Article Text

Abstract
Background Medication non-adherence in ambulatory care has received substantial attention in the literature, but less so as it affects acute care. Accordingly, we aimed to estimate the frequency with which non-adherence to medication contributes to hospital admissions.
Methods We searched the Cochrane Library, EMBASE, Cumulative Index to Nursing and Allied Health Literature, International Pharmaceutical Abstracts and PubMed (until December 2017) to identify prospective observational studies that examined prevalence rates of hospital admissions associated with medication non-adherence. A quality assessment was performed using an expanded Crombie checklist. Data extraction covered patterns, circumstances, and patient and other key characteristics of non-adherence. Pooled estimates were obtained using a random-effect model.
Results Of 24 included studies, 8 were undertaken in North America, 7 from Europe, 6 from Asia and 3 from Australia. Most studies (79%) were rated as low risk of bias. All but three studies used combination measures to detect non-adherence, but approaches to assess preventability varied considerably. Across the studies, there was high heterogeneity among prevalence estimates (χ2=548, df 23, p<0.001, I2=95.8%). The median prevalence rate of hospital admissions associated with non-adherence was 4.29% (IQR 3.22%–7.49%), with prevalence rates ranging from 0.72% to 10.79%. By definition, almost all of these admissions were considered preventable. The underlying causes contributing to these admissions included medication cost and side effects, and non-adherence most often involved cardiovascular medicines.
Conclusions Hospital admissions associated with non-adherence to medication are a common problem. This systematic review highlights important targets for intervention. Greater attention could be focused on adherence to medication during the hospital stay as part of an enhanced medication reconciliation process. Standardisation in study methods and definitions is needed to allow future comparisons among settings; future studies should also encompass emerging economies.
- adverse events, epidemiology end detection
- hospital medicine
- medication safety
- patient Safety
- compliance
Statistics from Altmetric.com
- adverse events, epidemiology end detection
- hospital medicine
- medication safety
- patient Safety
- compliance
Introduction
Adherence is defined as ‘the extent to which a person’s behavior, (taking medication, following a diet, and/or executing lifestyle changes) corresponds with agreed recommendations from a health care provider’.1 However, non-adherence to medication is common among patients with long-term conditions, which can negatively affect their health outcomes. Previous studies have suggested that 25%–90% of non-adhering patients experienced treatment failure and for some leading to hospitalisation.2–4 This accounts for significant healthcare costs, estimated as exceeding $100 billion annually, to the US economy.5 6
Several studies have examined the prevalence and nature of hospital admissions associated with medication-related problems.7 8 Around 5%–10% of hospital admissions are thought to arise from such problems,9 10 often due to adverse drug reactions or adverse drug events.8 11 However, far less is known about the role of medication non-adherence that leads to hospital admissions, and the associated risk factors. To our knowledge, no systematic review has yet quantified the prevalence of hospital admissions that are a consequence of non-adherence to medications. Therefore, this systematic review and meta-analysis of prospective observational studies aimed to determine these aforesaid prevalence estimates and the nature of medication non-adherence leading to hospital admissions.
Methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines12 and registered with the International Prospective Register of Systematic Reviews (PROSPERO number: CRD42017083688).
Study outcome
The prevalence of hospital admissions associated with non-adherence to medications was defined as our primary outcome.
Data sources and study selection
Inclusion criteria
The following criteria were used for including studies in our systematic review: (1) studies were prospective and observational, and provided sufficient data to calculate the prevalence of hospital admissions associated with medication non-adherence; (2) patients could be admitted to any hospital department, including admission via emergency departments. There were no restrictions on the definition of (non)-adherence used in the studies.
Exclusion criteria
We excluded studies that investigated the prevalence of hospital admissions arising from non-adherence to specific medications or for specific diseases. Case reports, case series, editorials and review articles were also excluded.
Search strategy
We searched the following bibliographic databases from their inception dates until December 2017: Cochrane Library, EMBASE, Cumulative Index to Nursing and Allied Health Literature, International Pharmaceutical Abstracts and PubMed. The search strategy included the following keywords and their synonyms: (‘patients’ OR ‘human’) AND (‘drug-related problem’ OR ‘adverse drug events’ OR ‘non-adherence’) AND (‘incidence’ OR ‘prevalence’). The literature retrieval was supplemented by manually searching the reference list of all identified articles. There were no language restrictions.
Screening process
Eligible titles/abstracts and full-text articles were screened by two independent investigators (PM and CK). Inter-reviewer agreement for study selection was assessed using the Cohen’s kappa statistic. Any disagreements were resolved through discussion.
Data extraction and methodological quality assessment
Studies meeting the eligibility criteria were extracted independently by two investigators (PM and CK) using a predesigned extraction form. The following information was extracted: country of study, study setting, study year, study period, population, participant ages, percentage of men, definitions of medication non-adherence, method for detecting medication non-adherence, implicated medications classified according to the British National Formulary classification system,13 causality assessment, preventability, reasons for medication non-adherence and prevalence rates for hospital admission related to medication non-adherence. Reasons for medication non-adherence that led to hospital admissions were classified into three groups: patient-related factors, healthcare professional-related factors and healthcare system-related factors. We also contacted authors when primary outcome data were missing. If the authors did not respond, the study was excluded. Inter-reviewer agreement for extracting prevalence rates was assessed using the Cohen’s kappa statistic and disagreements were resolved by discussion.
Two investigators (PM and CK) independently appraised the risk of bias for the included studies using the Crombie checklist, which is applicable for cross-sectional/prevalence studies.14 The operationalisation of the Crombie tool, specifically for prevalence studies, is provided in online supplementary etable 1. Each item was scored 1 point for ‘yes’, 0.5 points for ‘unclear’ and 0 point for ‘no’. Studies were then classified as having high risk of bias if the summary score was 0 to <4 points, moderate risk of bias if 4 to <7 points and low risk of bias if 7–9. Inter-reviewer agreement for quality assessment was assessed by the Cohen’s kappa statistic and disagreements resolved by discussion.
Supplementary file 1
Data analyses
The prevalence of hospital admissions associated with non-adherence was calculated as the number of patients who had medication non-adherence that required hospital admission (the numerator) divided by the number of patients admitted to hospital during the study period for any medical cause (the denominator). Pooled-effect estimates for the prevalence rate of hospital admissions associated with medication non-adherence across the included studies with corresponding 95% CIs were calculated using the DerSimonian-Laird random-effects model, assuming that the true effect size varies between studies.15 To assess heterogeneity of prevalence rates among studies, we used standard χ2 tests and the I2 statistic. If high heterogeneity was indicated (I2≥75%), the results across studies were summarised using the median rate and IQR. To explore possible sources of heterogeneity, subgroup analyses were performed by study population (children, all-age group and elderly), geographical region (North America, Europe, Asia and Australia) and method of detection (combination vs single measures), to investigate the impact on the prevalence rates of hospital admission associated with medication non-adherence. In addition, heterogeneity was also explored in a univariate random-effects meta-regression. The following variables were included: publication year, study population, geographical region and method of detection ((1) an interview method, (2) a combination of medical record review and drug level analysis, (3) a combination of medical record review, drug level analysis and interview methods, (4) medical record review only, (5) a combination of medical record review and interview methods, and (6) a combination of medical record review, interview and pill count methods). A funnel plot was used to investigate any evidence of publication bias. We also tested for funnel asymmetry using the Begg’s test, Egger’s tests and the trim-and-fill method (all p<0.05).16–18 Statistical tests were two-sided and used a significance threshold of p<0.05. All analyses were performed using STATA V.14.1 software.
Results
Search results
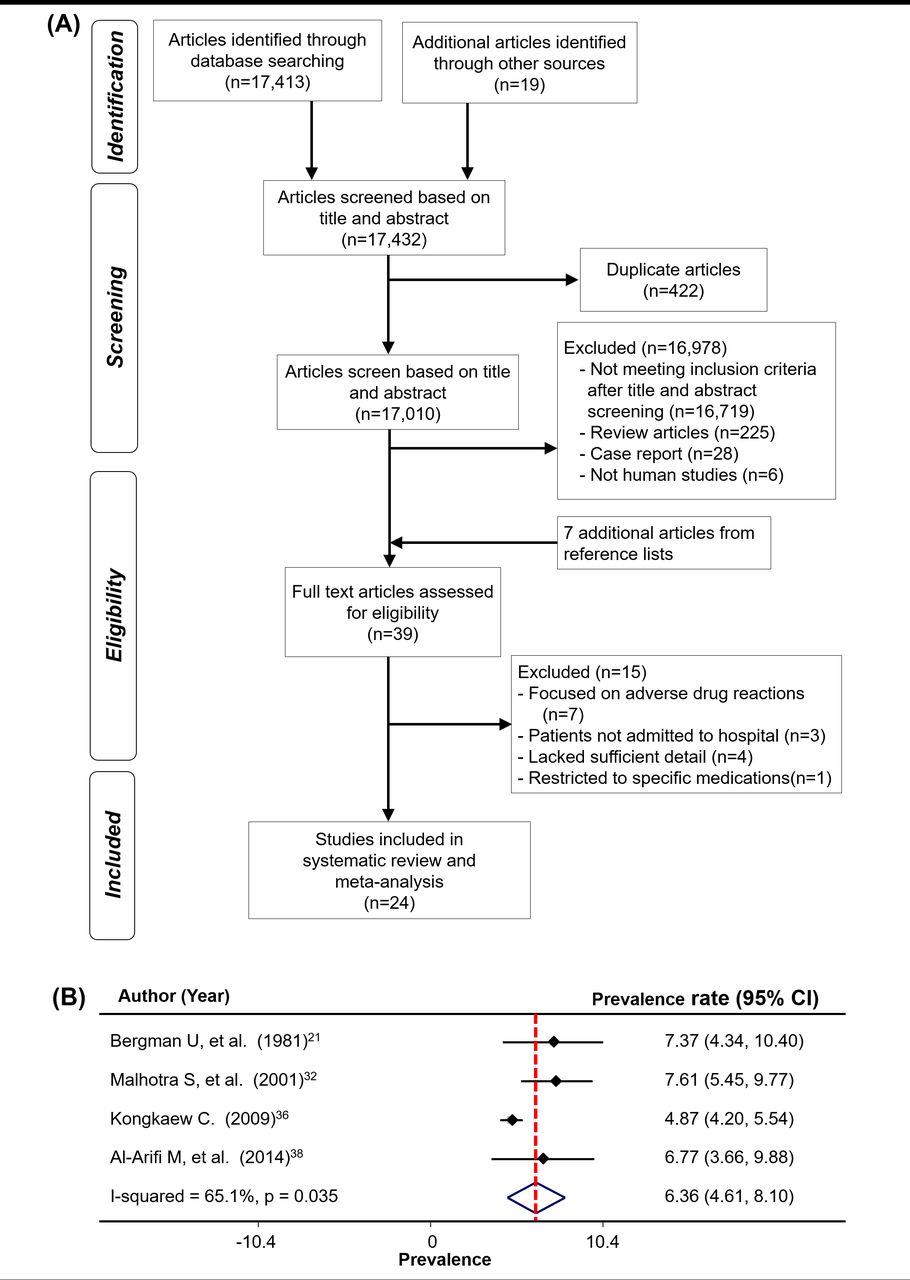
From all sources, 17 432 articles were identified. After removing duplicates, 17 010 articles remained. Of these, 16 978 were removed because they (1) did not meet the inclusion criteria after screening (16 719 articles); (2) were review articles (225); (3) were case reports (28); or (4) were not related to humans (6). Seven additional articles were identified by hand-searching. The remaining 39 full-text articles were assessed for eligibility and 15 articles were excluded because they focused on adverse drug reactions (7 articles); patients were not admitted to hospitals (3 articles); had insufficient data to calculate prevalence rates of non-adherence to medications (4 articles); and were related to specific medications (1 article). In all, 24 studies2 19–41 were included in the systematic review and meta-analysis (figure 1A). The inter-reviewer agreement was deemed good for full-text screening (Cohen’s kappa value=0.72) and very good for data extraction on prevalence rates (Cohen’s kappa value=1.0).
{kind=link}
All the included studies (n=24) were prospective and observational that investigated hospital admissions related to medication non-adherence. They were conducted in North America (8 articles), Europe (7), Asia (6) and Australia (3). Three studies36 39 40 (12.5%) were multicentre. In 21 studies2 19–22 24–29 31–39 41 (87.5%) employing combination measures, four different approaches for detection of non-adherence were identified: (1) a combined review of medical records and blood drug concentrations; (2) a combined review of medical records, drug concentrations and interview; (3) a combined review of medical records and interview; and (4) a combined review of medical records, interview and pill count. In 18 studies that reported definitions of medication non-adherence, four studies21 32 36 38 used the Haynes definition,42 one39 applied the WHO definition,1 one37 used Hepler and Strand,43 and the remaining studies created their own definitions. For the type of population, 17 studies19–21 23 24 26 28–30 33–39 41 were conducted on general populations, six in the elderly,2 25 27 31 32 40 and one in a paediatric population22 (table 1). Eleven studies2 24–27 31 32 35 37 40 41 reported the mean number of medications prescribed to each patient, which ranged between 2.524 and 9.0.41 Two studies25 31 merely reported that patients admitted to hospital had at least two to four medical conditions/person. Many patients (14%–45%) were living alone.2 32 40 In addition, four studies (16%) reported that more than 50% of the patients had not completed education to high school level or above.2 32 37 39
Characteristics of 24 included studies
Quality assessment and publication bias
The Crombie tool for quality assessment yielded scores ranging from 4 to 9. Nineteen studies2 21 23–29 31–37 39–41 were classified as low risk of bias, five19 20 22 30 38 were moderate risk of bias and none was classified as high risk of bias. Here, the agreement for each item ranged from 0.78 to 1.00. However, when making an overall risk of bias judgement according to the range of summary scores, the agreement between reviewers was judged as very good (Cohen’s kappa=1.0) (online supplementary etable 2). Six studies2 25 31 33–35 met all nine domains on critical appraisal of prevalence studies. Most studies clearly stated the aims of the study, employed an appropriate design to meet the objectives, and adequately described the data in terms of method of participant selection, study location and study duration. Seventeen studies (70.8%) reported statistical methods used for data analysis. Twenty-one studies (87.5%) used combination methods for measuring medication non-adherence. Sixteen studies (66.7%) employed a method to evaluate the causal relationship between admissions and non-adherence (online supplementary etable 2).
No evidence of publication bias was detected by Begg’s test (p=0.36) and Egger’s test (0.066). The findings were not different after calibrating for publication bias by performing the trim-and-fill method. The corresponding funnel plot is displayed in online supplementary eFigure1.
Prevalence of hospital admissions associated with medication non-adherence
The 24 studies included 26 496 patients, of whom 999 experienced non-adherence to medications. The crude prevalence rates of hospital admissions associated with non-adherence varied from 0.7% to 10.8%. Given the high heterogeneity (χ2=548, df 23, p<0.001, I2=95.8%), the prevalence rate of hospital admissions associated with non-adherence was reported as a median of 4.3% (IQR 3.2%–7.5%). All 24 studies also reported the number of patients admitted to hospital due to medication-related problems (3354 patients). Of these admissions, 29.4% (as a median prevalence rate, IQR=17.0%–39.2%) were associated with medication non-adherence (heterogeneity: χ2=2761, df 23, p<0.001, I2=99.2%).
The evaluation of causality between hospital admissions and medication non-adherence was carried out in 16 studies2 21 23–26 28 29 31–36 39 40 based on explicit criteria and/or the judgement of reviewers. The non-adherence was classified as causal non-adherence if the causality was rated as definite/probable in 10 studies.2 21 23 26 29 34–36 39 40 The most common explicit criteria used to assess causality was the Hallas criteria44 employed in six studies,26 27 29 31 33 36 followed by the WHO criteria45 46 (two studies24 40), the Karch-Lasagna algorithm47 (two studies28 34), and the Bergman and Wiholm algorithm21 (two studies21 25). The remaining criteria2 32 48 of included studies are described in table 2.
Causality and preventability of hospital admission associated with medication non-adherence
Eleven studies23 27 28 31 33 35–39 41 (45.8%) estimated the preventability of hospital admissions associated with medication non-adherence, giving an overall median preventable rate of 100% (ranging from 29.5% to 100%). The criteria used27–29 43 44 49–51 and how preventability were judged are given in table 2 and online supplementary etable 3.
Subgroup analyses
In subgroup analyses, the median prevalence of hospital admission for the elderly was 5.1% (IQR 3.8%–7.6%) and that for all-age patients was 4.4% (IQR 1.6%–7.4%), while the mean prevalence for paediatric patients was 3.4% (95% CI 2.2% to 4.6%).
Geographically, eight studies originated from North America,2 19 20 23 25 27 29 35 where the median prevalence was highest (7.2%, IQR 3.8%–10.7%), six were from Asia22 30 32 37–39 (median prevalence=5.1%, IQR 1.5%–7.6%), seven from Europe21 24 33 34 36 40 41 (median prevalence=4.4%, IQR 3.8%–5.5%), while the lowest prevalence rate was from three Australian studies26 28 31 ((pooled mean 1.7%, 95% CI 0.9% to 2.5%) with a moderate degree of heterogeneity (I2=37.2%, p=0.20)) (table 3).
Subgroup analysis according to population, continent and method of detection
Detection using combination measurements yielded a median prevalence of 4.4% (IQR 3.0%–7.4%) and a similar value when single measures were employed (4.2%, 95% CI 3.8% to 9.5%). Fourteen different definitions of non-adherence were identified. Four studies21 32 36 38 found prevalence estimates of 6.4% (95% CI 4.6% to 8.1%, p=0.035, I2=65) (figure 1B) by using the Haynes definition,42 which was the first to be introduced into medicine.52
Meta-regression
Geographical regions and method of detection were related to admission rates, while age group and year of publication were unrelated (online supplementary etable 4).
Reasons and risk factors for medication non-adherence
Five studies2 22 24 31 32 identified the causes of medication non-adherence by conducting an interview. The reported reasons for medication non-adherence were classified into three categories: (1) patient-related, (2) healthcare professional-related and (3) healthcare system-related (shown in table 4).
Reasons for medication non-adherence that led to hospital admissions
Two studies2 32 identified risk factors for hospital admissions associated with non-adherence which were poor recall of the medication regimen,2 32 multiple consulting physicians,2 32 female gender,2 32 medium income ($10 000–$15 000 per year) compared with those on public assistance (Medicaid)2 and a greater number of medications prescribed.2 32
Medication classes involving non-adherence
Twelve (48%) studies2 19 20 22 24 26 28 32–34 36 40 reported the medication class associated with hospital admissions due to medication non-adherence. Those most commonly involved targeted the cardiovascular system (50.9% (IQR 39.6%–58.9%)) (n=8),2 19 22 24 26 28 32 33 respiratory system (24.2% (IQR 8.7%–33.3%)) (n=7),2 19 24 26 28 32 33 central nervous system (15.4% (IQR 6.7%–22.6%)) (n=6),19 20 22 28 32 33 endocrine system (9.1% (IQR 5.6–20)) (n=6)2 19 20 28 32 33 and medication used to treat infections (4.3% (IQR 2.2%–64.5%)) (n=3).19 22 33 Other medication classes reported were analgesics, gastrointestinal drugs, haematology drugs and nutrition preparations, but their rates for non-adherence were not stated (table 1).
Discussion
This systematic review and meta-analysis found that medication non-adherence accounted for 4% of all hospital admissions or 29% of all medication-related problems. These findings are similar to admission rates due to adverse drug reactions, which are considered a major healthcare burden,8 11 equally reflecting the importance of medication non-adherence to patient safety.
It is noteworthy that hospital admissions due to non-adherence were judged as almost always preventable largely by definition. In practice, this is an area that requires high priority attention. Our findings indicate potential at-risk groups, such as (1) patients having poor recall of their medication regimen, (2) those who consult multiple physicians, (3) those receiving polypharmacy, and (4) as in previous reports,53–55 patients whose medication treats cardiovascular, respiratory and infectious diseases remain a problem. Appropriate and effective interventions are needed, but so far no single intervention strategy or package of strategies has led to large improvements of adherence across all patients, conditions and settings.1 56 Nevertheless, a multiplicity of approaches is likely to have worthwhile gains. Pharmacist-led interventions in England delivered by telephone has recently demonstrated useful improvements in adherence.57–59 Considerable evidence has accumulated suggesting that interventions tailored to individual patients together with support from family, community, patient organisations or healthcare professionals trained in adherence management are required for improving medication non-adherence.60 61 In addition, since medication reconciliation has shown promising benefits in reduction of the rate of all-cause readmissions or all-cause emergency department visits,62 actions to improve medication adherence during hospital stay as part of an enhanced medication reconciliation process should be explored further. However, evidence from robust cost–benefit analyses demonstrating improvements in patients’ quality of life is needed to demonstrate both clinical and cost-effectiveness of such interventions in routine clinical practice.
The observed prevalence rates of hospital admissions associated with medication non-adherence were influenced by several factors, which influenced the marked heterogeneity between studies, including the geographical region and method of detection. Another known factor is the non-uniformity in the terminology and definitions of non-adherence, which is in line with another systematic review where a taxonomy for describing and defining adherence to medications was proposed.52 According to this taxonomy, adherence to medications is further divided into three quantifiable phases: ‘initiation’, ‘implementation’ and ‘discontinuation’. To our knowledge, no study has yet explicitly reported the risk of hospital admissions using these phases. Therefore, we suggest that future studies should look into this issue, especially the risk of hospital admissions due to poor implementation versus non-persistence. Other possible patient-level sources of heterogeneity that were identified previously are likely to include the complexity of the medication regimen, level of education and underlying medical conditions.63
This study has some limitations. First, the included primary studies differed in methodology. This could affect the estimation of prevalence rates. Second, few studies reported the number of medications, number of comorbidities, family/society support and reasons for non-adherence, although these factors were cited as important factors affecting non-adherence.64 Finally, we observed (1) variations in how non-adherence was measured and (2) small sample sizes in some subgroup analyses. Such variation in methods, and rather small subgroups, may compromise their interpretation. We suggest that further studies aiming to investigate the prevalence and nature of hospital admissions related to medication non-adherence should include the following minimum characteristics: (1) clearly defined terms describing medication non-adherence,52 (2) clearly provide the number of patients who were non-adherent and the total number of admissions, (3) apply explicit criteria for assessing causality by experts, and (4) use a validated tool for measuring non-adherence to medication.
Our study had several important strengths. It is the first systematic review and meta-analysis estimating the prevalence and nature of hospital admissions associated with medication non-adherence. We undertook an extensive search to ascertain that the included studies were representative: this involved searching a wide range of international bibliographic databases, hand-searching for unpublished articles and without language restrictions. In the absence of information in individual studies, we also contacted the study authors for additional data. The agreements between reviewers were rated as ‘good’ for full-text screening and ‘excellent’ for extracting prevalence rates and overall quality assessment. The results presented no evidence of publication bias. In addition, we used an explicit criterion (ie, the modified Crombie scale) to critique study quality.14 Finally, our study adheres to the standard methodology of systematic review and meta-analysis as required by the Cochrane and PRISMA checklists.12 65
Conclusions
Hospital admissions associated with medication non-adherence were a common problem. Almost all were preventable by definition and surpass estimates of preventable admission rates due to adverse drug reactions. Medications commonly involved included those used to treat cardiovascular and respiratory disorders, and infections. Future research and implementation should (1) determine the most effective strategies to minimise unnecessary hospital admissions due to non-adherence to medication, thereby improving patient safety, (2) have robust study designs that fulfil our quality checklist, and (3) encompass emerging economies.
References
Footnotes
Contributors DMA and CK conceptualised the study. PM and CK performed the searches, screened all the titles and abstracts for compliance with the inclusion criteria, reviewed full-text articles of the potential studies, and completed data extraction. All included studies were assessed for methodological quality by PM and cross-checked by CK. PM and CK drafted the manuscript. CNS, DMA and CK extensively revised the manuscript. All authors have read and approved the final manuscript.
Funding Financial support from The Thailand Research Fund through the Royal Golden Jubilee PhD Program (Grant No PHD/0197/2557) and Naresuan University Research Fund (R2559C244) is gratefully acknowledged.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.