Article Text

Abstract
Objective To assess the efficacy of an electronic discharge communication tool (e-DCT) for preventing death or hospital readmission, as well as reducing patient-reported adverse events after hospital discharge. The e-DCT assessed has already been shown to yield high-quality discharge summaries with high levels of patient and physician satisfaction.
Methods This two-arm randomised controlled trial was conducted in a Canadian tertiary care centre’s internal medicine medical teaching units. Out of the 1953 patients approached and screened for inclusion, 1399 were randomised and available for data linkage for determination of the primary outcome. Participants were randomly assigned to e-DCT versus usual care (traditional discharge communication generated by dictation). The primary outcome was a composite of death or readmission within 90 days. The secondary outcome included any patient-reported adverse events within 30 days of discharge.
Results Among 1399 randomised participants, 230 of 701 participants (32.8%) in the e-DCT group experienced the primary composite outcome of death or readmission within 90 days vs 205 of 698 participants (29.4%) in the usual care group (p=0.166). The incidence at 30 days of patient-reported adverse outcomes (35% for e-DCT vs 34% for usual care) and adverse events (2.1% for e-DCT vs 1.8% for usual care) also did not differ significantly between groups.
Conclusions The e-DCT tested did not reduce the composite endpoint of death or readmission at 90 days, nor the incidence of patient-reported adverse events at 30 days. This neutral finding for hard clinical endpoints needs to be considered in the context of high patient and physician satisfaction, and high quality of discharge summaries.
Statistics from Altmetric.com
Introduction
The transition between acute care and community-based care represents one of the most vulnerable periods in medical care, particularly as the complexity of the inpatient population increases.1–3 In most health systems, discharge communication still relies heavily on the use of handwritten or dictated discharge summaries, despite documented shortcomings.1–9 At the first visit after hospitalisation, this summary is unavailable to the community care physicians up to 75% of the time.4 8–10 When summaries are received, inconsistent content and inaccuracies are common.6 9 11 Acute care physicians often neglect to include diagnostic findings, hospital course, medication changes and follow-up plans.12
Electronic communications with structured discharge summaries developed on a communications platform bridging acute-care and community-care sectors provide a potential approach to improving the timely delivery of information. Such tools can standardise information content and how information is conveyed to community providers.13–19
The purpose of this study was to assess the efficacy of an electronic discharge communication tool (e-DCT) that our team developed in partnership with the provincial health authority for acute care discharges from several acute care hospital sites. Our specific objective was primarily to assess the efficacy of the e-DCT for reducing death or hospital readmission within 90 days from hospital discharge, and second to assess patient-reported adverse events occurring within 30 days. This clinical trial assessing hard clinical endpoints was preceded by a pilot evaluation of the deployed e-DCT tool showing high-quality discharge summaries and high levels of patient and physician satisfaction.20–23 Our clinical trial was also preceded by our completion of a systematic review of the literature19 showing benefits of e-DCT interventions on timeliness and quality of discharge summaries, and also provider and patient satisfaction. Effects of e-DCT interventions on hard clinical endpoints such as readmission, death and adverse events are, on the other hand, much less clear because of insufficient power.19 This large clinical trial is one of the first to have sufficient statistical power to examine the impact of an e-DCT on these important clinical outcomes.
Methods
The study was approved by the Conjoint Health Research Ethics Board at the University of Calgary, and it is registered at ClinicalTrials.gov (NCT01402609).
The e-DCT intervention
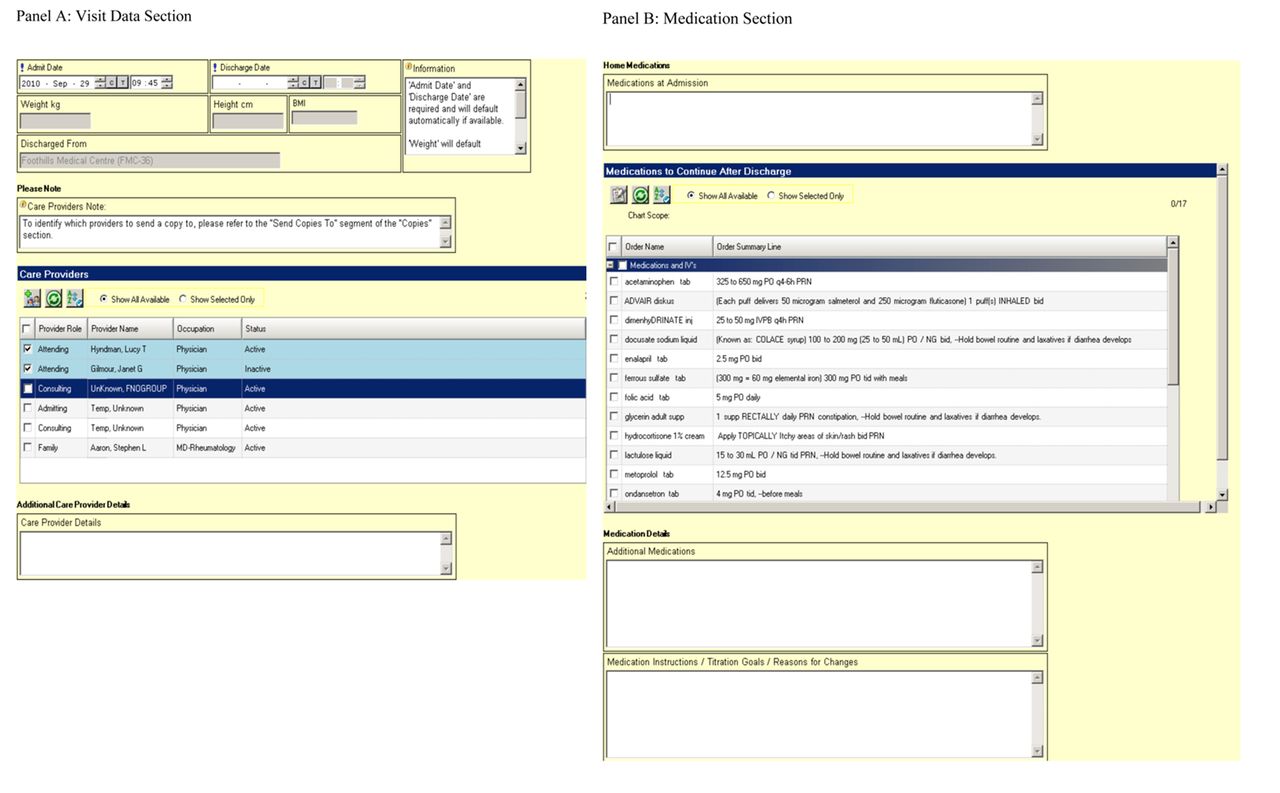
The e-DCT assessed in this study was developed by Alberta Health Services (the province’s health authority) in partnership with a multidisciplinary team at the University of Calgary through iterative consultation with multiple clinical stakeholders and participants/families using ‘vaporware’ prototypes, later integrated into the electronic acute care health information system already in place across Calgary area hospitals (Sunrise Clinical Manager, Allscripts Healthcare Solutions, Chicago, Illinois, USA). The tool that we assessed was pilot-tested with demonstrated positive effects on provider satisfaction and timeliness of information transfer.20–22 Figure 1 shows selected screen shots of the e-DCT.

Screen shot of the electronic transfer-of-care communication tool (A) visit data section and (B) medication section.
The implementation of the tool was accompanied by physician training, and consisted of three strategies: (1) introductory written materials about the tool; (2) formal presentations to physician teams; and (3) daily support. The introductory material included a video guiding users through all aspects of the e-DCT. Training was conducted by health information specialists, and a 24-hour help line was created specifically for the tool’s implementation. In the majority of cases, medical residents generate the e-DCT discharge summaries, with subsequent review of the final version by attending physicians.
The completed e-DCT-generated discharge summaries contain structured content on reason for admission, details of the hospital stay, treatments received and follow-up care required. The e-DCT summaries are instantly uploaded into the provincial health information exchange system, Netcare,23 a province-wide web-based health data repository that is accessible to all community-based providers who would potentially be involved in postdischarge care. Hard copies of the e-DCT discharge summary are provided to patients at time of discharge, with instructions that it should be shared with community providers. In contrast, usual care involved the generation of discharge summaries through dictation and subsequent health records transcription. The key differences between usual care and e-DCT discharge summaries are that the former were often not ready at time of discharge, and that they had unpredictable timing of delivery and non-standardised content and structure. Furthermore, the appearance of dictated usual care discharge summaries on Netcare actually only began sometime after the clinical trial started, and the uploading of such discharge summaries did not occur immediately at time of preparation, but rather after some delay, which in many instances could be some weeks after discharge. The essence of the e-DCT intervention is thus a hybrid of more predictable and timely delivery, and standardised/structured content.
Study participants
Subjects were included if they were admitted to the medical teaching units (MTU). MTU patients have multiple comorbidities and complicated medication profiles. Previous pilot work on the MTU services revealed that approximately one in four patients discharged from the services is readmitted within 3 months.24
Patients were excluded if they were (1) under 18 years; (2) unable to provide contact information; (3) lacking English proficiency and without a family member or friend through whom the team could communicate; (4) enrolled in two or more other studies; (5) unwilling to provide consent; (6) non-Alberta residents (essential for determining follow-up outcomes); (7) previously enrolled in the study; (8) being discharged to hospice; (9) transferred to another hospital; or (10) transferred from the MTU to another service in the study hospital. Patients who died in the hospital or who remained hospitalised without prospects for discharge home were also excluded.
Patient enrolment
Trained research assistants (RAs), who were available to care teams 24/7, consulted MTU charge nurses daily to identify all new admissions as potential study subjects. After confirming eligibility and obtaining consent, RAs collected baseline data including sociodemographic information, admission diagnosis, Charlson Comorbidity Index variables25 and health status via the Health Utilities Index (HUI3).26 All data were collected on a secure, web-based program.27
Randomisation
The web-based data management program also provided the RAs who enrolled participants with a concealed patient allocation tool, derived according to a randomisation sequence generated and maintained away from patient care areas. The randomisation algorithm used permuted variable block sizes. Randomisation occurred as soon as the medical team indicated to the RA an intention to discharge a patient in the upcoming 24–48 hours. Immediately after random allocation, the RA labelled patient charts to inform providers of the assigned method of generating the discharge summaries. In parallel, physicians were contacted via the medical centre paging system to alert them of their patient’s allocation.
Outcome measures
The study’s primary outcome was a composite of death or readmission to any provincial acute-care hospital within 3 months of discharge. This outcome was determined through linkage to data from the Alberta Health Services Data Integration, Measurement, & Reporting unit (to determine readmission), and to data from the Alberta Bureau of Vital Statistics (to determine all-cause mortality). This linkage is the most robust way of determining the occurrence of any readmissions or deaths that occurred with the province, as it avoids reliance on patient self-report, and the potential challenges associated with determining vital status of participants who cannot be reached by telephone.28
The secondary outcomes of interest were the occurrence of patient-reported adverse outcomes (PRAOs) (ie, any undesirable health issues reported by the patient after hospital discharge) and adverse events (the subset of PRAOs that were independently judged by physician raters to be linked to problems with medical management) at 30 days postdischarge.29 This was determined using a validated method described by Forster and colleagues.1 2 At 30 days, a trained investigator, blinded to patient group assignments, conducted a telephone follow-up interview, asking participants about any adverse health issues and details surrounding these. These were later categorised by physician reviewers as being either a ‘worsening condition’ relating to the problem for which they were hospitalised and/or a ‘new condition’. Raters also judged whether these were preventable and/or ameliorable events. The team of physician raters consisted of two Royal College-certified internal medicine specialists and a College-certified family physician. Two physician raters, blinded to group assignments, independently reviewed each patient-reported adverse event, and disagreements were resolved through consensus discussion or by a third rater when necessary.29
Statistical analysis
A pilot study conducted on the MTU services demonstrated that 23% of patients discharged were readmitted to hospital.24 Based on this, we estimated an absolute event rate of 25% in the control group for the composite of death or readmission. Using 80% power and a type I error rate of 5%, we required 686 participants per group to allow detection of a 25% relative reduction in the primary outcome in the intervention group. The latter relative risk reduction target was selected based on our finding in the literature of >30% relative reductions in readmissions seen in prior discharge intervention studies assessing electronic discharge summaries (Casas et al 30) and a transition coaching intervention (Coleman et al 31). With inflation for loss-to-follow-up and dropouts, the study protocol thus called for enrolment of 700 participants per group. The unit of analysis was individual patients, not physicians.
We used t-tests for comparison of continuous variables between groups, and χ2 and Fisher’s exact tests to compare categorical variables including the outcomes of readmission or death and postdischarge adverse events. For readmitted participants, we used t-tests to compare the length of stay for the two groups. A Kaplan-Meier analysis with log-rank test was used to assess event-free survival for the primary endpoint of death or hospital readmission, and a proportional hazards analysis was used to determine HRs, adjusting for age, sex and comorbidities. All analyses were conducted using SAS V.9.2. Subgroup analyses were conducted to assess the effect of the e-DCT intervention stratified by age, sex and phases of study (earlier vs later enrolment in the study). These were not prespecified subgroup analyses in our protocol, but they were conducted (with appropriate interpretive caution) because the study team received queries on their potential impact from various study stakeholders. All analyses were by intention-to-treat. CONSORT trial reporting guidelines were followed.32
Results
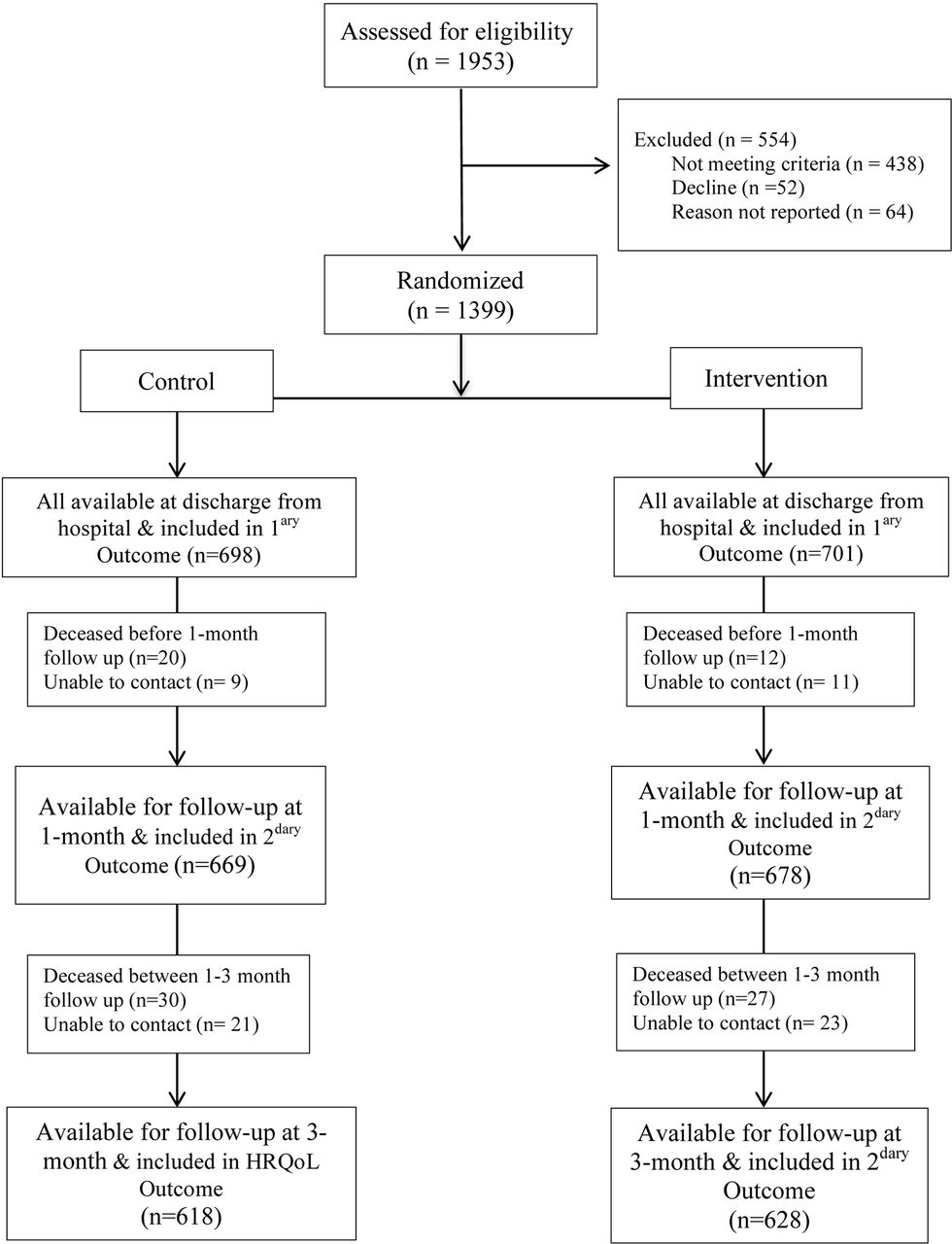
From January 2012 to December 2013, we approached 1953 patients, of whom 1399 were randomised. Among these, 701 were assigned to the e-DCT intervention group and 698 to the control group (figure 2). Through careful study oversight, all patients remained true to their group assignments and had their discharge summaries generated by the assigned method. Further, all of the 1399 randomised participants were available for data linkage for determination of the primary outcome within 90 days. Due to early postdischarge deaths (32) and some losses to follow-up (20), smaller numbers were available for the telephone interview to determine PRAOs and adverse events at 30 days (n=1347), and participants’ health status assessments at 90 days (n=1246) (figure 2).

CONSORT flow chart.
Baseline characteristics of participants were similar between groups (table 1). Participants had a mean age of 59 years, 50% were male and 78% were Caucasian. Most of the participants had more than one comorbidity (84%); diabetes mellitus was the most common comorbid condition. There was a slightly greater proportion of men in the usual care group, but patient characteristics were generally evenly balanced between groups. Patient severity of illness is reflected by their generally low mean HUI3 quality of life scores.26
Patient characteristics in the two study groups
Table 2 displays the results for outcomes at 7, 15, 30 and 90 days. The primary outcome of death or readmission at 90 days occurred in 230 of 701 (32.8%) of the e-DCT group and in 205 of 698 (29.4%) in the usual care group (p=0.166). Of note, components of the composite primary endpoint were divergent. At each time point, readmissions were nominally higher for e-DCT versus usual care, while deaths were lower for e-DCT relative to usual care.
Primary outcomes for participants discharged using the e-DCT versus usual care
Figure 3 displays Kaplan-Meier event-free survival curves for the composite primary endpoint (A) and for all-cause mortality (B). There was no statistically significant difference between the time-to-event curves extending to 90 days for the composite primary endpoint (A: p=0.166) nor for the endpoint of all-cause mortality (B: p=0.153). The previously mentioned divergence of the components of the composite primary endpoint is again apparent in figure 3. There was similarly no statistically significant difference between the groups for the secondary outcome of PRAOs, reported in 239 of 678 contacted subjects (35.3%) in the e-DCT group and in 227 of 669 (33.9%) of the usual care group (p=0.611) (table 3). The secondary outcome of adverse events (adjudicated by physician outcome assessors), meanwhile, occurred in 14 of 678 (2.1%) of the e-DCT group and in 12 of 669 (1.8%) of the usual care group (p=0.788). At 90 days, there was no difference between the groups for quality of life scores or for length of stay of readmissions (table 3).

Kaplan-Meier plots for the electronic discharge communication tool (e-DCT) versus usual care groups: (A) readmission or death and (B) death.
Secondary outcomes for participants discharged using the e-DCT versus usual care
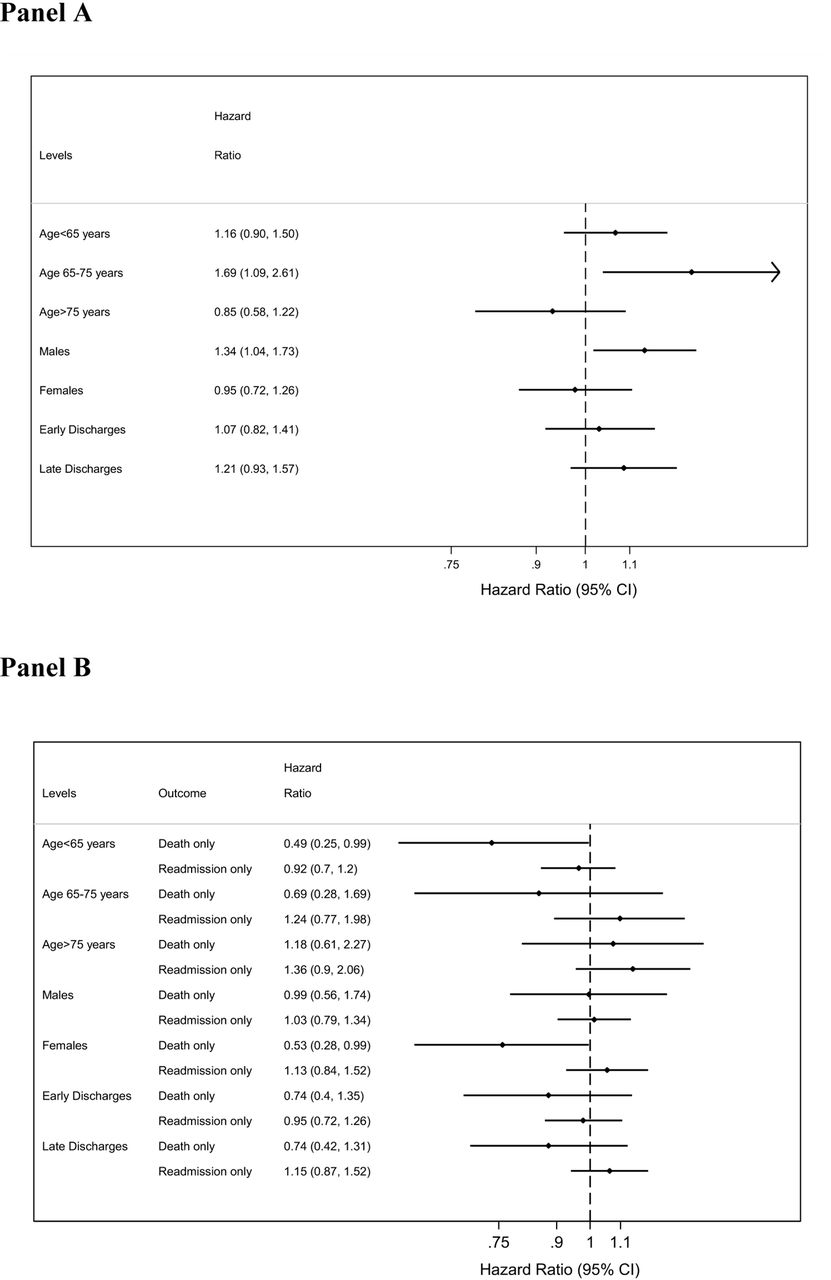
Subgroup analyses (figure 4) assessed the effect of the e-DCT intervention stratified by age, sex and phases of study (earlier vs later enrolment in the study). There were no differences in study findings across the stratification variables for the primary composite endpoint (A), but the analyses for death and readmission analysed separately (B) again reveal divergence on how e-DCT relates to the death versus readmission components of the study’s composite endpoint.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Subgroup analyses stratified by age, sex and phases of study (earlier vs later enrolment in the study): (A) HR for combined outcome at 90 days and (B) HR for death and readmission separate endpoints at 90 days.
Discussion
This large randomised e-health intervention clinical trial assessed the efficacy of an e-DCT with sufficient power to determine whether the intervention reduces the composite of hospital readmission or death, as well as other postdischarge adverse events. This e-DCT was developed in an attempt to improve timely delivery of patient discharge information, including relevant information on patient stay, medication reconciliation and follow-up care instructions. As mentioned, our clinical trial builds on knowledge produced in our previous studies, which included a systematic review of related literature19 and a pilot study demonstrating high quality of discharge summaries and patient and provider satisfaction.20 22 Despite these previously demonstrated benefits of the e-DCT, the findings of this study reveal that the e-DCT did not reduce the composite endpoint of death or readmission within 90 days of hospital discharge.
Our neutral overall study finding in a large well-powered clinical trial assessing death or readmission after hospital discharge is not an isolated one. Recently, Dhalla et al 33 conducted a similarly large clinical trial testing the ‘Toronto virtual ward’, an intervention that involved a multidisciplinary team caring for complex individuals discharged home after inpatient internal medicine hospital stays. The ‘Toronto virtual ward’ did not produce any significant reduction in the composite of death or readmission at 30 days. In contrast, there are some interventions that have yielded positive results in reducing readmissions.33 34 Coleman et al 33 designed an intervention consisting of patient and caregiver engagement strategies, which included support by a ‘transition coach’. This intervention resulted in a reduction in readmission rates extending to 30 days after hospital discharge. A similar result is reported by Shu et al, 34 who evaluated an integrated programme including a disease-specific care plan, follow-up phone calls, hotline counselling and referral to a hospitalist-run clinic, and found a significant decrease in readmission and mortality within 30 days of hospitalisation.
In light of these various studies, we are left to ponder why some interventions reduce readmissions and others fail to do so.35–37 One potential explanation is the varying intensity of the various complex interventions tested across studies. Our e-DCT intervention is certainly much less intensive than those tested in the other three studies just discussed above. Our prior systematic review of similarly light-intensity electronic discharge summary interventions19 revealed a small number of underpowered intervention studies assessing impact on hard clinical endpoints; only one by Casas et al 30 revealed a significant reduction in readmission. The important caveat to the other negative studies identified in our systematic review for these endpoints is that they were underpowered to assess death and/or readmission as endpoints.
Yet another consideration is our choice of primary endpoint. The death or readmission composite is an endpoint that has been quite popular in studies assessing interventions seeking to reduce readmission to hospital.31 33–35 38 39 However, our findings raise the possibility of divergence of the death and readmission components of the composite primary endpoint. This raises both methodological and clinical questions of importance to any potential studies assessing such interventions. Methodologically, these findings suggest that future studies should carefully consider the use of a death-or-readmission composite as the components of the composite should be of equal relevance to patients, they should occur with similar frequency, and they should be affected to a similar degree and in the same direction by the intervention being tested.40 41 From a clinical standpoint, there are plausible reasons for divergence of the death and readmission endpoints. Some readmissions are planned, and even when they are not planned, they may often be entirely appropriate and could contribute to preventing clinical deterioration and death. Indeed, readmissions may often arise from more diligent outpatient clinical follow-up by community providers who have received discharge communications from hospital-based providers outlining parameters requiring close observation.42 Future large-scale studies assessing interventions for better transitions of care should perhaps be designed to be even larger than this study, so that there is sufficient statistical power to assess effects on mortality alone.
Our study has limitations. First, individual participants were the units of analysis and randomisation. The advantage of this approach is that it produced two study groups of almost identical size and clinical characteristics. The downside was the potential for contamination, with participants in the usual care arm benefiting from more attentive discharge planning than they might have otherwise had if there had not been an ongoing study focusing on transitions of care. In our study, both usual care and e-DCT intervention groups received careful discharge planning from a nurse care transition coordinator — a control group cointervention that might have reduced the potential incremental value of the e-DCT intervention. An alternative approach would have been to randomise clusters (either the large MTU teams or individual physicians). However, the small number of clusters available to us would have limited our ability to ensure balanced clinical characteristics and symmetry in the size of the two study arms. A second limitation is that we do not have ‘under-the-hood’ mechanistic information for patients in this trial on the timing of community physician access to the discharge summary, nor patient-level information on the use versus non-use of Netcare by community providers. It would be very helpful to have this information on trial patients to better understand our neutral trial result (eg, is the neutral result present because community physicians did not access Netcare at all?). Mitigating this limitation is one important known fact: All e-DCT patients leave hospital with a hard copy of their discharge summary in hand, with explicit instructions to deliver that hard copy to their community providers. That is an ancillary form of information transfer (over and above immediate availability on Netcare) that did not occur with usual care. A third general limitation to mention for such studies is that the interventions being tested are complex ones that are subject to context dependency; the demonstration of benefit in one context does not generalise to other jurisdictions.
Conclusion
Based on our study, what should healthcare systems do based on the current state of knowledge? Should innovation like ours be adopted? Strictly speaking, this clinical trial reports a neutral result, and one potential interpretation to draw from this is that an e-DCT-like intervention should not be adopted because our study reveals no apparent benefit to hard clinical outcomes. However, although the primary composite endpoint did not differ between e-DCT and control participants, this does not mean that organisations should not adopt an e-DCT. It may be that hard clinical endpoints are too far downstream to be influenced by an electronic discharge summary. The e-DCT produces more complete discharge summaries, in a more timely manner and with a high level of satisfaction among both sending and receiving physicians.20 22 These more proximal outcomes are of value to patients and providers. As a testimonial of potential interest to health systems elsewhere, the hospital network in which this study was undertaken is maintaining its support of the e-DCT for now widespread use, and is in fact developing other similar structured e-health clinical notes for interhospital transfers, interward transfers and intensive care unit discharges. Furthermore, this novel e-DCT is relevant to a much wider audience than to the Canadian hospitals where it is currently deployed, as it was developed on the internationally available Allscripts hospital information system platform that is used in many hospitals worldwide.
The e-DCT tested did not reduce the composite endpoint of death or readmission at 90 days, nor the incidence of patient-reported adverse events at 30 days. This neutral finding for hard clinical endpoints needs to be considered in the context of increased patient and physician satisfaction, and high quality of discharge summaries.
Acknowledgments
We would like to acknowledge the in-kind contributions of the following individuals to the project:From the W21C Research and Innovation Centre -- Shandra Harman and Barbara Artiuch; from the Clinical Research Unit at the University of Calgary -- Mark Lowerison; from the Medical Teaching Unit at Foothills Medical Centre -- Sonia Morrison, Rhonda Niebrugge, and Olivia Muir; from Alberta Health Services -- Chris Klotz and Janice Mandolesi who supported the implementation of the e-DCT tool. Finally, we would like to thank the patients for volunteering to be part of this study. No one mentioned herein received additional remuneration for participating in the research or helping in the editorial process.The e-DCT Team: Barbara Okoniewska, Nancy Clayden, Katherine Skora, Aida Raissi, Wrechele Ocampo, Murtaza Dahodwala, Chloe de Grood, Carmel Steinke, Jill de Grood.
References
Footnotes
Contributors Drs. Santana and Ghali had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.All authors satisfy the criteria for authorship relating to study concept and design, acquisition and analysis of data, drafting and revising the manuscript, statistical analysis, funding and materials support and study supervision. Studyconcept and design: Ghali,Holroyd-Leduc, O’Brien, Flemons, White and Forster Dataacquisition included research assistants: Okonieswka, Clayden,Skora, Raissi, Ocampo, Dahodwala and de Grood. Drafting of the manuscript: Santana,Southern, Ghali. Critical revision of the manuscript for intellectualcontent: all authors. Statistical analysis: Southern, Santana, Ghali. Obtained funding: Ghali, Holroyd-Leduc,O’Brien, Flemons, White and Forster Administrative, technical, or material support: Steinke and de Grood. Study supervision: Santana, Ghali, Holroyd-Leduc,O’Brien, Flemons, Hill, White and ForsterAll authors have read and approved the final paper.
Competing interests None declared.
Patient consent This article does not contain personal medical information about an identifiable living individual, and therefore does not require the patient’s explicit consent before we can publish it.
Ethics approval The study was approved by the Conjoint Health Research Ethics Board at the University of Calgary.
Provenance and peer review Not commissioned; externally peer reviewed.