about patients and would benefit from institutionalising the intervention as a key component in the transformation. In order to advertise and brand the implementation efforts, we adapted the elements of the I-PASS Resident Handoff Bundle campaign toolkit for use in a nursing context. Visual reinforcement materials with the aim of further reinforcing key I-PASS concepts were implemented on the study unit such as posters and computer monitor frames reminding staff of the mnemonic elements.
Main outcome measures
Assessment of verbal handoffs
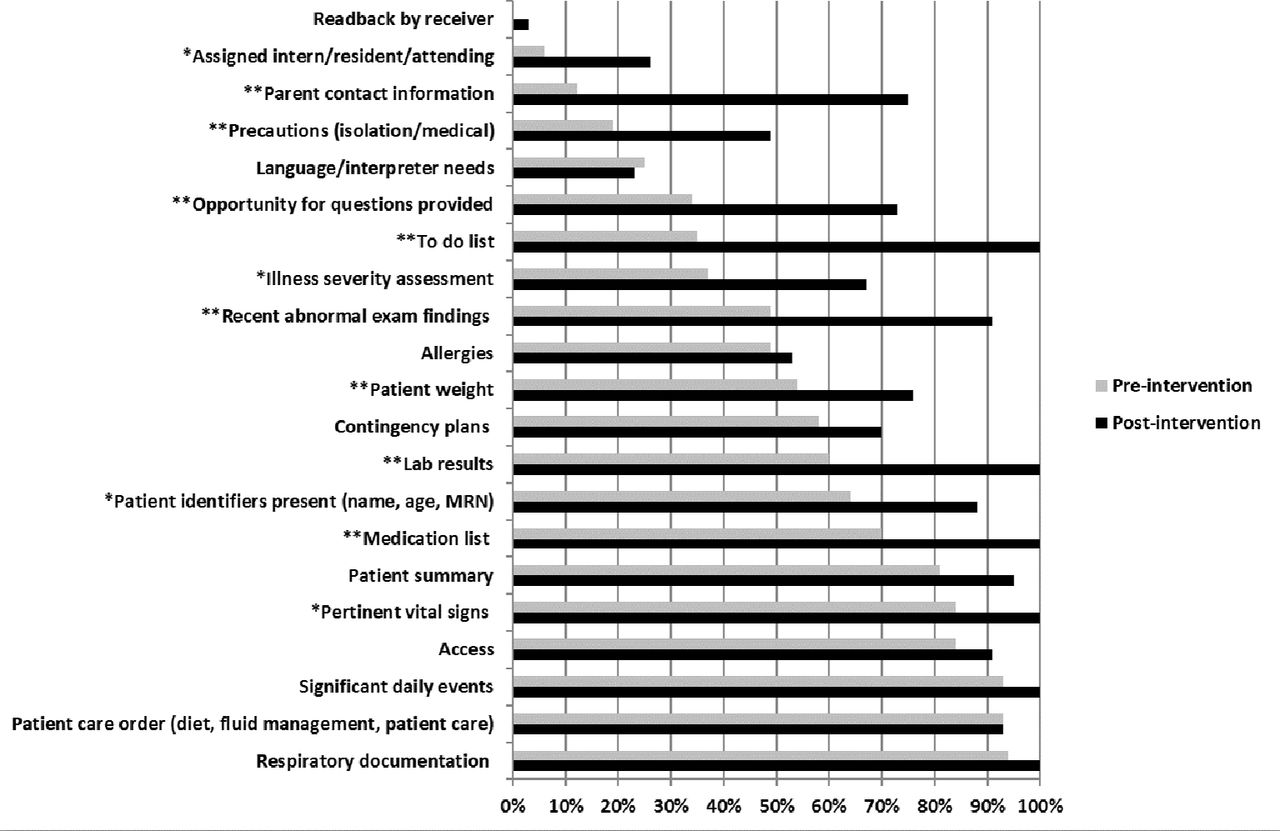
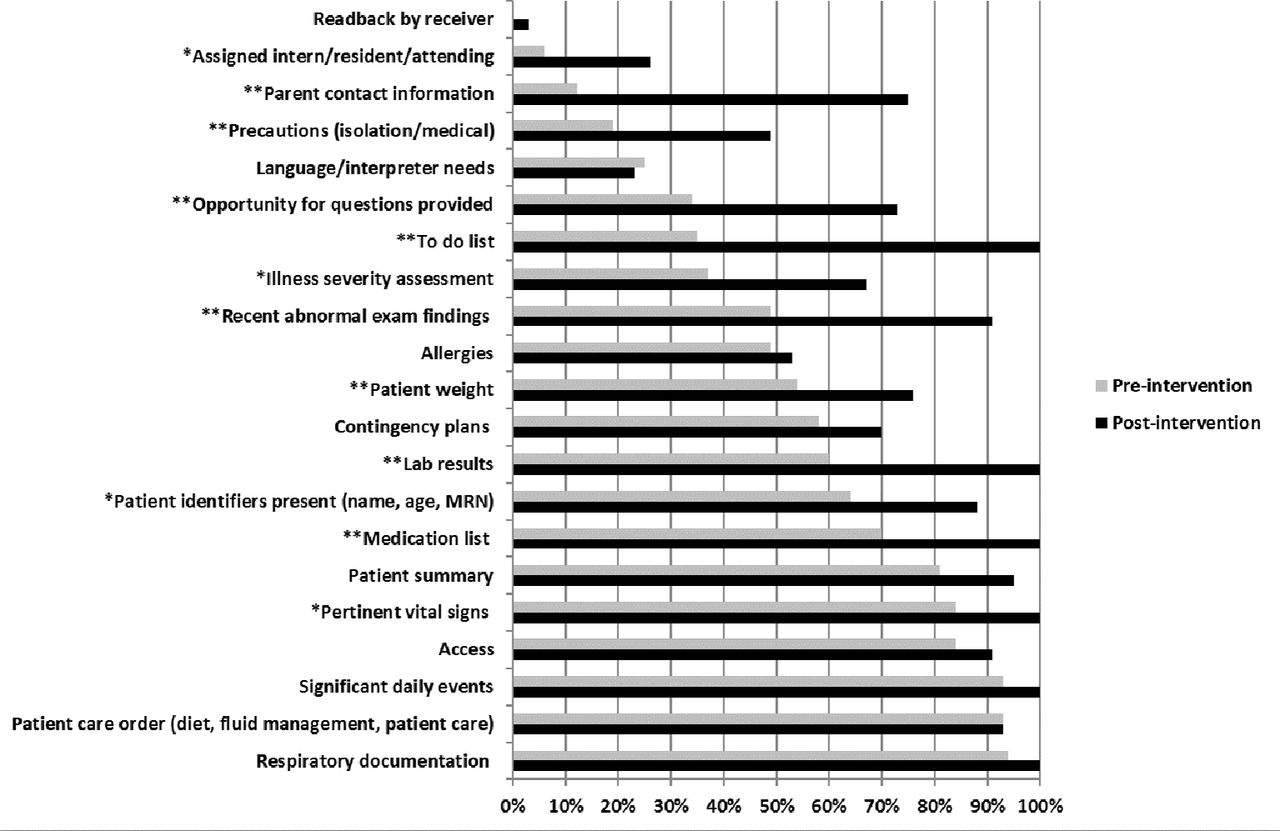
Research assistants and research nurses conducted direct observations of the nursing handoff process during both the preintervention and postintervention periods. We created a nursing handoff assessment tool to capture critical data elements of the end of shift handoff common to the ICU setting known to be related to rates of medical errors and miscommunication.10 These data elements were selected based on review of the literature and existing handoff assessment tools,10 28 29 input from nurse educators, nurse managers, nurse infomaticians and front line staff. Research assistants recorded the presence or absence of 21 key elements (figure 1) during end of shift handoffs. Additionally, the research team rated the quality of five key data elements on a 5-point Likert scale adapted from a prior study evaluating verbal handoffs for resident physicians.30 Research assistants also catalogued the frequency, duration, type and source of interruptions during the period of verbal handoff.
{kind=link}
Frequency of inclusion of verbal handoff data elements pre implementation versus post implementation. *=p<0.05, **=p<0.01.
Assessment of nursing workflow patterns
Leveraging prior work performed in evaluating the impact of bar code/ electronic medication administration records for nurses and handoffs among residents,31–33 we sought to develop a time motion and handoff observation tool to study the end of shift nursing handoff process, and the impact this process had on nursing workflow. We categorised nurse activities by adapting a previously published activity list for nurses, deleting elements that were not relevant for paediatric inpatient use.31 These categorisations of the nurse activities and handoff elements were further refined following meetings with key nursing staff members (including nurse managers, educators and front line staff) to better identify nurse’s daily tasks. We then performed a 2-week pilot in the study units and made necessary iterations to the tool based on the results of this pilot. The nursing activities were classified into categories that corresponded to visible activities such as using the computer, communicating with patients and providers, physically caring for patients and medication administration. Subcategories were developed to capture the specifics of a particular activity. Nursing activity was divided into two main categories for analysis including direct patient care and indirect patient care. Direct patient care activities included 39 subcategories related to 19 major categories of nursing activities (patient activity, bowel, coping, fluid volume, behavioural health, infection control, infusion care, medication care, nutrition, physical regulation, radiology, respiratory, role/relationship, safety, self-care, sensory, skin integrity, transfusion care and urinary) taking place in the presence of the patient such as talking with patients or administering medications or therapies. Indirect patient care activities that did not take place in the presence of the patient included 78 subcategories of nine major categories (communication, computer, documentation, education, looking for, medication care, miscellaneous, personal time and unit-related) activities that do not occur in the presence of the patient including reviewing and recording data or communicating with members of the medical team. Once the categorisation was finalised, we programmed the tool into a time-motion study application within an MS Access database. This application was loaded onto a laptop computer to enable research assistants to log nursing activities in real time. The application included built-in time stamps, allowing the observers to press a touch screen when the nurse starts, completes or suspends an activity. Tasks/activities observed and the time spent on activities were recorded by the application for later analysis.
The study also specifically focused on the handoff process as it related to overall nursing workflow. Additional outcomes of interest included the percentage of time spent engaged in the patient handoff process. Once identified, the specific variables were added to the time-motion study instrument for data collection purposes. Research assistants were trained by study investigators to conduct 8–12 hours of observation sessions with a single nurse and record his/her activities using a tablet computer. Each observation session was completed by a single research assistant. Research assistant training was performed by clinical research specialists, to help ensure accuracy in data collection and maintenance of proper patient and nursing confidentiality.
Nursing experience with the handoff process
During the baseline period, as part of a needs assessment exercise prior to the launch and design of the nursing handoff bundle, a survey was distributed to all nurses working on the study unit to assess overall experience and satisfaction with the current handoff process as well as perceived barriers and facilitators of handoff improvement efforts.
Analysis
We used χ2 tests to compare the percentage of verbal handoffs with any interruptions in the preintervention versus postintervention periods and Poisson tests to compare the number of interruptions per 100 handoffs. The number of interruptions by type and source was also compared with Poisson tests. We compared the rates of inclusion of key data elements as well as the quality of the handoffs in the preintervention versus postintervention periods using χ2 tests. To compare distributions of time-motion data pre intervention versus post intervention, we used bootstrapping to estimate the change in the percentage of time devoted to direct and indirect patient care activities, overall and by shift. Day shifts were defined as time from 06:30 to 18:30, and night shifts were defined as 18:30 to 06:30, in conjunction with the defined nursing hours of the study unit.
We powered the study to address the primary outcome of interest, the percentage of nursing time spent in direct patient care activities in a 24-hour period. Prior data from nursing time-motion studies suggest that nurses spend 26.1% of their time performing direct patient care activities. For the purposes of our analysis, a 25% change in time spent performing direct patient care was considered clinically significant. Therefore, it was determined that a sample size of 750 hours would allow for 80% power to detect a 25% reduction in nursing work hours spent in direct patient care, assuming a two-sided alpha error of 0.05%.
Results
Fifty-nine per cent of nurses completed a handoff experience survey (n=90) during the preintervention period that served as a needs assessment. Participating nurses were primarily female (95.3%) and of Caucasian race (94.9%) but represented a range of levels of training, academic achievement and work schedules (table 2). At baseline, 65.3% of nurse subjects perceived that inadequate training on how to hand off patient information was an important barrier to successful nursing handoffs. Use of a standardised verbal mnemonic and protected time to conduct handoffs free of interruptions and distractions was cited as key a solution to improve nursing handoffs.
Characteristics of nursing subjects
A total of 126 handoffs were observed (n=81 preintervention, n=45 postintervention). Implementation of Nursing I-PASS was associated with significant increases in the inclusion of key handoff data, including: the identification of the primary physician (6% vs 26%, p=0.004), parent contact information (12% vs 75%, p<0.001), whether the patient was on isolation or medical precautions (19% vs 49%, p<0.001), opportunity to ask questions (34% vs 73%, p=0.001), to do list (35% vs. 100%, p<0.001), illness severity assessment (37% vs 67%, p=0.001), recent abnormal exam findings (49% vs 91%, p<0.001), patient weight (54% vs 76%, p<0.001), laboratory results (60% vs 100%, p<0.001), patient identifiers such as name/age, and medical record number (64% vs 88%, p=0.005), a medication list (70% vs 100%, p<0.001) and pertinent vital signs (84% vs 100%, p=0.004) (figure 1).
Rating of the quality of five verbal handoff elements on a 5-point Likert scale demonstrated significant improvement in the frequency of handoff observations rated as a 4 or 5 during the postintervention period for the following handoff elements: overall health status (68% vs 96%, p<0.001), general hospital course (43% vs 78%, p<0.001), upcoming possibilities (55% vs 82%, p=0.003) and tasks to complete on the next shift (44% vs 84%, p<0.001) (table 3).
Quality of communication of key handoff data elements
Following implementation of Nursing I-PASS, there was a significant reduction in the percentage of handoffs that had interruptions present (67% vs 40%, p=0.005, table 4).
Frequency and characteristics of handoff interruptions pre intervention versus post intervention
The most frequent type of interruption that occurred was medically related to the patient being discussed, which declined significantly during the postintervention period (102 vs 60 per 100 handoffs, p=0.02).However, even larger reductions were observed in medical interruptions unrelated to the patient being discussed (36 vs 4 per 100 handoffs, p=0.004). Those interruptions that were initiated by a nurse were significantly likely to decrease following the intervention (63 vs 24 per 100 handoffs, p=0.004) whereas those interruptions that were initiated by other individuals including physicians, other staff, the patient or family, or other sources of interruptions did not decrease significantly following the intervention.
A total of 765 hours of time-motion data were collected (n=351 preintervention, n=414 postintervention). There was not a significant difference in the median duration of each patient handoff (18.8 min vs 19.9 min, p=0.48) following implementation of the I-PASS Nursing Handoff Bundle. Additionally, implementation was not found to be associated with any significant changes in the amount of time spent in direct (39.6% vs 40.8%, 95% CI −2.7%, 5.0%) or indirect (60.4% vs 59.2%, 95% CI −5.0%, 2.7%) patient care activities (table 5). Similarly, key major categories of indirect care activity that potentially might have been impacted by the intervention did not change significantly pre intervention vs post intervention including communication with staff and colleagues (19.0% vs 21.1%, 95% CI −0.6%, 4.7%), time at the computer (10.6% vs 8.6%, 95% CI −4.5%, 0.5%) or documentation (6.5% vs 8.7%, 95% CI 0.0%, 4.7%).
Percentage of time spent by nurses working on study unit on direct and indirect patient care activities*, assessed through time-motion study
Discussion
We found that implementation of the I-PASS Nursing Handoff Bundle was associated with significantly increased inclusion of key data elements during verbal handoff sessions, and a 40% reduction in rates of interruptions. In addition, verbal handoffs included higher quality data elements without a significant change in the median duration of each patient handoff or change in nursing workflow patterns. These findings support the hypothesis that the I-PASS Handoff Programme is applicable and effective for nursing handoffs of care within a paediatric ICU setting.
Prior investigations have found that nursing handoffs lack standardisation, and that lacking this standardisation, nursing handoffs are frequently ‘partial’ and ‘cryptic.’18 19 34 Yet, despite calls from the Joint Commission and others for structured handoffs,17 very little evidence has been generated to support the use of any specific structure, protocol or method.12 13 15 35 Furthermore, although a handful of prior studies have described the use of the situation, background, assessment and recommendation as an organising framework to standardise nursing handoffs of care,36–38 this particular mnemonic was not designed for purposes of handoff communication and lacks key data elements felt to be important for optimisation of patient safety during transitions of care.27 Here we provide evidence demonstrating the applicability of the I-PASS mnemonic for nursing handoffs, which has previously proven successful as a framework for organising physician handoffs as well.10
Interruptions during nursing handoffs are known to be frequent and contribute significantly to miscommunications.39 The measurement and categorisation of interruptions and their impact on patient safety is complex.40 Our study found a significant decrease in overall rates of interruptions during periods of verbal handoffs following implementation of I-PASS for nurses, with the most significant reductions occurring among interruptions initiated by nurses, and involving issues unrelated to the patient being handed off. The reduction in nursing-initiated interruptions in particular suggests that nurses who were trained in I-PASS came to view the handoffs of their peers as safety critical events that should not be unnecessarily interrupted, but this learning did not extend to other staff in this unit (eg, physicians) who had not been trained in I-PASS. Further investigation is needed to learn whether implementation of I-PASS in other disciplines might lead to further reductions in handoff interruptions initiated by those disciplines.
The results of the current study are consistent with two prior studies we have conducted of the effectiveness of a resident-physician handoff bundle on handoff communications, resident workflow and patient safety.9 10 The current study adds significantly to these demonstrating that implementation of I-PASS resulted in similar communication improvements when used by nurses in a paediatric ICU setting.
An important limitation of our study is that we did not have the resources in this project to measure whether implementing I-PASS was associated with a reduction in medical errors or preventable adverse events, as well as a reduction in miscommunications. In our studies of resident physicians, however, communication improvements quite similar to those seen here were accompanied by substantial improvements in patient safety,9 10 suggesting that safety improvements may have accompanied the implementation of the I-PASS Nursing bundle as well. Moreover, a multicentre collaborative handoff study in which we participated, and in which I-PASS was used at our institution (but not other institutions) demonstrated improvements in nurse-reported clinical handoff failures following implementation of handoff bundles across sites.41 Further studies investigating this possibility in greater depth should be conducted.
Our study has a number of additional limitations. First, we studied one ICU in a single paediatric hospital. Although the nursing schedules and baseline handoff practices we evaluated are common, it is unclear how generalisable our findings may be to other settings, other provider types or other types of handoff communication such as interunit transfers. Second, because of the observational design, causality cannot be established. Third, our study design precluded the ability to blind nurses and research assistants to the intervention period, a common limitation of systems-based patient safety interventions. We addressed this by training all data collectors, none of whom were study investigators, to collect data on handoff observations and workflow in a standardised manner, emphasising the importance of consistent, objective data collection. However, the possibility of a Hawthorne effect secondary to the presence of the observers cannot be ruled out entirely, though any Hawthorne effect should have been present both pre intervention and post intervention. Finally, our pre-post study design did not account for ongoing secular trends as would an alternate approach such as an interrupted time series design42–44; nor did it afford the opportunity to continue to longitudinally study the sustainability of the intervention over time, which would be an important area of focus for future research and/or quality improvement efforts.
In conclusion, we found that implementation of the I-PASS Nursing Handoff Bundle was associated with improvements in the completeness and quality of handoff communications and reductions in rates of interruptions, without a significant impact on handoff duration or nursing workflow. Future investigations should investigate the reproducibility of these findings in additional settings and for multiprofessional handoffs, as well as factors associated with successful adaptation and implementation in additional environments.
References
Footnotes
Contributors AJS and CL designed the study. KOS collected the data. RH and DAG performed the statistical analyses. AJS wrote the original draft of the manuscript. AJS, KOS, AL, RH, DAG, CK and CL were involved in interpreting the findings and editing the manuscript. AJS is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests AJS reported receiving honoraria and travel reimbursement from multiple academic and professional organisations for delivering lectures on handoffs and patient safety. She has consulted with and holds equity in the I-PASS Institute, which seeks to train institutions in best handoff practices and aid in their implementation. CL likewise has consulted with and holds equity in the I-PASS Institute. In addition, he has served as a paid consultant to Virgin Pulse to help develop a Sleep and Health Program. He is supported in part by the Children’s Hospital Association for his work as an Executive Council member of the Pediatric Research in Inpatient Settings (PRIS) network. He has received monetary awards, honoraria and travel reimbursement from multiple academic and professional organisations for teaching and consulting on sleep deprivation, physician performance, handoffs, and safety, and has served as an expert witness in cases regarding patient safety and sleep deprivation. No other authors reported disclosures.
Provenance and peer review Not commissioned; externally peer reviewed.