

Abstract
Objective. To describe the frequency and types of reported adverse events and system improvement recommendations in the Morbidity and Mortality Conference (M&MC) within the Division of Rheumatology at The Hospital for Sick Children, Toronto, Ontario, Canada (SickKids).
Methods. A 5-year retrospective review of the M&MC within the Division of Rheumatology at SickKids was completed. Descriptive data including the number and types of events reported were collected. Events were categorized using an adaptation of the National Coordinating Council for Medication Error Reporting and Prevention Index. Recommendations were classified according to the Institute for Safe Medication Practices Canada.
Results. Between January 2007 and December 2011, 30 regularly scheduled M&MC were held. Eighty-three cases were reviewed. The most common types of reported events were related to “miscommunication” (34.9%), “treatment/test/procedure” (22.9%), “adverse drug reactions” (12.0%), and “medication errors” (8.4%). Category A events (“an event that has the capacity to cause error”) were the most common with 39.8% of the cases, followed by Category C events (“an event occurred that reached the patient, but did not cause harm”) with 28.9%. Eighty-nine recommendations were made. Over half of these were classified as “information” (58.4%), followed by 11 “rules and policies” recommendations (12.4%). Of the 36 action items generated from these recommendations, most are either complete or ongoing.
Conclusion. The M&MC within the Division of Rheumatology reviews a variety of events. Increased reporting of adverse events can lead to system improvements, and has the potential to improve and promote safer healthcare.
High-quality medical care is critical in the treatment of rheumatic disease. Improving rheumatic disease care begins with acknowledging the need to improve and a clear understanding of where to improve1. Physicians are being mandated by government, accrediting specialty societies, hospital credentialing committees, patients, and even mass media2 to demonstrate quality of care assurance and quality improvement. One key dimension of quality improvement is patient safety and the reduction of medical error. Unfortunately, there is little in the rheumatology literature on specific patient safety initiatives that have the potential to improve patient outcomes.
The Institute of Medicine report, “To Err Is Human: Building a Safer Health System”, exposed the magnitude of the patient safety problem in medicine. It suggested that 44,000 to 98,000 people die each year as a result of medical errors in the United States3. These errors are largely caused by faulty systems, processes, and conditions that lead people to make mistakes or fail to prevent them3. Since the publication of “To Err Is Human”, various professional, governmental, and private organizations have paid increased attention to the extent of the medical error problem. These groups have asserted that increased reporting and study of errors will lead to system improvements and safer healthcare. In the Canadian Adverse Events Study4, an estimated 7.5% of patients admitted to acute care hospitals in Canada in the fiscal year 2000 experienced 1 or more adverse events. The study also reports that 36.9% of these patients were judged to have highly preventable adverse events4. Similarly, the Canadian Pediatric Adverse Events Study reported an adverse event rate of 6.5%, of which 44.7% were preventable5. Healthcare staff need to be open to the discussion and study of adverse events and errors to identify and ameliorate the conditions that permit error. According to Leape, the realization that “errors must be accepted as evidence of system flaws, not character flaws” is essential6.
The Morbidity and Mortality Conference (M&MC) is one of academic medicine’s most visible fora for discussion of adverse events and errors; however, despite its longstanding tradition and venerated role in medicine, it is unclear whether the M&MC is effective in its role. The M&MC lacks a precise definition, a standard format, and identified goals. There is marked variability in the process and standards for the M&MC7,8. Publications in the medical literature report survey data showing that participants like the M&MC, believe it to be useful or believe they had learned from the M&MC (e.g., about practice-based learning and improvement and systems-based practice)7,9,10. Further, the M&MC has been shown to be an effective forum for addressing patient safety and quality improvement competencies11. Staff and resident doctors agree that these rounds represent a forum for addressing system-wide problems, as well as identifying, learning from, and if necessary, planning responses to medical error11.
To improve and promote safer patient care, the full scope of adverse events encountered by patients must be understood. The objectives of our present study were to describe the frequency and types of reported adverse events, as well as system improvement recommendations in the M&MC within the Division of Rheumatology at The Hospital for Sick Children (SickKids), Toronto, Ontario, Canada.
MATERIALS AND METHODS
Setting
SickKids is a 300-bed, university-affiliated tertiary/quaternary children’s hospital. The Division of Rheumatology at SickKids is one of the largest pediatric rheumatic diseases units in North America, with 10 staff pediatric rheumatologists. The Division of Rheumatology’s training program offers training at the postgraduate and undergraduate levels. In any given year there are about 6 pediatric rheumatology fellows as well as multiple rotating pediatric residents and medical students. There are 5 dedicated rheumatology nurses along with a physiotherapist, a physiotherapy practitioner, an occupational therapy practitioner, and a social worker.
A hospital-wide policy on the M&MC specifies that every division at SickKids must review every hospital death and all morbidity events12. A morbidity event is defined as “an untoward event or complication which, under optimal conditions, is not a natural consequence of the patient’s disease or treatment”13. The division also reviews all patients transferred to the Intensive Care Unit and those readmitted within 48 h of discharge. The chair of the M&MC is responsible for coordinating division reviews on a monthly basis and moderates the presentation of the reviews. Every year, a rheumatology fellow is assigned the role of overseeing preparation of the agenda of the meeting, which enables them to contribute to the enhancement of quality care and patient safety in their practice. This helps fulfill one of the objectives of training as specified by the Royal College of Physicians and Surgeons of Canada14.
All members of the division, including rheumatology fellows, allied health staff, as well as attending staff physicians, are encouraged to present an event for review in an interdisciplinary forum. This is then followed by a discussion among those present. The discussion is summarized and meeting minutes are forwarded to the overall hospital’s Morbidity and Mortality Committee for review. Where appropriate, disclosure of events to the family is ensured. Finally, the chair ensures that the recommendations made as a result of the event are communicated to the appropriate forum, group, or department.
Data collection and analysis
Minutes of the M&MC within the Division of Rheumatology at SickKids were retrospectively reviewed for a 5-year period (January 2007 to December 2011). Descriptive data including attendance, the number of events, location, and types of events reported were collected.
Events were categorized using an adaptation of the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) Index15. The index was initially created to effectively identify problem areas and trends so that quality assurance and medical committees can implement measures to improve drug use16. This index classifies an error according to the severity of the outcome and helps healthcare practitioners and institutions to track errors in a consistent, systematic manner. The index considers factors such as whether the error reached the patient and, if the patient was harmed, to what degree (Table 1). To better facilitate the description of severity of events reviewed within the M&MC, the word “error” was changed to “event” as suggested by McDonnell, et al17. To ensure reliability, categorization was completed by both the primary author and the senior author independently. Consensus was then reached when disagreement between events occurred.
Recommendations were classified in the categories used by the Institute for Safe Medication Practices (ISMP) Canada18. Figure 1 lists the examples of error-prevention strategies in order of effectiveness for creating lasting system changes. Those listed at the top are more powerful because they focus on changes to the system in which individuals operate18. As the list descends, strategies are presented that target system changes but rely in some part on human attentiveness and memory. Strategies toward the bottom are familiar and often easy to implement, but rely entirely on human vigilance. For example, a forcing function is a procedure that creates a “hard stop” during a process to help ensure that important information is provided before proceeding. Examples include using specially designed oral syringes (not parenteral syringes) that will not connect to intravenous tubing for all liquid oral medications18. Automation and computerization of certain processes and tasks can lessen human fallibility by limiting reliance on memory. Examples include use of technologically and clinically sound computerized drug information systems18. Education and information are important methods when combined with other strategies. However, the effectiveness of these latter tactics relies on an individual’s ability to remember what has been presented. Thus, on their own, they offer little leverage to prevent errors18.

Error-prevention strategies in order of effectiveness, adapted from Institute for Safe Medication Practices (ISMP) Canada18, April 2013. Reprinted in its entirety with permission from ISMP Canada.
Ethics
Our study was approved by the Department of Quality and Risk Management at SickKids as a quality improvement initiative.
RESULTS
Over the 5-year period, there were 30 regularly scheduled M&MC. Attendance was interdisciplinary with an average of 19 individuals per session. Twenty-five percent of participants were staff pediatric rheumatologists while trainees (pediatric rheumatology fellows, pediatric residents, and medical students) made up 45% of the attendance. Nurses and allied health professionals (i.e., physiotherapists, occupational therapists, social workers) made up 20% of the attendance. As appropriate, staff from other divisions in the hospital were invited to participate in the M&MC discussion of certain events. They made up 7% of the average attendance. Administrative staff made up the remaining 3%.
A total of 83 events were discussed (average 2.7 events per session) over the 5-year review. About 40% of the events occurred in the inpatient hospital ward, 26% in the medical short-stay unit (where patients were admitted for the day to receive medication infusions or undergo procedures such as intraarticular corticosteroid injections and lumbar punctures), 16% in the outpatient clinic setting, 11% in the image-guided therapy department (where patients received image-guided intraarticular corticosteroid injections), and 7% in the emergency department. Two deaths and 4 transfers to the intensive care unit occurred.
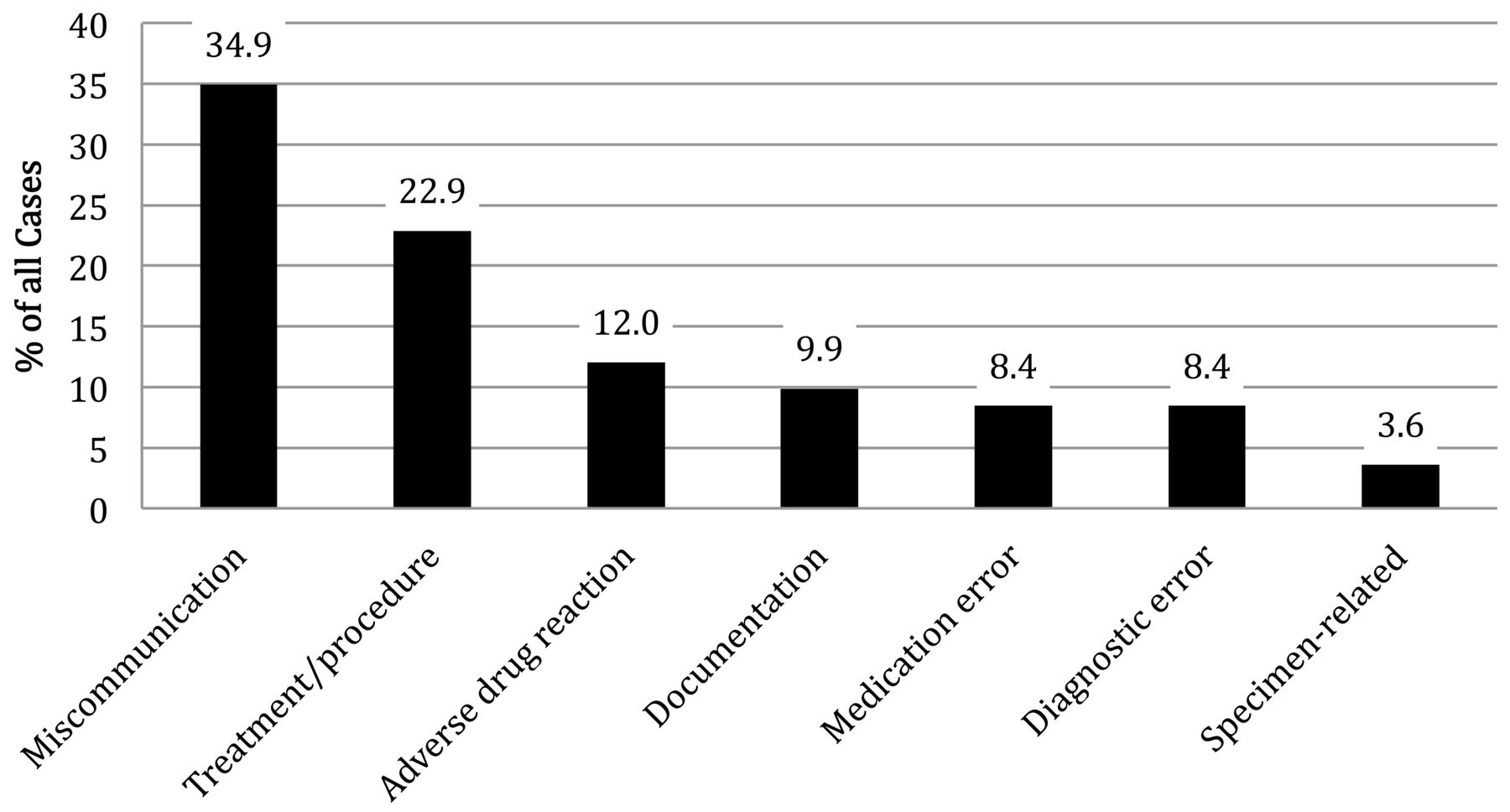
Figure 2 summarizes the types of events that were discussed in the M&MC. The majority of events were considered related to “miscommunication” (e.g., miscommunication between physicians and patients or between consulting services). For example, a patient on another service was discharged home prior to discussing a positive magnetic resonance imaging that required further investigation. The next most common type of event involved a treatment/procedure. For example, there was a series of patients who had significant pain after receiving intraarticular steroid injections of the temporomandibular joint and required a prolonged hospital stay or admission. Of note, we did not include subcutaneous atrophy or skin hypopigmentation following intraarticular steroid injections as adverse events. Adverse drug reactions most commonly occurred in relation to infusion reactions [such as with infliximab, rituximab, or intravenous immunoglobulin (IVIG)]. Medication errors included several events where the wrong dose or drug was given, an extra dose was given, or a drug was omitted. These were usually identified by either nursing or pharmacy review. Examples of documentation errors include mislabeled prescriptions and incomplete or mislabeled test requisitions. Diagnostic errors occurred when a patient did not receive the appropriate investigation for a given clinical presentation. These errors were usually discovered on patient followup when further investigation was completed. For example, a patient with systemic lupus erythematosus with elevated D-dimers was discharged home. On followup, an ultrasound was performed and a venous thrombus was found. The patient was then given antithrombotic therapy. Finally, events related to specimens included mishandling of biopsy samples or synovial fluid not sent to the appropriate laboratory for analysis.

Types of events discussed in the Morbidity and Mortality Conference.
All the events reviewed in the M&MC were categorized according to an adaptation of the NCC MERP Index (Figure 3)15,17. Category A events (“an event that has the capacity to cause error”) were the most common (39.8%). An example of a Category A event included improper handover of a patient to the on-call physician. Category C events (“an event occurred that reached the patient, but did not cause harm”) were the second most common, involving 28.9% of the events. An event in which a patient who is receiving cyclophosphamide was not given a protocol-specific prescription for sulfamethoxazole-trimethoprim prophylaxis is considered a Category C event. About 14.5% of the events fell within Category E (“an event occurred that may have contributed to or resulted in temporary harm and required intervention”); for example, a patient with a known reaction to a particular brand of IVIG had a significant reaction to a second infusion of the same brand and required management of the infusion reaction. Only 11 events (13.2%) were categorized F or higher and would have been recorded as adverse events in the Canadian Pediatric Adverse Events Study5. An example of a Category F event included a patient with juvenile idiopathic arthritis and uveitis who was taking the wrong dose of prednisone. There was confusion regarding the dose in mg versus the dose in ml (a medication book was not being used). The patient was therefore being underdosed and required admission to the hospital for treatment of his active disease.

A total of 89 recommendations were made during the 5-year review (Figure 4). Over half of the recommendations were classified as “information”. There were, however, several policies, checklists, as well as computerization suggestions made (Table 2). This occurred especially when a serious adverse event was presented. A total of 36 action items were generated from these recommendations. Action items included the revision of order sets for medication infusions, the creation of standard checklists for sedation screening, as well as the review of certain procedures such as intraarticular injections of the temporomandibular joint. Most of the action items have been reported as completed (41.7%) or are ongoing (30.6%). An interdisciplinary team (e.g., physicians, nurses, clerical staff, and information services) was involved in the completion of these action items. Most of the action items that were not completed depended on the help of information technology (IT) services. SickKids is currently undertaking a significant update to its IT platform and therefore those action items were put on hold until the update is complete.

Summary of recommendations made over the 5-year review, as classified by an adaptation of Institute for Safe Medication Practices Canada’s error-prevention strategies18.
Examples of recommendations as classified by the ISMP Canada18.
DISCUSSION
The M&MC was originally created in an attempt to improve medical practice through the examination of adverse events and errors19. The M&MC in the Division of Rheumatology at SickKids is well attended by an interdisciplinary team. Fortunately, most of the events did not lead to patient harm. Several recommendations with subsequent action items were generated, most of which have been completed or are ongoing. These recommendations included a wide range of actions, but there were few high-leverage error-prevention strategies that were suggested according to the criteria developed by ISMP Canada18. However, where a serious adverse event occurred, more effective system-level changes were recommended and completed.
There were several themes in the types of events discussed in the M&MC. Most of the events were labeled as “miscommunication”. It is well known that communication breakdowns are involved in the great majority of adverse patient outcomes20. The Joint Commission reported that ineffective communication resulted in 68% of all preventable errors involving death or serious injury from 2010 to the second quarter of 201221. There were several examples of miscommunication between referring and consulting teams, the emergency department, as well as patients and families. Most miscommunication events occurred between our consulting service and the primary responsible team. Ensuring that proper investigations are ordered and results followed, as well as appropriate discharge instructions are communicated to patients and families, remains a challenge when consulting on patients.
It is essential for healthcare practitioners and institutions to track adverse events and errors in a systematic manner. Using the NCC MERP Index15 allowed us to consider factors such as whether an error reached the patient and, if the patient was harmed, to what degree. A pediatric patient safety taxonomy has been described by Woods, et al22. This classification system is composed of 4 main categories: problem type; domain of medical care in which the patient safety event occurred; contributing factors in the patient, environment, and care provider; and outcome. Application of this taxonomy to events discussed in the M&MC can enable an analysis that facilitates the development, application, and evaluation of preventive strategies22,23.
There were several limitations to our study. The number of events discussed in the M&MC may not represent the true number of events experienced by patients given that there is no systematic way of choosing which events are to be presented. Although it is mandated to discuss all deaths and morbidities, less serious events may be underreported. The division also completes online safety/incident reports, which could be another source of information that can be discussed in the M&MC. However, incident reporting has major limitations24. Another potential limitation to our study is that the minutes of the M&MC were used as the only source of detail for all the events discussed. These records may have been incomplete or unclear. Finally, outcomes of the recommendations were not measured and the effectiveness of the completed action items was not assessed.
Despite the above limitations, several key lessons were learned following this review. A robust, multidisciplinary M&MC program has the potential to identify recurring adverse events as well as the ability to create high-leverage recommendations. It is essential to involve trainees in this process in order for them to gain competency in patient safety initiatives within their practice. It would be critical to track recurring adverse events as well as the completion of action items to study their effectiveness in preventing further events.
To improve and promote safer patient care in rheumatology, the full scope of adverse events encountered by patients must be understood. We report a 5-year review of the events discussed in the M&MC in the Division of Rheumatology at SickKids. It is unclear whether the M&MC is effective in its role. However, increased reporting and study of adverse events and errors can potentially lead to system improvements and safer healthcare.
- Accepted for publication August 1, 2014.








{kind=link}
{kind=link}
{kind=link}
{kind=link}