Article Text

Abstract
Objectives To explore the experiences of oncology staff with communicating safety concerns and to examine situational factors and motivations surrounding the decision whether and how to speak up using semistructured interviews.
Setting 7 oncology departments of six hospitals in Switzerland.
Participants Diverse sample of 32 experienced oncology healthcare professionals.
Results Nurses and doctors commonly experience situations which raise their concerns and require questioning, clarifying and correcting. Participants often used non-verbal communication to signal safety concerns. Speaking-up behaviour was strongly related to a clinical safety issue. Most episodes of ‘silence’ were connected to hygiene, isolation and invasive procedures. In contrast, there seemed to exist a strong culture to communicate questions, doubts and concerns relating to medication. Nearly all interviewees were concerned with ‘how’ to say it and in particular those of lower hierarchical status reflected on deliberate ‘voicing tactics’.
Conclusions Our results indicate a widely accepted culture to discuss any concerns relating to medication safety while other issues are more difficult to voice. Clinicians devote considerable efforts to evaluate the situation and sensitively decide whether and how to speak up. Our results can serve as a starting point to develop a shared understanding of risks and appropriate communication of safety concerns among staff in oncology.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
The qualitative approach allowed for an in-depth exploration of the connection between the type of safety issue raising concerns and the decision to speak up. This study is the first to acknowledge the importance of gestures and mimics, that is, non-verbal communication, for speaking up in the clinical context.
-
Participants ultimately self-selected for interview participation and personality traits associated with speaking-up behaviour, like conscientiousness and extraversion, may have also affected the willingness to participate in this study.
-
We sampled doctors and nurses from seven oncology departments, which improves the diversity and generalisability of the data.
Introduction
Medical errors and adverse events pose a serious threat to patients with cancer and have gained increasing attention in the past few years.1–3 Walsh et al reported that of 1262 adult patient visits involving 10 995 medications, 7.1% were associated with a medication error. Several interventions and strategies have been recommended to increase patient safety in oncology, for example, electronic prescribing, standardisation of processes and use of checklists for safe administration of drugs.4–8 However, communication failures often undermine the effectiveness of these safety tools, sometimes with severe consequences. The external inquiry into the disastrous case of David James who died of an intrathecal administration of vincristine is an early report of a tragedy of ‘silence’: the junior doctor knew that vincristine should not be given intrathecally, but failed to speak-up and to challenge the senior colleague.9 ‘Silence’, that is, not voicing safety concerns, is a common behaviour among healthcare professionals (HCP). The ‘Silence Kills’ study revealed that 84% of physicians and 62% of nurses reported peers taking shortcuts that could be dangerous to patients (eg, not washing hands, failing to check wristbands). Eighty-five per cent of nurses reported that they had been in a situation where a safety tool, for example, the surgical safety checklist, had warned them of a problem but 58% had also been in situations where they felt it was unsafe to speak up to their colleagues.10 In a qualitative study among residents in the USA, communication failures were reported as strong contributors to medical mishaps and were a consequence of individual relational and systemic factors.11 Residents typically navigate in complex relations and power discrepancies, do not want to appear incompetent and often hesitate to communicate to superiors. Blatt et al12 analysed 77 lapses in reliability and residents’ awareness and behaviours of these lapses. Residents chose to remain silent and did not correct or mitigate the mistake in 61% of the lapses they realised in real-time and they could do something. Many residents thought their silence contributed to adverse patient outcomes and expressed regret for not having voiced their concerns.
‘Speaking up’ can be defined as assertive communication in clinical situations that require (immediate) action through questions or statements of opinion or information with appropriate persistence until there is a clear resolution to prevent error or harm from reaching the patient.13 ,14 Speaking up about patient safety is vital to avoid errors reaching the patient and thus to prevent harm and to improve a culture of teamwork and safety. In oncology, a multiprofessional and complex area of healthcare, in which single small errors may result in serious patient harm, effective and assertive communication about errors and risky behaviours between team members is essential. However, very little is known about factors that determine HCPs’ willingness to speak up for safety. In interdisciplinary action teams, for example, in operation rooms, two barriers have been identified that inhibit speaking up: power discrepancies, for example, between nurses and the surgeon, and the staff's lack of conviction that their input is needed and desired, that is, little motivation that makes the effort and risk worthwhile.15 Research on employee silence suggests that decisions to speak up are strongly influenced by organisational and situational context and their interaction effects with individual-level factors.16 For example, the potential of harm and the social relationship between the observer and the actor of a risky behaviour vary from situation to situation and affect the decision to voice concerns.17 Lyndon18 investigated the agency for safety (taking a stand on an issue of concern) among nurses, midwives and doctors in perinatal care. She found HCPs’ willingness to engage for safety to be highly variable and dependent on situational factors. In particular, poor social relationships and the novelty of the situation were barriers to agency for safety. HCPs were motivated to preserve good relations with their coworkers and supervisors and the perceived risk of conflict inhibited speaking up. For example, knowing the involved colleague helped to anticipate his/her response to expressing safety concerns. To understand HCPs’ speaking-up behaviours, their facilitators and barriers, it is crucial to study these contextual factors. The aim of our study is to explore the experiences of oncology staff with communicating safety concerns to their colleagues and supervisors and to examine situational factors and motivations surrounding the decision whether and how to express concerns.
Methods
Interviews
We conducted semistructured interviews with experienced oncology staff. The topic guide was developed based on prior research, the literature and discussions with oncology experts.19–22 Figure 1 displays sample questions from the interview guide. The interviews began with general questions on how often participants experience situations that they felt would require voicing their concern and whether they generally feel comfortable to raise patient safety issues with coworkers and supervisors. The central part of the interview asked participants about situations where they experienced concerns about patient safety and decided whether and how to communicate them. Participants were asked to describe these situations and the context surrounding them in detail. We assessed the clinical circumstances and what exactly had raised their safety concerns, who was involved, whether and how they communicated their concerns, how those involved responded to the participants’ actions, whether and how the situation was resolved and whether any consequences resulted from the episode. They were asked to elaborate on their strategies for articulating safety concerns. The guide included various prompts and subquestions for each section. Examples (missed hand disinfection, medication error) were prepared as triggers for participants who could not access their own experiences ad hoc.

Sample questions from the interview guide (translated from the original in German).
Sample
Six hospitals participated with seven oncology departments. These included three regional hospitals and two university hospitals with adult oncology units, and two paediatric university hospital departments. One university hospital participated with its adult and paediatric oncology department Nurses and doctors working at the oncology departments of the participating hospitals received written study information and were invited to register for an interview. Interviewees were purposively sampled to include doctors and nurses, staff working at the ambulatory oncology units or on wards and with sufficient working experience in oncology. Interviewees gave prior written informed consent. Interviews were conducted face to face at the hospitals by a trained and experienced research assistant, audiorecorded and transcribed verbatim. The study was exempted from full ethical review by the Cantonal Ethics Committee (KEK-StV-Nr. 58/13).
Data analysis
An inductive thematic content analysis framework was applied to the transcripts.23–26 After listening to interviews and reading the transcripts to become familiar and get a sense of the whole, two researchers independently analysed and coded a subset of transcripts (open coding) using a mixed-methods research software.27 The texts were excerpted into units of meaning (words, sentences or paragraphs). Emergent themes and recurring ideas were identified and classified in terms of the concepts arising from it. The code structure was discussed and revised and applied to the next subset of transcripts in an iterative process. Again, areas of disagreement were discussed in feedback loops to increase validity.25 ,28 New codes were added as additional themes emerged and some codes were eliminated. The finalised code structure was then applied to all transcripts by both researchers, and any discrepancies were solved.24 ,29 The inter-rater reliability of code application on a sample of excerpts (n=255; 23%) was good (Cohen's κ=0.78, CI 0.77 to 0.81). Categories were abstracted as far as possible by grouping subcategories as categories and categories as themes.25 Data were organised in major themes relevant for the research question. Representative quotes were selected.
Results
Interviews were conducted with 32 doctors and nurses in oncology. The interviews lasted, on average, 42 min (range 21–58 min). Characteristics of the participants are provided in table 1. Participants frequently experienced clinical care situations which raised their doubts and required clarification or correction. Interviewees felt generally comfortable to voice their thoughts. Some referred explicitly to a special ‘culture in oncology’ making it easy to express concerns even towards supervisors—in contrast to other areas of medicine.
Characteristics of participants (n=32)
Situations raising safety concerns
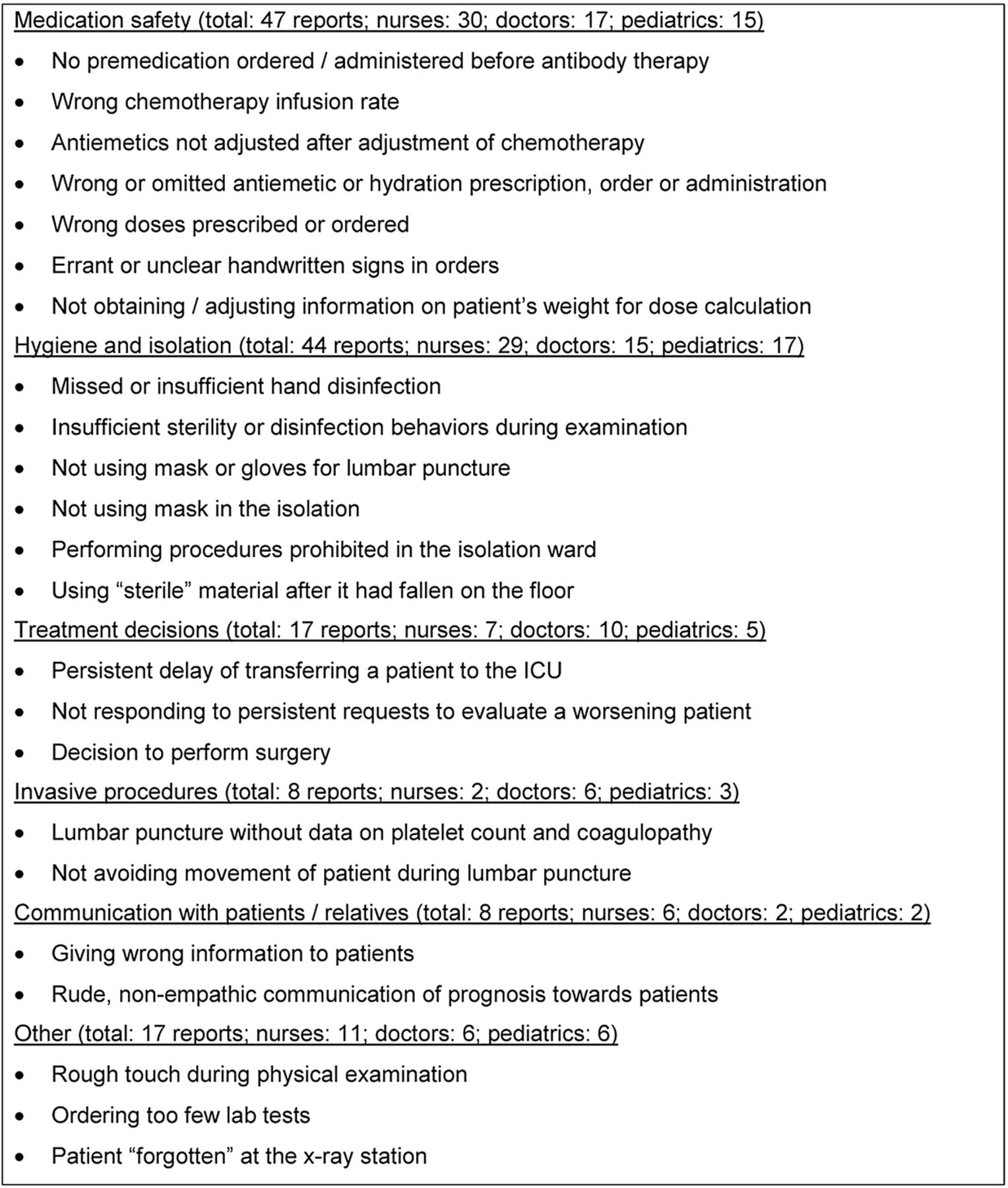
We obtained a wide variety of detailed situations in which participants had experienced safety concerns and deliberately decided whether and how to communicate these (examples are provided in the online supplementary appendix). The safety issues prompting concerns included the entire continuum of medication safety (47 reports), hygiene and isolation (44 reports) and, less frequently, treatment decisions (17 reports), invasive procedures (8 reports), communication with patients and relatives (8 reports) and other issues (17 reports). Reports involved single or multiple episodes of effective or potential errors (eg, slips of action) and observed violations of safety rules. Figure 2 displays the frequency of reports together with typical examples and by professional group.

{kind=link}
{kind=link}
Examples of safety issues which triggered participants’ safety concerns.
The vast majority of interviewees reported at least one episode where they decided to express their concerns. However, 13 participants also reported situations where they remained silent and did not act on their concerns. Hierarchical constellations and violations of norms were often provided as reasons for not expressing concerns.
You cannot do this as a resident. You cannot say ‘Professor, we have to discuss this.’ That is simply inadequate. That [violation of disinfection rules] needs to be brought up by the chief or a senior.
Senior doctor, ambulatory unit (C108)
Most episodes shared some common characteristics: in the typical constellation, (1) only two persons, the actor (the person the error was attributed to or who performed the questionable behaviour) and the interviewee (the person observing or discovering the error or violation), or multiple persons of mixed professions (doctors and nurses) were present; (2) the observer (interviewee) was of lower hierarchical status than the actor; and (3) the actor was a doctor and the interviewee was a nurse, or the actor and observer were doctors. We obtained only a few reports of constellations that involved equal-status team members and nurses as actors (and either nurses or doctors as observers).
Speaking-up behaviours and their relation to the safety issues which triggered them
Participants’ speaking-up behaviour was strongly related to the clinical safety issue. Nearly all episodes of ‘silence’ were connected to hygiene, isolation and invasive procedures. In contrast, across the hierarchies, professions and hospitals, there seemed to exist a strong culture to communicate questions, doubts and concerns relating to medication. Interviewees emphasised the importance of voicing medication safety issues. Speaking up about medication safety occurs frequently, is well accepted and even expected by staff and is usually easy to communicate.
In this issue [medication], I feel that doctors are very appreciative if we as nurses remain vigilant and speak to them, speak immediately. Better stop an infusion and ask back. In this issue [medication], it is not about keeping it confidentially but you are encouraged to act.
Nurse, ward (C114)
Some informants were well aware of their different behaviours relative to the cause of their concern.
This is about numbers and facts, and there is an error in the prescription or calculation or in writing, whatever. It is not so much on the personal level and therefore it wouldn't be too difficult for me [to speak-up]. It is easier to say something than… about behaviors. Disinfection of hands is something different. It's different to a prescription, where numbers are wrongly noted.
Nurse, pediatric ward (L230)
Types of ‘voice’ used
Informants described several voicing behaviours to communicate their safety concerns, many of which did not involve using their ‘voice’. Every second participant had used gestures or facial expressions to signal actors their concerns, mainly (but not exclusively) when safety rules of hygiene were violated. The main motivation for not using verbal expressions was to reduce intrusiveness and to avoid exposing the actor in front of patients or coworkers.
I do it with my hands. I would not voice. In particular, if it is a supervisor, I would not say it out loud.
Senior doctor, ward (B102)
I often give nonverbal signals, bring the gloves.
Nurse, ward (C112)
That you do not comprise him [the supervisor] but better say ‘Here, didn't you want to use the mask?’ or ‘The masks are there behind you.’ More as if to point him to the issue but not to make him look stupid... Or I take the mask myself and see whether he reacts upon that or I take one for me and pass one mask to him.
Resident, pediatric ward (J122)
Clinicians working at the paediatric oncology units were very much concerned about the presence of parents in situations requiring speaking up and reported switching to non-verbal communication (eg, harrumphing) with the expectation that parents would not understand the information. Nearly all interviewees were concerned with ‘how’ to say it. They invested considerable efforts in ‘diplomacy’, ‘a good communication style’, ‘choosing their words carefully’ and ‘selecting their strategy relative to who the actor is’. A third of the respondents explicitly elaborated that they would choose their voicing strategy based on who the actor was.
I would rather say ‘I'm used to doing it like this...’. A little relativized. With the nurses, I would go more directly ‘It should be done like…‘. With a supervisor, I'd say ‘I remember it being done like.‘.
Nurse, ambulatory (C113)
Senior clinicians used ‘good clinical reasoning’ and provision of well-considered arguments when questioning coworkers or supervisors. Preparing themselves and postponing the voicing of concerns to a bilateral confidential communication situation with the actor was also commonly mentioned. A third of the participants also described occasions where they did not express their concerns but tried to work around or rectify the error tacitly without confronting the actor. Some participants, in particular those of lower hierarchical status, reflected on deliberate ‘voicing tactics’. For example, residents commonly framed their concerns as naïve questions and embedded signals of ‘being a learner’, ‘inferiority’ or ‘acknowledgement of their limited experience’—even if an error or rule violation was obvious to them.
I first inspect everything, so that I for myself am sure whether it is right or wrong. And when I verified that it is definitely wrong, I would ask him [the senior] ‘I'm not quite sure whether this is optimal?’.
Resident, ambulatory unit (C107)
If a senior filed the prescription…you have to ask very naively.
Resident, adult ambulatory oncology unit (B103)
So as if I as a resident want to learn something ‘Wouldn't one need to use gloves when touching an open wound? Or is it sufficient to just use alcohol rub?’
Resident, ambulatory unit (P127)
I asked ‘Excuse me, I thought that it is usually done like this. Is there any special cause why a higher dose had been prescribed to this patient?’ He can then reason and notice that he had made an error.
Resident, ambulatory unit (X110)
Similarly, nurses often deliberately feigned ignorance or used open questions to challenge doctors’ behaviours or violations of rules or errors.
They [doctors] are very much up themselves. This and that is correct and we [nurses] have to do it this way. But I put it as: ‘The value [INR] is below 4… Should I really administer it [the medication]?’ Pretending to be a little dumb. Usually it is being well accepted then.
Nurse, ambulatory unit (P229)
I said ‘I saw this but I thought it is done so and so, and whether I'm wrong?’ More like, to prevent that I will make an error in the future rather than she actually made an error.
Nurse, ward (J216)
Consequences of speaking up
Participants mainly reported constructive reactions to their speaking up. Frequently, the coworker at whom the expression of concern was directed appreciated it, responded with gratitude or an apology and fixed the error or behaviour if possible. From the elaborations of some doctors, it was clear that there existed a hidden line between incidents when speaking up towards them is warranted and welcomed and incidents which would not justify voicing, based on what they perceived as a safety problem.
In the order form there are columns for the chemotherapy drugs and columns for the co-medication. Sometimes I write the steroids in the wrong, chemotherapy column. And they [nurses] point me to that. It is okay, but… contrariwise I think that this is not a safety problem. If I would forget it [the steroid order] this would be relevant. But whether I write it in this column or the other, that is not relevant. I have ten patients waiting for me and we discuss in which column to write… that causes some aggressions, I have to admit. It's just nit-picky.
Senior, ambulatory unit (C108)
Five participants experienced strong negative responses like disrespect or anger after they spoke up. Surprisingly, simply ignoring their colleagues’ expressions of concern without any change in behaviour or revision of an error was a common response to speaking up. Nurses, in particular, felt often ‘simply not being heard’ when pointing doctors to their violations of hygiene guidelines. If insistently speaking up was unproductive, these episodes often left feelings of frustration and resignation.
Sometimes they [doctors] just slip away, ‘You have nothing to tell me’.
Nurse, ambulatory unit (P225)
Eventually, you simply remain silent. What can you do?
Nurse, ward (J221)
I could discuss two or three hours with him, without any result, because he wants it this way and he does it this way—and that's it.
Nurse, ambulatory unit (P225)
Discussion
To the best of our knowledge, this is the first investigation into the communication of safety concerns among clinical oncology staff. Our results suggest that nurses and doctors in oncology commonly experience situations which raise their concerns and require questioning, clarifying and correcting. Although we found a high level of general preparedness to speak up, our rich data provide a more detailed and mixed picture. Our results indicate a broad and widely accepted culture to discuss any questions or errors relating to medication safety and, in particular, antineoplastic drugs. Clinicians in our study clearly expected their coworkers to voice such concerns and to respond to others speaking up in an appropriate and receptive style. Three details seemed to foster the willingness to speak up in medication safety: a collective understanding of the high potential for harm; the belief that one's speaking-up behaviour will be well received by coworkers because it is less ‘invasive and personal’; and finally, the fact that the constellation for expressing concerns often is—or can be shaped to be—a constructive, bilateral professional communication. In contrast, participants in this study found other safety issues more difficult to voice. Many participants reported episodes of silence when confronted with coworkers’ or supervisors’ violations of hygiene and safety rules. Reluctance to speak up about behaviours related to hospital hygiene has been reported outside oncology previously. In a survey study, medical students were willing to speak up to fellow students about inadequate hand hygiene, but this willingness decreased stepwise with individuals who were further up the medical hierarchy.30 In an exploratory study using case scenarios of potentially harmful clinical situations, Lyndon et al14 found that nurses’ and physicians’ perceptions of potential harm of missed hand disinfection differed considerably and were strongly linked to likelihood of speaking up.
Our study reveals a notable range of voicing tactics used by oncology staff. Clinicians evaluate the situation and sensitively decide whether and how to speak up based on the specific constellation. Efforts are made to avoid intrusiveness and showing a coworker or supervisor up. In situations which require immediate action and with multiple persons present, participants in our study used a variety of non-verbal cues, gestures and signs to attract the attention of the ‘wrongdoer’ and articulate the undesirable behaviour without vocalising the violation. It is alarming that those of lower hierarchical status (nurses and residents) feel a need to frame their observations, doubts and concerns as naïve questions by degrading their own expertise. Obviously, these groups of staff make the experience that this is an effective and less dangerous way of communication. As researchers from other fields, we found feelings of futility and resignation to be not uncommon among staff, in particular among nurses. In their model of employee silence, Milliken et al22 include the belief that ‘speaking up will not make a difference’ as an important contributor for the likelihood of remaining silent in the future.
Limitations
This study has some limitations connected to the study design. First, our findings are based on the personal accounts of participants. In relation to medication safety, we found strong social norms to voice any safety concerns. ‘Speaking up’ in this context was clearly labelled as socially desirable. Participants may have unconsciously presented themselves as more active and assertive as they actually are or may have concentrated on reports of situations where they decided to speak up. Future research should employ other designs, in particular, observational methods to study communication of safety concerns. For example, in a full-scale simulation study in anaesthesiology, nurses and residents challenged an attending in only few of the critical situations created by the attendant, including fatal drug administrations.31 However, the richness of our data could not easily be generated by observation. For example, we obtained many reports of complex and changing constellations. Second, as qualitative research, the accuracy of our study is threatened by undetected researcher influences. Reflexivity during the research process is an important strategy to ensure credibility.32 In our study, interviews were conducted by an experienced and trained interviewer with no specific background in the research question. After each interview, the interviewer made field notes and documented, in particular, personal accounts, questions, emotions and reflected on her impressions.33 These documents and the interview recordings were used in the regular discourse between the interviewer and the researcher. We discussed the role and influence of the interviewer, our subjectivities and preconceptions and the social relationships with participants. Two researchers with different theoretical backgrounds analysed the data by mutual collaboration. We used the transcripts and the original audio files to identify and reflect on our own beliefs, mental models, positions to the interviews and what we, as individuals, ‘hear’ in the data. These reflections spanned the entire range of data analysis and interpretation, from the meaning of single words used by interviewees to main concepts of social interactions in hospitals. We made explicit what we found to be outside our assumptions. These steps contribute to the validity of this study. Third, while we tried to encourage a diverse group of staff, participants ultimately self-selected themselves for the interview. Personality traits associated with speaking-up behaviour, like conscientiousness and extraversion,34 may have also affected the willingness to participate in this study. Again, this may have led to an overestimation of voicing behaviours and an underestimation of ‘silence’ among staff. As a strength of this study, we recruited doctors and nurses from seven units in six hospitals, including paediatric departments. This diversity suggests that our results are not much influenced by any specific organisational culture.
Implications for practice and future research
Our study has some important implications for practice and future research. First, oncology staff need to be much more aware that the safety of patients with cancer comprises more than antineoplastic drug safety, though, of course, these drugs have a considerable potential for harm. Patients with cancer are severely affected by hospital-acquired infections and precautions need to be taken seriously. Second, our results emphasise the importance of teaching and training health professionals in the use of assertive communication. Medical and nursing students and clinicians should be given the opportunity to learn, at best in multidisciplinary settings, how to question and challenge the actions of coworkers and higher-ups when patient safety is impacted. Participants in our study were particularly concerned with the ‘how to's’ and many recalled instances in which they wanted to speak up but simply did not know how to find the right words and actions. Thus, practical training (eg, using roleplay) and acquiring and adopting advocacy and inquiring language is essential. Several training programmes have been developed recently, but evidence about their success is still limited and mixed.35–37
Third, we found non-verbalising ‘voicing behaviours’ to be a quite common strategy in our sample. Simply speaking, the fact that healthcare workers do not literally speak up does not necessarily imply that they do not express their concerns. Obviously, for sensitive issues, gestures and signs are easier and less precarious to perform and to receive. Actively training staff in the use of gestures for speaking up (rather than remaining silent entirely) could decrease barriers to communicate concerns. However, before non-verbal speaking-up behaviours could be recommended, research is clearly needed into the effectiveness and risks of this communication. For example, in some of our case reports, those violating safety rules occasionally did not respond to their coworkers’ gestures, either because they had not recognised them or had not interpreted them as intended, or because they had deliberately decided to ignore them. Fourth, our results also indicate that at least some doctors have clear ideas of what poses a safety threat and they want to be made aware of—and what not—and that this perception differs from what nurses find important to clarify or correct. We suggest that these differences should be discussed in oncology units and appropriate behaviours acceptable to both professional groups be agreed on. The established culture of speaking up relating to antineoplastic drug safety clearly indicates that a shared understanding of risks and appropriate communication of safety concerns is achievable.
Acknowledgments
The authors thank the nurses and doctors for their openness and for sharing their thoughts with us in the interviews. They also highly appreciate the support by the following clinical mentors at the study hospitals: Daniel Aebersold, Sabine Blättler, Beatrice Brinkers, Katrin Conen, Karin Etter, Martin Fey, Michael Grotzer, Kurt Leibundgut, Walter Mingrone, Miklos Pless, Heidi Scheel, Isabelle Schelling, Esther Squaratti-Heinzmann, Martin Wernli. Finally, the authors thank Jeannine Ammann for conducting the interviews.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors DS drafted the manuscript. KG revised it critically for important intellectual content. DS and KG made significant contributions to the study conception and design, as well as coordination and data analysis and interpretation. DS and KG read and approved the final manuscript.
-
Funding This work was supported by Krebsforschung Schweiz (Cancer Research Switzerland, KFS-2974-08-2012). The funding source had no influence on the study design; in the collection, analysis and interpretation of the data; in the writing of the manuscript; and in the decision to submit the manuscript for publication. The views expressed and any errors are the sole responsibility of the authors.
-
Competing interests None.
-
Ethics approval Ethics commission of the Canton of Zurich.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.