Article Text

Abstract
Upper respiratory tract infection (URTI) in children is one of the most common reasons for general practice (GP) attendance over the winter months. It is crucial to be able to risk stratify and determine the severity of illness in these patients. It is important both to recognise those who are clinically unwell and require treatment escalation, and also to not overprescribe antibiotics due to the ongoing problem of antibiotic overuse and resistance.
This quality improvement project was undertaken to improve the way in which these consultations were held and also the way they were documented. It was recognised that key features in assessing a potentially unwell child were to measure their heart rate (HR) and respiratory rate (RR). As children can often deteriorate rapidly and their clinical course may not necessarily be easy to predict, we wanted to make sure that parents were being provided with safety netting information in the event that the child should become more unwell after the consultation.
Through the course of our project, we managed to improve the proportion of consultations for URTI or ‘viral illness’ in children in which HR and RR were documented from 57% to 100%. The proportion of consultations in which safety netting information for parents was discussed and documented improved from 48% to 96%.
By using quality improvement strategies, we have succeeded in improving both the safety and efficiency in the way children who present with URTI are assessed in GP.
- quality improvement
- general practice
- PDSA
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
In general practice (GP), it is widely acknowledged that there is enormous time pressure and demand on workload, particularly in the context of seasonal illness during the winter months. One of the challenges and rewards of working in GP is the huge range of health and disease it encompasses but diligence and care is required when it comes to assessing patients who present with common complaints such as a viral upper respiratory tract infection (URTI). Although it is not unusual to use consultations perceived as being ‘easy’ or ‘straightforward’ to catch up on a clinic where complex patients with multiple issues are being seen, we recognised that there was a potential for the assessment of these patients and the documentation of the consultation to be compromised as a result of this. An experienced clinician will no doubt be capable of safely assessing a child presenting with an URTI, however when under time pressure, it is easy to miss simple yet important parts of the assessment as well as document minimally in order to save time.
This project was designed to improve the assessment of children presenting with upper respiratory tract symptoms and their documentation by using a simple yet effective template within the Egton Medical Information System (EMIS) used by the practice. The practice is located in the tenth least deprived Index of Multiple Deprivation decile, serving a population of just under 5000 patients. Having recently changed from the Vision (In Practice Systems) system to EMIS, there was an impetus to use the tools available to improve the healthcare services provided. Our SMART (specific, measurable, achievable, realistic and timely) aim was to measure and record heart rate (HR) and respiratory rate (RR) in 95% of children who present with URTI symptoms and provide safety netting information to 95% of those patients and/or their parents over a course of 3 months.
Background
Respiratory tract infection is one of the most common presentations of children to primary care. Although the majority of cases are due to viral illness, there is a wide spectrum of disease which can be risk stratified using appropriate clinical assessment. Antibiotic prescription in primary care for coughs and cold has increased by 40% between 1999 and 20111 and it has been demonstrated that this leads to increased antimicrobial resistance in individual patients.2 This has implications on a population level as well as affecting individual clinical outcomes, including increased time to symptom resolution, increased repeat consultation and increased prescription of further antibiotic courses.3 Furthermore, a recent survey by market researcher, Ipsos MORI, revealed that although half of patients who attend their local GP with respiratory tract infection expected antibiotics, many patients expected advice due to the severity of their symptoms and lack of improvement.4 They showed that 88% of the population surveyed trusted their GP to determine whether or not antibiotics were needed. This suggests that there is scope for strategically reducing unnecessary antibiotic prescriptions in GP, reducing the risk of further antibiotic resistance in the population.
There has been research supporting certain characteristics as being independently predictive of hospital admission and thereby severity of illness,5 as well as established tools such as the Centor criteria.6
The assessment of an unwell child will centre on a few key observations which allow us to objectively measure the severity of illness. There is undoubtedly significant overlap between these observations and the clinical signs that are indicative of sepsis. One of the first signs of an acute illness and respiratory distress is a rise in RR.7 This is closely followed by HR, a rise which can indicate both an increase in cardiac output due to the increase in energy demands of respiratory distress as well as intravascular depletion secondary to poor oral intake and the sepsis response. With changes in physiology, the normal value ranges for HR and RR in children change as they get older.8 However in a short consultation, there is not always time to look up these values, so we decided to include these values on the template itself to act as a quick reference for the user.
Safety netting is an important part of clinical practice.9–11 As with any assessment of illness, the assessment done has temporal constraints in that one can only assess and document how the child presents at that point in time. Although there are markers that can be indicative of severity, it is not possible to predict the outcome in every child who presents to their GP. As a result, it is important to provide parents with information that will help them to know if their child has become more unwell and what they can do in those situations. Through educating patients and/or their parents on adverse developments to look out for, we can help to safeguard these patients, particularly younger children, who may not themselves be able to recognise or communicate the severity of their illness. It is also a communication tool that we can use to reassure parents that at the time of consultation, the child does not warrant any escalation in medical treatment and empower them to have the confidence in looking after their child at home with clear instructions on features to look out for that may indicate deterioration.
From the medicolegal perspective, well-maintained medical records are paramount to optimising clinical care. Keeping good quality medical records contributes to effective risk management. It builds a clear picture of the consultation which may need to be referred to retrospectively, for instance to assess for any change or development in clinical status, and helps to identify an emerging clinical diagnosis or disease trajectory. This is particularly important if there is a number of healthcare practitioners who are involved with the patient over a period of time as it ensures good communication between teams and allows for improved continuity of care. Well-maintained medical records, where a thorough history and examination are clearly documented, as well as relevant follow-up or safety netting information is recorded, demonstrate good clinical practice. It reflects well on the clinician in difficult cases where the patient may encounter an unfavourable outcome or be dissatisfied with their treatment. Therefore good record keeping is just as important as the clinical assessment of children who present to GP with URTIs.
Measurement
An initial baseline measurement of the number of children who were coded as having an URTI or ‘viral illness’ in the month prior to starting the quality improvement project was performed. The EMIS population reporting tool was used to generate a list of patients where ‘URTI’ or ‘viral illness’ were coded in the ‘Problem’ section of the consultation. These consultations were retrospectively analysed to identify the proportion of encounters in which HR or RR and safety netting discussion were documented. We decided to choose these characteristics as they form the basis of a safe consultation where severity of illness has been objectively assessed and safety netting information has been appropriately given. Both numerical values for pulse rate and RR as well as qualitative descriptors such as ‘pulse rate normal’ were accepted as an indication of assessment.
The results of our baseline measurement showed that in the month preceding this project, 21 patients were coded as having an URTI or ‘viral illness’. Of those patients, 57% had HR or RR documented and 48% had documentation of the safety netting discussion.
To assess whether we had achieved our aim of measuring and recording HR and RR and providing safety netting information in 95% of children who present with URTI symptoms, we used this same methodology to study the efficacy of each intervention.
Design
The idea for this project was initially conceived after discussion about how best to use the EMIS template function to improve consultations. Particularly during the winter months, URTIs in children are very frequently seen and so we decided that we could make a substantial positive impact on delivery of care by targeting these types of consultations. We reviewed the literature on this topic area and collated the pertinent features that contribute to diagnosis and prognostication. Based on this, we created a draft template.
The initial draft template was trialled by the two authors. Based on their experiences, adjustments were made to the formatting. Extra components were added to make the template more comprehensive and certain fields were made mandatory.
The main stakeholders of the project were the GP partners and the GP trainees with whom this template was first piloted. They were very amenable to trialling this template and were keen to make full use of the facilities of the new system. They were shown both how to access the template and also use it during the consultation, emphasising that all mandatory fields must be entered before the template can be saved.
As this project took place in a relatively small practice, we were able to receive regular feedback on the use of this template and could adjust the template to their needs, as well as address any issues with using or saving the template. This tool was therefore tailored for the purposes of the stakeholders of this project.
Strategy
Our SMART aim was to improve consultations for children who presented with symptoms of a viral illness or URTI by measuring and recording HR and RR in 95% of patients and provide safety netting information to 95% of those patients and/or their parents over a course of 3 months. We undertook three Plan Do Study Act (PDSA) cycles.
PDSA 1
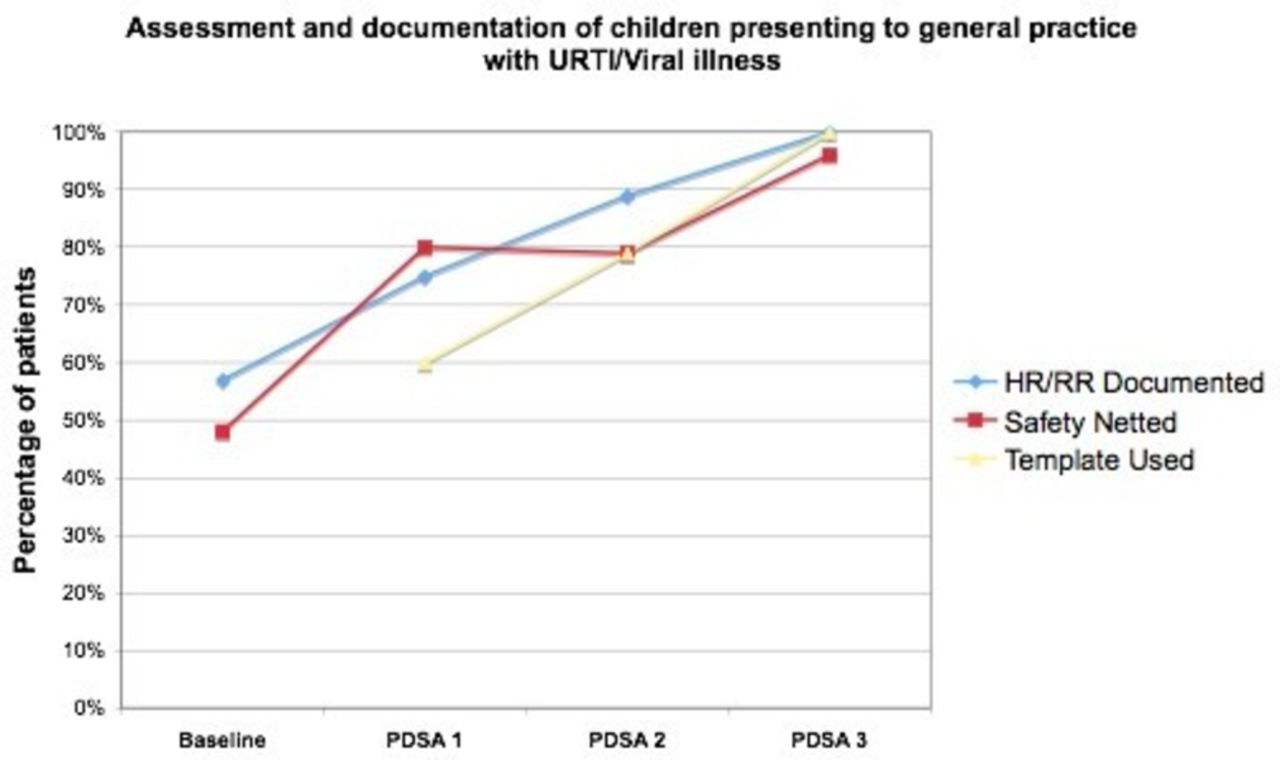
After creation of the initial template, we introduced it to all the doctors in the practice and explained how to implement it during their consultations. Although there was some promising early uptake of the template (60% of all consultations in children coded with URTI or ‘viral illness’), leading to an increase in documentation to 75% and 80% for HR/RR and safety netting documentation, respectively, there were some factors limiting its use. First, not all users remembered that there was a template and so the consultation was documented using free text. Second, in some consultations where the template was used, there were incomplete mandatory fields which prevented the consultation from being saved and so those users reverted to free-text documentation. Third, although many of the fields in this template were relevant to the assessment of the patient, restricting this to being coded as an URTI was not always appropriate.
PDSA 2
There were many learning points from the first PDSA cycle. The biggest factor identified was that there was a number of consultations in which the template had been forgotten to be used. In only 79% of consultations in children coded as URTI or ‘viral illness’ was the template used. We therefore decided to create a protocol using the EMIS system where after coding for a ‘viral illness’, ‘URTI’ or any similar description, the user would be prompted to use the URTI template. This improved template uptake and as a result, documentation of HR/RR improved to 89% while the documentation of safety netting discussion was maintained at 79%.
PDSA 3
After the second intervention, we noted that users were all more familiar with using the template. However, we realised that it was very restrictive to use this for only ‘viral illness’ and ‘URTI’. Our third intervention was therefore to open up the criteria for using this template to any child presenting with symptoms of a viral infection who would warrant a sick child assessment. We did this by changing the automatic coding of URTI to a drop-down menu of common problems such as ‘viral tonsillitis’ and ‘otitis media’. Users were notified of this change and were in agreement that this template would be a useful tool to facilitate more efficient documentation of these consultations. Template uptake reached 100% of children’s consultations coded as URTI or ‘viral illness’ and as a result, documentation of HR/RR improved furthermore to 100% and safety netting to 96%. The feedback we received showed that by making the template more flexible, there was higher uptake of template use both as a prompt for clinical assessment and as a tool for improving the standard of record keeping. We found, as an added benefit, that the template also acted as a reminder to give safety netting advice to the patient and record the discussion.
Results
Our results demonstrate that with each intervention, there was both increased uptake of template utilisation reflecting an improvement in the percentage of consultations in which HR and RR as well as safety netting information was documented. By the end of the third PDSA cycle, we had successfully reached our target of achieving at least 95% compliance with documentation (see figure 1). All consultations that involved URTIs or ‘viral illness’ had been documented using the template. Verbal feedback from the stakeholders was good and the template was found to be easy and straightforward to use; the general consensus was that it helped to manage the consultation time more effectively, spending more time with patients while still ensuring good and safe documentation. Compared with the initial baseline measurements of 57% and 48% documenting HR/RR and safety netting, respectively, this was almost a 100% improvement.
{kind=link}
Chart demonstrating percentage of patients in whom HR/RR and safety netting were documented and the template was used. HR, heart rate; PDSA, PLan Do Study Act; RR, respiratory rate; URTI, upper respiratory tract infection.
By using EMIS and an online report generation tool, data collection was accurate and readily amenable to audit. However in terms of completeness, there is evidently an unmeasurable number of consultations where a child with an URTI or viral illness was seen but not coded specifically. These consultations would not have been reported by the EMIS search tool. Despite this, the number of patients in each search report stayed approximately the same through each PDSA cycle and by measuring the proportion rather than absolute number or consultations, this factor is unlikely to have had a significant impact on the overall results.
One of the unexpected benefits of going through this project was that although this template was specifically designed for use in children, it was also found to be quite useful for documentation of adult consultations of a similar nature. Although it required some adjustment, the template translated relatively well and in some adult cases, was also used to document their URTI or ‘viral illness’. Overall this project was cost neutral.
Lessons and limitations
The completion of this project demonstrated to us clearly the potential of using templates to facilitate improved consultations. Informal feedback showed that the template made consultations more time-efficient and clinically orientated. Although designing the template itself was relatively straightforward, the real challenge was tailoring it for the users within the practice and optimising its access and ability to meet the demands of a busy clinic. Regular engagement with all users of the template meant that we could address their needs and develop a clinically useful tool.
One particular strength of this project is that it establishes a way of improving consultations which can then be translated to other problems. For example, for the examination of skin lesions, a template can be used to ensure that a thorough ABCD (Appearance, Border, Colour and Diameter) system is used and following this, guidance that we give patients on changes to look out for and sun protection advice is documented.
Another strength of this project is the way it can be exponentially upscaled through the sharing of templates across the EMIS network. Although this project is relatively small, we can easily share this template with a number of other GP practices that are using EMIS. It would certainly be interesting to see whether the improvements seen at this practice can be demonstrated in other practices, leading to a regional or even national improvement in the way URTIs and viral illnesses in children are seen in the GP setting.
One of the main challenges was lack of familiarity with the system. As this practice had only just transitioned to EMIS, there was a very steep learning curve, both in terms of the system itself and the use of the template. This may represent a potential confounding factor. It may be that uptake of template use improved as a result of the interventions we implemented, and with improved familiarity with use of the EMIS system. It would be impossible to tell from our results to what extent this contributed. However it would be very interesting to see whether results can be sustained in the future, and whether a similar project on a different medical problem may achieve similar results. This project was undertaken during a 4-month foundation year 2 rotation where there was no significant staff change-over. Again it would be interesting to see whether with the changes implemented through our PDSA cycles, good documentation of these consultations will be continued in the long term, reflecting improved access and usability of the template.
In terms of generalisability, a template like this clearly can be applied to different medical problems and also used in different GP practices as previously discussed. However one of the main positive features of this project was using informal feedback from users to determine how best to adapt the template to suit their needs. This approach can be used to a certain extent, however, we would give a conservative estimate to the extent to which this could be generalised, for instance to a highly specialised area or to a much larger practice or organisation.
Conclusion
Through this project, we were able to implement a template for documenting consultations of URTIs and viral illnesses in children. This led to a substantial improvement in terms of documentation of key features such as HR and RR and also safety netting information for parents. Respiratory tract infections continue to be one of the most common reasons for consultations by GPs, and it is crucial to be able to determine whether the child may need antibiotic treatment or admission to secondary care. The template acted as a prompt for clinicians as well as a facilitator of quicker and easier documentation of key data. All stakeholders reported that use of the template helped to improve their assessment and documentation of children who presented with such problems. By tailoring this quality improvement project to the needs of the clinicians at the practice, we were able to achieve our initial aims.
To ensure that these improvements are sustainable, new members of the team will be introduced to the EMIS system and the use of the template, while the prompts that have been programmed will remain in place. This template has also been shared with GPs from other practices who can then adapt it to their needs with the hope that we can demonstrate further widespread improvements in the assessment of children who present with this common complaint.
Acknowledgments
The authors thank all the staff at Avon Road Surgery for their help and support in the undertaking of this project, particularly Dr Gouldie and Dr Robson, without whom this project could not have been completed.
Footnotes
Contributors CC and RC contributed equally to this work; CC is overall responsible for the content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.