Article Text

Abstract
Background The discharge letter is the primary means of communication at patient discharge, yet discharge letters are often not completed on time. A multifaceted intervention was performed to improve communication in patient hand-off from the intensive care unit (ICU) to the wards by improving the timeliness of discharge letters.
Methods A management directive was operationalised by a working group of ICU staff in a longitudinal before–after study. The intervention consisted of (a) changing policy to require a letter for use as a transfer note at the time of ICU discharge, (b) changing the assignment of responsibility to an automatic process, (c) leveraging positive peer pressure by making the list of patients in need of letters visible to colleagues and (d) provision of decision support, through automatic copying of important content from the patient record to the letter and email reminders if letters were not written on time. Statistical process control charts were used to monitor the longitudinal effect of the intervention.
Results The intervention resulted in a 77.9% absolute improvement in the proportion of patients with a complete transfer note at the time of discharge, and an 85.2% absolute improvement in the number of discharge letters written. Statistical process control shows that the effect was sustained over time.
Conclusions A multifaceted intervention can be highly effective for improving discharge communication from the ICU.
- Quality improvement
- decision support systems
- clinical
- hand-off
- medication reconciliation
- critical care
- clinical decision support
- handover
- intensive care
- decision support
- clinical
- decision support
- computerised
- information technology
- evidence-based medicine
- healthcare quality improvement
- patient safety
- diagnostic errors
Statistics from Altmetric.com
- Quality improvement
- decision support systems
- clinical
- hand-off
- medication reconciliation
- critical care
- clinical decision support
- handover
- intensive care
- decision support
- clinical
- decision support
- computerised
- information technology
- evidence-based medicine
- healthcare quality improvement
- patient safety
- diagnostic errors
Introduction
The discharge letter is the primary tool for communication in patient hand-off.1 A recent review showed that discharge letters are rarely written by the first follow-up visit, and only 51–77% are written within 4 weeks.1 Patient hand-off is a high-risk process.2 3 Although poor information continuity has not been linked with patient outcomes,4 poor discharge communication has been associated with readmission,5 and physicians feel that poor discharge communication is a risk to patient safety.6
Clinical decision support, which provides computer-based assistance in clinical tasks,7 has been shown to be an effective strategy for quality improvement.8 However, there is evidence of greater success with multifaceted interventions which incorporate multiple strategies for behavioural change.8 Clinical decision support has been shown to be very effective in other documentation tasks.9 10 Structuring discharge summaries seems to improve recall and acceptability.11 12 In studies comparing use of software to dictation for writing letters, 27–47% more letters are sent if software is used, with a reduction in the mean time to send letters.1 13 However, the time to realise improvement is not yet known, and it is also not known whether the effect is sustained over time.
The objective of this study was to measure the effect of a multifaceted intervention on the time to write an intensive care unit (ICU) discharge letter, the time required to realise the effect, and whether the effect persisted over time.
Methods
Setting
The ICU at the Academic Medical Centre is a 30-bed mixed medical–surgical closed-format ICU, staffed by 10 staff physicians, eight subspecialty fellows and 20 residents. Data on ICU discharges and letters were collected from January 2006 to October 2009.
Quality-improvement intervention
Improvement in medication reconciliation and the timeliness of communication in patient hand-off from the ICU to the wards was made a priority by ICU management. It was decided to use the initial version of the ICU discharge letter as the transfer summary for the wards. This also encouraged writing discharge letters and thus better communication with the general practitioner, who plays a central role in coordination of care in The Netherlands. Because a Patient Data Management System (PDMS, Metavision, iMDsoft) containing all ICU patient data had been in use since 2002, it was anticipated that software integrated with the PDMS would be an effective solution. A longitudinal before–after intervention was developed by a working group of ICU staff (including one of the authors, E JvL), and agreed upon by all ICU staff physicians. The intervention consisted of changes in policy, responsibility and process.
Figure 1 shows the process of writing a discharge letter. Prior to the intervention, hospital policy stated that discharge letters should be written for all patients, but this was not part of ICU policy, and standard practice was that letters were written only for patients who died. Letters were assigned by the department secretary to a doctor (usually a resident), who dictated the letter to be typed. The typed initial letter was sent to a staff doctor for changes, or to finalise the letter as ready to send. For the remaining patients, nearly all of whom are discharged to the wards, a copy of the last day's record and nursing notes were printed and sent with the patient to the wards.

Basic process of preparing a discharge letter. Since the start of the intervention, a copy of the completed initial letter goes with the patient at the time of intensive care unit discharge.
The components of the intervention are detailed in the subsections below.
Policy change
All ICU patients should have letters, and an initial letter goes with the patient to the receiving ward at discharge.
Responsibility
The new software, called ICU-Letters or ‘I-Let,’ assigns responsibility automatically. ICU doctors can see a list of patients needing letters and the doctor who is responsible, and can actively take responsibility for a letter.
Process
Letters can be written in I-Let, with a template to support content decisions. The template includes the date and reason for admission, history, problem list, allergies, labs and medications copied automatically from the PDMS. (A translation of the template is provided in the web-only appendix.) Dictation was still available for doctors who preferred it. If a patient does not have a completed initial letter at the time of discharge, I-Let provides support in the form of an email reminder to the responsible doctor. Staff doctors are responsible for finalising letters and receive a weekly email with a list of letters needing their attention.
The directive for improvement was announced in February of 2006. As the directive was ‘top down,’ consensus was reached by developing the plan at a round-table discussion. Every clinician agreed to comply with the new work plan, and members of the ICU staff were assigned to design the software, including the letter templates. The software was developed and tested in October–December 2006, and the intervention began without incident on 1 January 2007.
Analytical methods
The ICU discharge letter had two important recipients: the ward doctor (receiving the initial letter) and the general practitioner (receiving the finalised letter). We measured the percentage of patients with a completed initial letter ready at the time of discharge, the median time to the first completed initial letter and the median time to finalise a letter. To assess whether improvement could be attributed simply to policy change, deceased patients were analysed as a subgroup.
Since some interventions have a learning curve,14 we also assessed the longitudinal effect using statistical process control (SPC) charts. SPC charts plot a summary statistic over time (eg, the mean time to write a letter) and use the observed variability to calculate the limits of expected variation. A single point outside the limits is statistically significant, but a group of points which are within the limits but trending towards a different mean are also detected. Significant changes indicate that the process is ‘out of control,’ otherwise it is ‘stable.’ A successful intervention causes the process to go ‘out of control’ in the direction of improvement, and a new mean and limits are then calculated.15
For dictated letters, the PDMS patient list was linked with the hospital letters database by matching on the patient number and the ICU discharge date ±1 day. No limit was placed on the time frame after discharge; any letter registered in the database was eligible. Initial letters were registered only when they were formally completed and sent to a staff doctor for approval. Incomplete letters were not measured in our study. If the initial letter was registered before discharge, the elapsed time was recorded as zero.
Analysis was performed in R 2.11.1 (The R Foundation for Statistical Computing), using the package qcc.
Results
Table 1 describes the study population. The percentage of patients with an initial letter formally completed at the time of discharge increased from 2.5% in the 12 months before the intervention to 80% in the 34 months after. By the third month after the intervention, 89.9% of patients had a letter ready at the time of discharge. As shown in the SPC chart (figure 2), this improvement was sustained. The doctors showed a strong preference for using the new I-Let software over dictation: only 45/4811 letters were dictated after the introduction of I-Let.
Demographics of patients admitted to the intensive care unit during the observation period (IQR in parentheses)
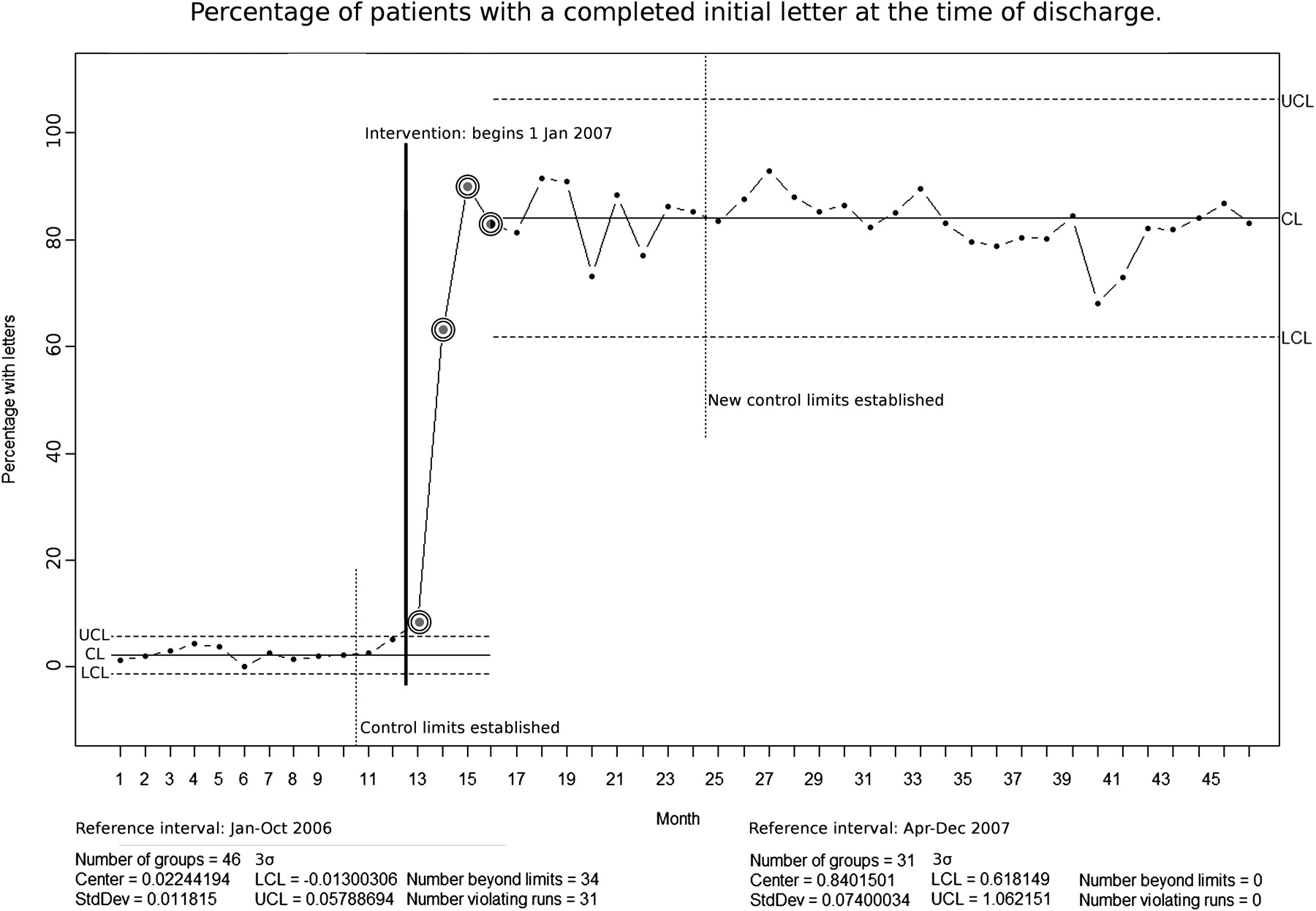
Statistical process control chart of the percentage of patients with a completed initial letter at the time of discharge, per month. The initial letter was used as the transfer note for patients discharged from the intensive care unit to the wards. The intervention resulted in an immediate improvement, and by the third month after the intervention a new pattern was established where 80–90% of patients had a letter ready at the time of transfer. CL: control limit; LCL: lower control limit; UCL: upper control limit.
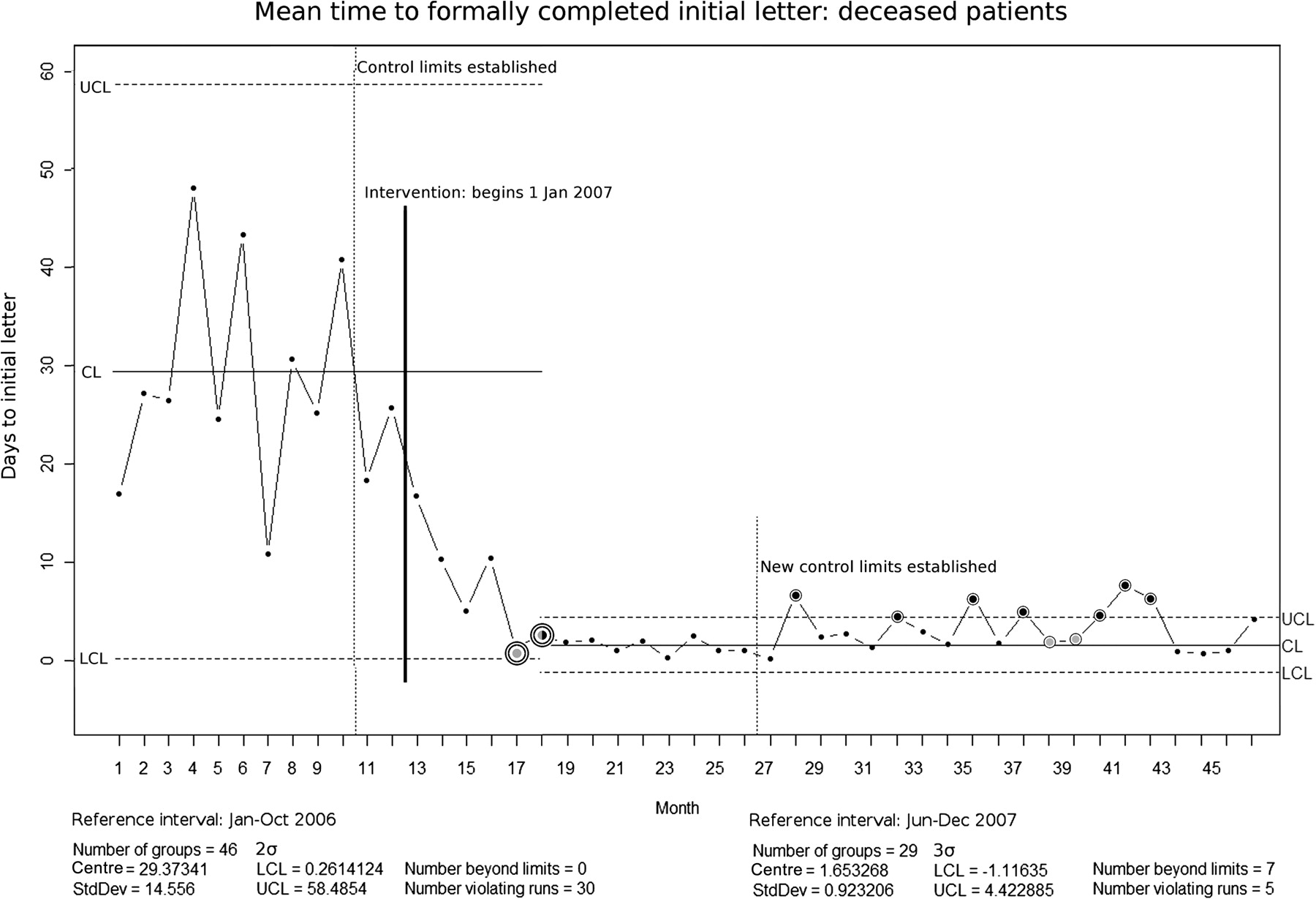
A similar improvement was seen in the mean time to complete the initial letter (figure 3A). The letters were ‘out of control’ by the second month of the intervention, and the new stable pattern began by the third month. The process was stable throughout the remainder of the observation period. The percentage of patients with a finalised letter improved from 11.4% before the intervention to 96.6% after. The median time to finalise a letter was 23 days before the intervention (IQR 9–41) and 4 days after (IQR 2–9, p<0.0001). This improvement was equally rapid but slightly less stable (figure 3B); the control chart reveals a trend towards an increasing mean in the last year of observation. Letters for deceased patients also improved; 71.6% had a completed initial letter before the intervention and 99.7% after, and the time to write the initial letter improved from a median of 15.8 days to 4.7 days, though the effect was smaller and not as stable (figure 4).
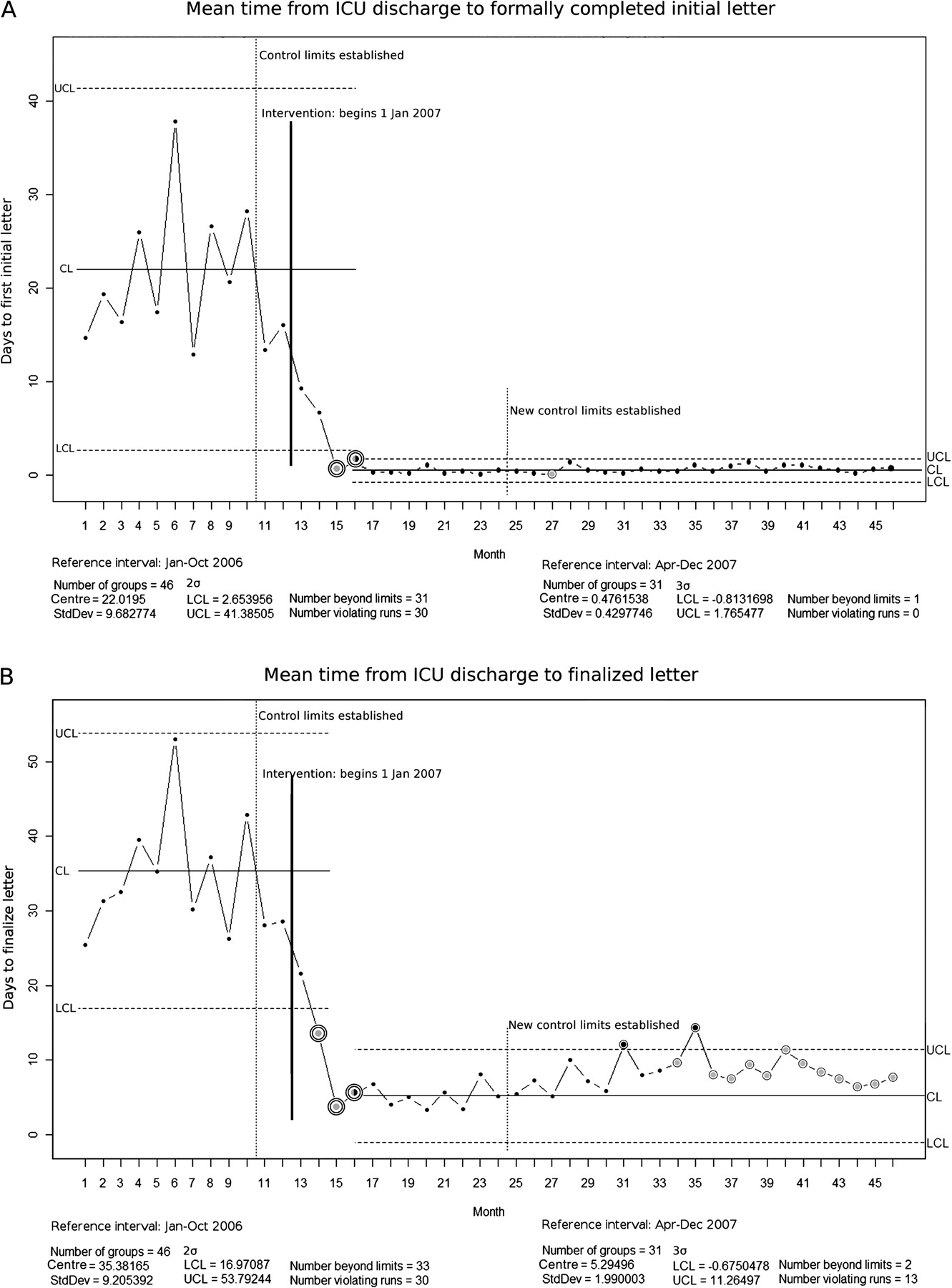
(A) Statistical process control chart of the mean time elapsed between discharge and the completed initial letter. The process was ‘out of control,’ meaning that the intervention had established a statistically significant effect, by the third month after the intervention (month 15). New control limits were established and show that the time to the initial letter has remained stable since the third month of the intervention. (B) Statistical process control chart of the mean time elapsed between discharge and the finalised intensive care unit discharge letter. The results are similar, except the process is less stable than the time to the initial letter. The last 13 months post‐intervention show a trend towards increasing time to finalise letters. CL: control limit; LCL: lower control limit; UCL: upper control limit.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Statistical process control chart of the time elapsed between discharge and the completed initial letter for patients who died. Before the intervention, intensive care unit policy stated that letters were required for patients who died. After the intervention, letters were required for all patients. Analysis of letters for deceased patients shows that the intervention was also effective for this group and demonstrates that factors other than policy change in this multifaceted intervention also had an effect. The effect was not as stable as for the general population but still clearly significant. CL: control limit; LCL: lower control limit; UCL: upper control limit.
Discussion
The principal finding of this study is that a multifaceted intervention can dramatically improve the timely writing of discharge letters. SPC charts help to visualise the rapid effect of the intervention and show that its impact is sustained over time.
The main strength of this study lies in the large number of patients, the profound and sustained effect of the intervention, and the use of SPC to track performance over time. Other than the inherent limitations of a single-centre, before–after study, the main limitation is that the intervention was multifaceted, limiting our ability to determine which components were most important. The other limitation is that we did not measure letter quality (eg, whether the letters contained correct information) or the subjective satisfaction of the users or recipients. However, satisfaction with the system was discussed informally at monthly ICU staff meetings, and it is expected that both letter quality and the quality of overall transfer communication improved with the use of I-Let's content support to encourage completeness and reduce the number of copying errors.
The use of SPC allowed detection of a recent increase in the length of time to finalise letters. This may be related to the increase in the number of medical cases and the severity of illness (see table 1), leading to more complex letters which require more input from the staff doctors. Increased awareness may explain the slightly better performance in December 2006 than in the other preintervention months, although educational effect alone usually is modest and wanes in a short time.1
We considered that the observed improvement was due simply to the new policy of requiring letters for surviving patients. However, a significant improvement was also seen in letters for deceased patients (figure 4), even though these letters are arguably less urgent than letters for living patients. We also observed that after the intervention, 30% more letters were written by day 3 in I-Let versus dictated letters, which is comparable with other studies which did not have a concurrent change in policy.1 13
The initiative was announced in February 2006, and the plan was finalised in October. During this time, several barriers and concerns arose. It was not certain if a PDMS add-on could be written which would fit the workflow of residents, staff and secretarial personnel. This concern was eased by directly involving ICU staff in software design and development, and allotting time for volunteer users to test the system before implementation.
The culture in our ICU is one of proactive quality improvement, and this enthusiasm for innovation facilitated development and acceptance of the new system. Another supporting factor is that new residents enter our team every 6 months, and for them the new system is ‘just the way we do things.’ Increased standardisation of the process and content may also contribute to success.16
We anticipate that similar results are possible for hospital discharge letters. Hospitals without a complete electronic patient record cannot offer automatic copying of this information into the discharge letter, an important feature of I-Let. However, the doctors feel that email reminders and the positive peer pressure of having the list of ‘letters due’ visible to their colleagues are highly effective, and these support features could be provided without a full electronic patient record.
No studies to date have reported on the use of email reminders as decision support to improve the time to send letters, but other reminders to perform documentation tasks have reported good results, including a 50% improvement in completion of evaluation forms and 13% improvement in completing anaesthesia documentation.9 10 Email reminders are a logical form of support for tasks such as documentation which are important, but not urgent. A randomised controlled trial testing this simple component of the intervention alone would help to quantify its effect.
In conclusion, a multifaceted intervention can be very effective for improving the percentage of discharge letters which are written and the time to write them. The intervention consisted of policy change and implementation of software with decision-support features such as automatic copying of relevant information from the patient record, transparency to peers and electronic reminders to complete letters. This intervention resulted in a rapid improvement which was sustained over the 2-year observation period.
Acknowledgments
The authors would like to acknowledge the management, doctors and support staff of the ICU for their involvement in the planning and implementation of this intervention.
References
Footnotes
Funding This study was funded in part by The Netherlands Organization for Health Research and Development (ZonMw), through the ICOVE project (#311020302).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.