Article Text

Abstract
Background The impact of a pandemic on unplanned hospital attendance has not been extensively examined. The aim of this study is to report the nationwide consequences of the COVID-19 pandemic on unplanned hospital attendances in Denmark for 7 weeks after a ‘shelter at home’ order was issued.
Methods We merged data from national registries (Civil Registration System and Patient Registry) to conduct a study of unplanned (excluding outpatient visits and elective surgery) hospital-based healthcare and mortality of all Danes. Using data for 7 weeks after the ‘shelter at home’ order, the incidence rate of unplanned hospital attendances per week in 2020 was compared with corresponding weeks in 2017–2019. The main outcome was hospital attendances per week as incidence rate ratios. Secondary outcomes were general population mortality and risk of death in-hospital, reported as weekly mortality rate ratios (MRRs).
Results From 2 438 286 attendances in the study period, overall unplanned attendances decreased by up to 21%; attendances excluding COVID-19 were reduced by 31%; non-psychiatric by 31% and psychiatric by 30%. Out of the five most common diagnoses expected to remain stable, only schizophrenia and myocardial infarction remained stable, while chronic obstructive pulmonary disease exacerbation, hip fracture and urinary tract infection fell significantly. The nationwide general population MRR rose in six of the recorded weeks, while MRR excluding patients who were COVID-19 positive only increased in two.
Conclusion The COVID-19 pandemic and a governmental national ‘shelter at home’ order was associated with a marked reduction in unplanned hospital attendances with an increase in MRR for the general population in two of 7 weeks, despite exclusion of patients with COVID-19. The findings should be taken into consideration when planning for public information campaigns.
- emergency department
- healthcare quality improvement
- health services research
- mortality (standardized mortality ratios)
Data availability statement
Data may be obtained from a third party and are not publicly available. According to Danish law, data cannot be shared. However, the data sources are available for other researchers pending approval from the Danish Health Data Authority.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
- emergency department
- healthcare quality improvement
- health services research
- mortality (standardized mortality ratios)
Introduction
At the end of 2020, more than 83 million people have been confirmed to have COVID-19 infection and 1.8 million have died worldwide.1 To reduce the transmission and mortality from COVID-19—that is, ‘flatten the curve’—many countries, including Denmark (online supplemental figure 1), have issued ‘shelter at home’ orders involving the whole nation temporarily shutting down daycare, schools, industries and most public gatherings.2 Such actions have not been taken before in modern times and the downstream effects are therefore unknown.
Supplemental material
The effects of such drastic measures are confined to patients with suspected or confirmed COVID-19 infection and these actions affect the entire population. ‘Shut-down’ measures and the intense focus on a single disease could increase public concerns about the risk of contamination by infected persons.3–5 This may cause the general public to believe that the concentration of infected persons is higher in healthcare settings than in society as a whole, and that the capacity of the healthcare system is not sufficient to handle patients without COVID-19. Consequently, people may avoid hospitals or delay seeking medical care with possible detrimental effects. Indeed, there have been reports of reduction in hospital and general practitioner (GP) visits during the COVID-19 pandemic from several countries.6 7 Several countries have reported increases in overall mortality during the pandemic,8 while some, including Denmark, until now have shown little change or a reduction of the mortality rate.9
To date, no scientific study has documented unplanned hospital attendances of an entire population during a pandemic. We report the nationwide consequences of the COVID-19 pandemic on unplanned hospital attendance patterns and population mortality of Denmark for the first 7 weeks after the national ‘shelter at home’ order (11 March 2020) was issued. Specifically, this study compares the incidence rate of unplanned non-psychiatric and psychiatric hospital attendances on a weekly basis before and during the ‘shelter at home’ period between 2017–2019 and 2020; it shows these patterns for the most common discharge diagnoses of diseases expected to remain stable during the pandemic; and it describes the risk of death-in-hospital and the general population mortality during these periods.
Methods
We conducted a nationwide observational study of hospital-based healthcare seeking and mortality of all people living in Denmark, excluding Greenland. We used the Danish nationwide registers (the Danish Civil Registration System and the Danish National Patient Registry (DNPR), see below) to identify all unplanned hospital attendances and calculated the incidence rate per week in 2020 (9 March–26 April), comparing it to corresponding weeks in 2017–2019.
Setting
Denmark is a high-income country with high population density (137 per km2) and approximately 5.8 million citizens. The Danish healthcare system is publicly funded by taxation and is free at the point of care to all residents with universal coverage, except for some copayments for prescription drugs and dentistry. GPs act as gatekeepers to secondary healthcare and almost all residents are assigned a GP.10 Emergency department (ED) attendance requires a medical referral or activation of the emergency medical services. Psychiatric hospitals have separate EDs and some are open for walk-in patients.11
Participants
We included all people registered as living in Denmark between 1 January 2017 and 26 April 2020.
Data sources
Data on age, sex and mortality were extracted from the Danish Civil Registration System (DCRS).12 Information on hospital attendance (date of arrival and discharge), diagnoses and procedures were extracted from the DNPR,13 including non-psychiatric and psychiatric attendance. Both registries are considered to have high data quality and low frequency of missing data,12 but DNPR was delivered in a temporary form, made available by the government expressly due to the COVID-19 pandemic for research. Follow-up ended on 26 April 2020. Unplanned hospital attendances were identified using the allocated variables (c_pattype=1 or 3, c_indm=1 and prioritet=ATA1) describing the indication of the priority of the patient and the patient’s administrative relationship with the hospital.
DNPR is based on individual hospital attendances, and any transfer between departments was coded in the database as individual attendances. For the purpose of assessing attendance as an entire admission rather than individual attendances, we combined instances of multiple attendances within 4 hours into one attendance.14 Only unplanned hospital attendances were included. We did not include elective surgery and outpatient clinic attendances.
The number of inhabitants in Denmark was retrieved from Statistics Denmark that collects, compiles and publishes statistics on the Danish society (https://www.dst.dk/).
Outcomes
The primary outcome was the incidence rate ratio (IRR) of unplanned hospital attendances per week, calculated by comparing unplanned incidence rates during ‘shelter at home’ with corresponding periods from the prior 3 years.
Secondary outcomes were mortality rate of the general population and risk of death-in-hospital on a weekly basis.
Mortality rate for the general population was calculated for the entire population based on DCRS data, while risk of death-in-hospital was calculated for any person who died during admission or on the day of discharge based on DCRS (for date of death) and DNPR (for whether the person was admitted at that time or not) data. The yearly increase in the Danish population was taken into account by using the mean population number per period.
Variables
Age was grouped into four categories: 0–17, 18–49, 50–69 and 70+ years.
Comorbidity was presented using the Charlson Comorbidity Index (CCI).15 CCI was calculated by us based on hospital diagnoses in the 10 years before the hospital attendance. CCI was coded three levels: low (score 0), moderate (score 1–2) and high (score ≥3).
In addition, we predefined 29 diagnoses (online supplemental table 1) for which the incidence rate was expected to remain unaffected by the ‘shelter at home’ orders. We plotted these on a weekly basis for the years 2017–2019 (data not presented) and selected the five most common discharge diagnoses that remained stable across 2017–2019 to examine changes in 2020.
Ethics
Under Danish law, observational studies do not require ethical approval.16 Data are presented in accordance with the STROBE guidelines.17
Data availability
According to Danish law, data cannot be shared. However, the data sources are available for other researchers pending approval from the Danish Health Data Authority.
Statistics
Data are presented in absolute numbers of attendances (per cent) and differences between groups assessed with the Pearson’s χ² test. To account for any holidays that might have implications for week-to-week variance, we calculated the weekly mean number of the unplanned hospital attendances for the control years (2017–2019). To analyse the changes in death-in-hospital and mortality rate after ‘shelter at home’ was ordered, we calculated the IRR and mortality rate ratio (MRR) using Poisson regression. The impact model calculated the weekly IRR and MRR during the home shelter period (9 March–26 April 2020) with all other weeks as a reference. We adjusted for the year-by-year increase in unplanned hospital attendances and the weekly variance. We did not adjust for patient-level characteristics to describe the actual changes in the unplanned hospital attendances. However, analyses were stratified according to age, sex, psychiatric/non-psychiatric and the five most common discharge diagnoses expected to remain unaffected during the pandemic. Analyses were done on attendance level. All analyses were carried out with Stata V.15 (Stata, College Station, Texas, USA).
Results
A total of 2 438 286 unplanned hospital attendances were registered, 247 567 of these happened during the ‘shelter at home’ period and 763 538 in corresponding weeks in the previous 3 years (table 1). The case-mix in the ‘shelter at home period’ differed compared with the previous years’ corresponding weeks. More were women, older and more likely to have a medium score in CCI after the ‘shelter at home’ order.
Characteristics of patients from the control years in 2017–2019, the prior period in 2020 (30 December 2019–8 March 2020) and during the ’shelter at home' (9 March–26 April) order was issued on 11 March 2020
Immediately after the ‘shelter at home’ order was issued, there was a clear drop in unplanned hospital attendances (figure 1A). Within 3 weeks, however, the number of attendances rapidly increased to near normal numbers, but this was due to suspected or confirmed COVID-19 cases (figure 1A–D). The drop in non-COVID-19 attendances were seen for both non-psychiatric and psychiatric diagnoses (figure 1C and D). The mean number of unplanned hospital attendance in 2020 was 646 (SD 12.3) before and 607 (SD 61) after the ‘shelter at home’ order. In the corresponding periods in 2017–2019, the mean number of unplanned hospital attendances were 606 (SD 16.6) and 628.6 (SD 9), respectively. In relative numbers, expressed as IRRs, unplanned visits decreased significantly after the ‘shelter at home’ order (table 2), both overall (16–22 March, IRR 0.79, 95% CI 0.77 to 0.80), excluding COVID-19 related attendances (16–22 March IRR 0.69, 95% CI 0.68 to 0.71), for non-psychiatric attendances (16–29 March IRR 0.69, 95% CI 0.68 to 0.71) and psychiatric attendances (6–12 April IRR 0.70, 95% CI 0.65 to 0.75).

Number of unplanned hospital visits per 100 000 population per week. Solid lines indicate weeks in 2020, dashed lines mean number of visits per week in 2017–2019. (A) Number of unplanned hospital visits overall. (B) Number of unplanned hospital visits excluding COVID-19-related visits. (C) Number of unplanned non-psychiatric hospital visits excluding COVID-19-related visits. (D) Number of unplanned psychiatric hospital visits excluding COVID-19 related visits.
IRR for unplanned hospital visits in the period following the ‘shelter at home’ order in Denmark
Children’s (<18 years old) unplanned attendances were the age group most affected with a 41% reduction from 30 March to 5 April (IRR 0.59, 95% CI 0.57 to 0.61). However, this drop for children was not as pronounced for unplanned psychiatric attendances with reduced use in a single week (6–12 April) immediately followed by an increased use the following week.
Of the five diagnoses expected to remain stable, chronic obstructive pulmonary disease (COPD) exacerbation was the most affected with an unexpected decline in all weeks. Also, hip fracture and urinary tract infections had unexpected drops in unplanned attendances with a 32% (IRR 0.68, 95% CI 0.53 to 0.88) and 54% (IRR 0.46, 95% CI 0.47 to 0.67) drop 23–29 April, respectively.
There was an immediate increase in the number of hospital attendances (figure 1A–D) after the Danish National Board of Health issued a statement reminding the public to seek help if needed on 13 April.
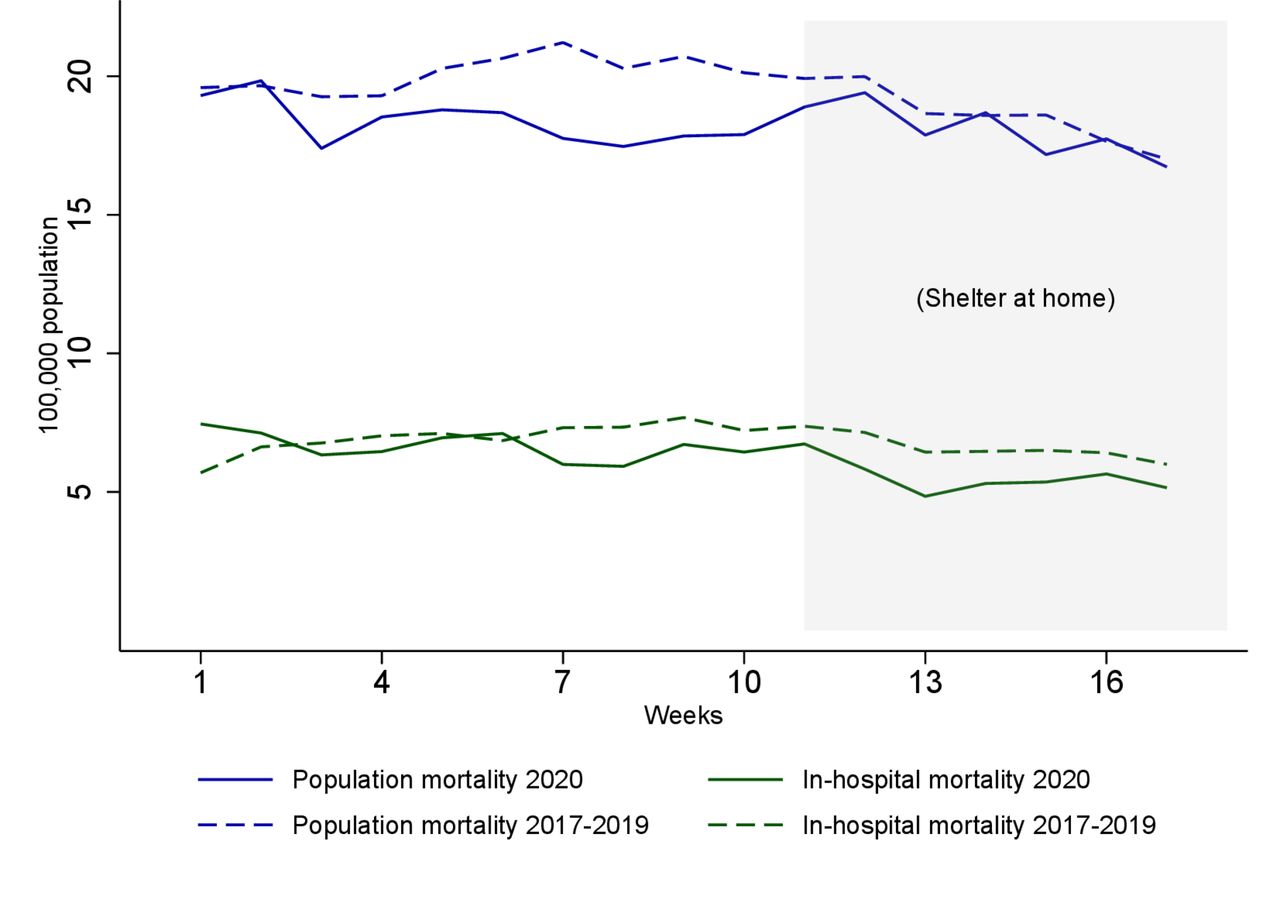
The overall crude mortality rate in the general population decreased in the observed weeks of 2020 (figure 2). However, in relative terms (adjusting for years, individual weeks and weeks after issuing the ‘shelter at home’ order), we observed increased MRR after the ‘shelter at home’ order in the general population for all weeks except week 11 (table 3). When excluding suspected or confirmed COVID-19 infections, the increase in general population MRR was only significantly increased for 2 weeks, from 30 March to 5 April (MRR 1.10, 95% CI 1.01 to 1.20) and 13–19 April (MRR 1.10, 95% CI 1.01 to 1.21) (table 3).
MRR for unplanned hospital attendances in the weeks following the ‘shelter at home’ order in Denmark

{kind=link}
{kind=link}
Crude death rate (population and in-hospital) per 100 000 population per week in 2020. Solid lines indicate weeks in 2020 and dashed lines mean number of visits per week in 2017–2019.
The crude risk of death-in-hospital per week decreased in both 2020 and 2017–2019 (figure 2). The mean number of death-in-hospital in 2020 was 6.7 (SD 0.5) before and 6.2 (SD 0.4) per 100 000 after the ‘shelter at home’. In the corresponding periods in 2017–2019 were mean number 7 (SD 0.5) and 6.6 (SD 0.5). Adjusting the risk of death-in-hospital as MRR only showed a significantly reduced risk in the 2 weeks from 16 to 29 March (MRR 0.85, 95% CI 0.73 to 0.99, MRR 0.79, 95% CI 0.67 to 0.93, respectively) and only when excluding patients not hospitalised with suspected or confirmed COVID-19 infection. The reduction in the risk of death-in-hospital was mostly accounted for by the elderly (table 3).
Out of the 29 prespecified diagnoses expected to remain stable during a pandemic (online supplemental table 1), the five most common were schizophrenia, COPD exacerbation, hip fracture, myocardial infarction and urinary tract infection. Of these, schizophrenia and myocardial infarction were unchanged, while the other three decreased over the 7 weeks (online supplemental figure 2 and table 2). The MRR could not be calculated for schizophrenia and urinary tract infection due to too few events and was unchanged for the other three (table 3).
Discussion
In this nationwide observational study, we describe a marked decrease in the incidence of unplanned hospital attendances, both for non-psychiatric and psychiatric patients, after a government-issued shelter at home order. We found a decrease of up to 31% for non-psychiatric patients and up to 30% for psychiatric patients after excluding visits due to suspected or confirmed COVID-19 infection. Crude mortality rates for the general Danish population decreased after the shelter at home order was issued, whereas the adjusted mortality rate was moderately increased in some but not all weeks. Death-in-hospital also decreased after issuing the shelter at home order in crude analysis but adjusting for expected mortality rates as MRRs we found the decrease to only be significant if excluding patients with confirmed or suspected COVID-19 infection.
Our observed reduction in patients with non-COVID-19 related disease is similar to what has been reported elsewhere.14–16 However, the general population’s overall mortality rate appears to be less marked than in many other countries.1
When designing the study, our initial concern was, that patients would opt out of seeking healthcare during the pandemic due to the risk of nosocomial infection and a wish not to burden an already overstretched system. While choosing to opt out of healthcare perhaps can be of little consequence for some, other patients could put themselves in danger by doing so. In order to plan for future pandemics, decision-makers in healthcare must have an indication of the behaviour of the public. Who will, and who will not, attend hospitals and primary care and why? Our findings show that, fortunately, mortality rates did not increase substantially despite a general decline in hospital attendance. Thus, perhaps, we should not be worried about patients with relevant complaints not seeking care during a full-scale pandemic in a country with free universal healthcare.
During this pandemic, other studies have also reported a reduction in hospital attendances by patients not suffering from COVID-19,18 but with a significant concomitant increase in mortality.7 17 Using the unique Danish registries, we have been able to examine the effects of the COVID-19 pandemic for an entire nation and all unplanned hospital attendances. We show a marked decrease in unplanned hospital attendances after the ‘shelter at home' order was issued and demonstrate an 11%–20% increase in the general population’s MRR in 6 of 7 weeks. Excluding patients admitted with suspected or confirmed COVID-19, the excess mortality rate was lowered to 10% and only present in 2 out of 7 weeks and with CI very close to 1.00.
In contrast to the findings of this study, other countries have reported reductions in patients who had stroke,19 myocardial infarctions20 and primary percutaneous coronary intervention.21 While not all of these entities were part of our analyses, we could not confirm the reduction in myocardial infarction for any of the weeks included. There are likely to be several reasons for this difference. Perhaps most importantly, Denmark was quick to issue a ‘shelter at home’ order; as a result, the healthcare system was never over-run, and vital emergency services were continuously provided. In addition, several widespread public information campaigns have taken place over recent years (even as late as early 2020), reminding the public to remember to seek help in case of symptoms relevant to stroke or myocardial infarction. It is also important to note that Denmark has a universal healthcare system, which decreases the barriers to seeking care. The Danish population has a high degree of health literacy and a general trust in authorities (both healthcare and governmental) and may have a stronger tendency to seek help when needed.22 This is also evident by the rapid increase in hospital visits after the National Board of Health’s reminder. While we expected COPD to remain stable in attendances based on 2017–2019 numbers, we, in fact, saw a marked reduction. We can only speculate to the cause, but suspect that a general reduction in transmittable diseases (including viral pathogens) also controlled by the national lockdown, probably decreased proportionally.18
A situation, where an entire population could choose to opt out of healthcare services, has never been seen before in the Western world.23 In fact, increased healthcare utilisation, both in general and in relation to influenza, was seen in prior influenza epidemics.24 During the recent Ebola epidemic in Africa, one study reported a decrease in hospital use in those most affected by Ebola.25
While we did observe indications of increased general population mortality rates, this did not seem to be directly correlated with the steep decrease in unplanned hospital attendances, especially when excluding suspected or confirmed COVID-19 infections. As we only have data until 26 April 2020, it could be that we simply have not yet seen the full effect of the lower hospital attendance. An alternative explanation may be potential overuse of some healthcare services prior to the pandemic.26 While previous studies reporting on hospital strikes have indicated a reduced in-hospital mortality,27 no solid causal arguments yet have been made on adverse effects of lower hospital attendance. Denmark has a strong tradition for GP service and all Danes have access to a GP around the clock. Therefore, it is also plausible that patients could have contacted their GP (when they would normally seek hospital care), but as we do not have access to data on GP usage, we can only speculate.
Our study has limitations. First, we only have data until 26 April 2020. Therefore, any increase in delayed mortality or hospitalisation will not be apparent in our study and additional follow-up time will be required. Second, while data were extracted from national registries, the patient registry was only delivered in a temporary form, made available by the government expressly due to the COVID-19 pandemic for research. Hence, the data were not validated to the usual level of the Danish databases, and there is a risk of incomplete data.28 However (see online supplemental figure 3), we have no indication of any reduction in data quality. As most data in the national registers are automatically extracted from hospital registries, we expect that data quality should not be affected. Indeed, our thorough data validation did not provide any indication that this should be the case. Third, as we use only primary discharge diagnoses and not supplementary diagnoses, we rely on the treating physicians' coding quality. Given that we have compared 2017–2019 with 2020, there is most likely only a minimal risk of coding practice changing over time. Fourth, we only include data for attendances and one patient might have been included multiple times, even with related readmissions. Fifth, there is the possibility that the ‘shelter at home’ order resulted in a general reduction in communicable diseases which could reduce other admissions. Unfortunately, we are currently unable to study this with the existing dataset. While we only have register data, we do indeed have data on a truly national level and not only for hospital use. Our results as such do represent the general population and not only for residents using the healthcare system. And last, our results might not be generalisable as the Danish healthcare system is unique and the health-literacy of the population is high.
Conclusion
The COVID-19 pandemic and the governmental shelter at home order in Denmark led to a marked reduction in the incidence rate of unplanned hospital attendances with a significant decrease in the absolute number of fatalities in the general population but with a moderate increase in adjusted mortality rate in 4 of 7 weeks in the general population.
Data availability statement
Data may be obtained from a third party and are not publicly available. According to Danish law, data cannot be shared. However, the data sources are available for other researchers pending approval from the Danish Health Data Authority.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Danish Patient Safety Authority (file number 20/18426).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
SBB and MF are joint first authors.
Twitter @BieBogh
Contributors All authors made a substantial contribution to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work. MBr, SBB and MF conceived the study. MBr, SBB, RYH and MF designed the study. SBB and MF processed and analysed the data and all authors were involved in interpretation of the data. RYH and CAG provided an international approach to findings. MBe, SPJ, SBB, DPH, KRO and LCT designed the statistical analysis plan. SKN, SH, MRK, LEL, TL, MBS, HL, RYH, CAG, MBr, MF, PH and HGJ interpreted the findings from the emergency department. LF, EFC, JS, DPH, KEB and SM interpreted the findings from associated fields of medicine. MBr, SBB and MF drafted the paper and all authors revised it critically for important intellectual content. All authors gave the final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. MBr is the guarantor for the paper and accepts full responsibility for the work and/or the conduct of the study, had access to the data and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.