Article Text

Abstract
Introduction Patients with cardiovascular disease are living longer and are more frequently accessing healthcare resources. The Evaluation of the Methods and Management of Acute Coronary Events (EMMACE)-3 national study is designed to improve understanding of the effect of quality of care on health-related outcomes for patients hospitalised with acute coronary syndrome (ACS).
Methods and analysis EMMACE-3 is a longitudinal study of 5556 patients hospitalised with an ACS in England. The study collects repeated measures of health-related quality of life, information about medications and patient adherence profiles, a survey of hospital facilities, and morbidity and mortality data from linkages to multiple electronic health records. Together with EMMACE-3X and EMMACE-4, EMMACE-3 will assimilate detailed information for about 13 000 patients across more than 60 hospitals in England.
Ethics and dissemination EMMACE-3 was given a favourable ethical opinion by Leeds (West) Research Ethics committee (REC reference: 10/H131374). On successful application, study data will be shared with academic collaborators. The findings from EMMACE-3 will be disseminated through peer-reviewed publications, at scientific conferences, the media, and through patient and public involvement.
Study registration number ClinicalTrials.gov Identifier: NCT01808027. Information about the study is also available at EMMACE.org.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Cardiovascular health and care
The past 10 years has seen a decline in mortality rates from cardiovascular disease.1 ,2 In the UK, from 2003 through 2010, the risk of in-hospital mortality from acute coronary syndrome (ACS) has fallen by half.3 ,4 Nevertheless, cardiovascular disease is the leading cause of death in the UK and is responsible for over four million deaths per year in Europe.5 ,6
In addition, cardiovascular disease confers a substantial morbidity and financial burden.7 ,8 Elderly patients with ACS account for more than half of all admissions to hospital.9 ,10 As a result of reduction in mortality rates, patients are living longer and more frequently accessing healthcare services. The forecasted impact of heart failure, cerebrovascular disease and recurrent ACS as a result of improved survival is unprecedented.7 ,11 ,12 Moreover, cardiovascular disease already costs the UK economy £29.1 billion in healthcare, informal care and productivity losses.8 Consequently, there are new challenges for making the best use of scarce healthcare resources. Future policies will require enhanced regulatory apparatus to respond to the increasing demand.
Two important questions facing healthcare decision-makers are: (1) how do patients recover from ACS and (2) how does their initial presentation and hospital care impact on subsequent healthcare resource use and health-related outcomes? Recently, a succession of large-scale UK observational studies were funded—aiming to improve the understanding of variation in cardiovascular quality of care and outcomes.13 We also have sought to anticipate and understand these challenges. In this paper we describe the profile of the Evaluation of the Methods and Management of Acute Coronary Events (EMMACE)-3 study, a unique national collaborative research effort collecting repeated measures for medicines and their adherence profiles, health-related quality of life, cardiac rehabilitation, hospital readmissions and cause-specific mortality in patients who have been hospitalised with ACS.
Evaluation of the Methods and Management of Acute Coronary Events
EMMACE-3 is the third in a series of prospective studies. EMMACE-1 and EMMACE-2 were regional, multicentre, cross-sectional evaluations of around 2500 patients, hospitalised with ACS, in each study, undertaken in 1994 and 2003, respectively. The National Service Framework for Coronary Heart Disease, a major initiative in this area, was introduced between these 2 studies, 5 years before the start of EMMACE-2.14 The original study (commissioned by NHS R&D) was tasked with assessing alternate methods of case ascertainment and their impact on assessment of quality of care.15 The studies have each reported variations in hospital outcomes,16 ,17 temporal improvements in the adherence to guideline-recommended therapies and their association with a decline in mortality rates,18 impact of cardiac rehabilitation on survival,19 impact of clinical investigations and treatments on mortality,20–22 and the relative impact of diabetes on early and late mortality by temporal changes in hospital care.23 ,24
Aims and objectives
The objective of EMMACE-3 is to improve the understanding of the effect of quality of care on health-related outcomes for patients hospitalised with ACS. The study aims to (1) quantify variation in health-related outcomes from ACS, (2) identify modifiable factors that could lead to improved quality of care and health, (3) investigate the longer term trajectories of recovery from ACS and (4) describe the use of guideline recommended medicines. On completion, the study will allow the evaluation of the full pathway of care from hospital to community, providing data that other cardiovascular studies lack.
Methods and analysis
Study design
EMMACE-3 is a multicentre, longitudinal cohort study of ACS outcomes from the time of hospital discharge over 1 year. The combined primary end point is the time to first occurrence of a major adverse cardiovascular event (MACCE), defined as one of the following: death, non-fatal acute myocardial infarction and coronary revascularisation. The secondary endpoints are (1) quality of life assessed using EuroQol 5-dimension, EQ-5D25; (2) readmission to hospital with ACS; (3) new diagnosis of, or hospitalisation, for heart failure; (4) medication use and patient adherence profiles; (5) cessation of smoking and (6) completion of cardiac rehabilitation.
Study setting
EMMACE-3 is based at the University of Leeds, who is its sponsor. Data storage, linkage, sharing and other processing will be undertaken at the University of Leeds in partnership with Leeds Teaching Hospitals NHS Trust. EMMACE-3 forms part of a portfolio of collaborative cardiovascular studies using electronic health records (EHRs) working with a number of partner organisations including the Farr Institute, University College London and the National Institute for Cardiovascular Outcomes Research, University College London. The EMMACE-3 investigators and collaborators are a multidisciplinary team of epidemiologists, biostatisticians, health service researchers, health informaticians and clinical cardiologists.
Study timeline
EMMACE-3 began on 1 November 2011 and completed recruitment of 5556 patients on 17 September 2013. For up to 10 years data will be gathered on these patients using surveys and EHRs as part of EMMACE-3X study.
Inclusion criteria
The study includes patients aged 18 years or older, who have been admitted with ACS at one of the participating hospitals in England. The spectrum of ACS phenotypes includes ST-elevation myocardial infarction (STEMI), non-STEMI and troponin negative ACS (unstable angina).26
Exclusion criteria
Patients at a terminal stage of any illness, and those in whom follow-up would be inappropriate or impractical were excluded from the study.
Recruitment
Figures 1 and 2 illustrate the spatial coverage and rate at which 5375 participants (excluding multiple entry records) with ACS from a total of 48 hospitals volunteered to be part of this project. Each hospital provided their own recruitment support (research nurses) funded through the NIHR-CLRN funding stream (5.2 Research Support Services V.5). This model encouraged an exponential rate of new centre participation as each hospital acted as active stake-holders in the funding model.

Regional map of English National Health Service hospitals and patients participating in Evaluation of the Methods and Management of Acute Coronary Events (EMMACE)-3.
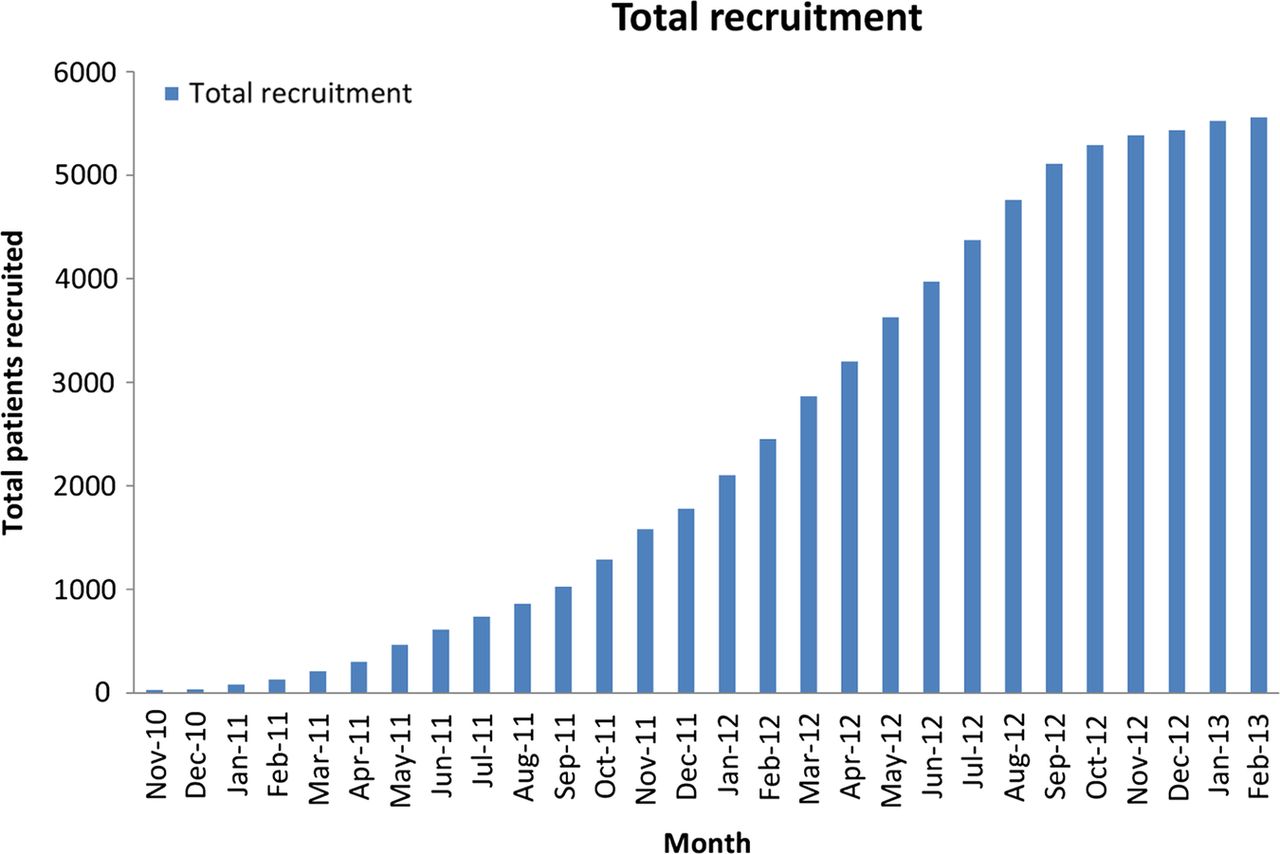
Evaluation of the Methods and Management of Acute Coronary Events (EMMACE)-3 cumulative recruitment of participants.
Data collection
Routine clinical information are being gathered from hospital records and clinical databases and supplemented with data from questionnaires at three time points over the first year after hospital discharge.
EMMACE-3 combines self-reported longitudinal data on numerous health parameters with cross-sectional disease-specific clinical information (figure 3). The cross-sectional data, which are summarised in tables 1 and 2, include: (1) demographic data such as age, sex, place of treatment and residency, (2) information from the national heart attack registry (Myocardial Ischaemia National Audit Project, MINAP),27 (3) a survey of hospital-level cardiovascular facilities and (4) patient-level deprivation indices (Index of Multiple Deprivation score, Townsend score).28
Baseline patient characteristics
Distribution of EMMACE-3 hospital cardiovascular facilities

Flow chart of the EMMACE studies. MINAP, Myocardial Ischaemia National Audit Project; NHS, National Service Framework; HES, Hospital Episode Statistics; EQ-5D, EuroQol 5-dimension; EMMACE, Evaluation of the Methods and Management of Acute Coronary Events.
Longitudinal data are being collected at four time points: in-hospital, and 1, 6 and 12 months postdischarge (figure 3). These include measures of: (1) health-related quality of life (EQ-5D),25 (2) general practitioner and hospital specialists appointments, (3) physical activity, (4) cardiac rehabilitation, (5) prescribed medications and (6) indices of medicines-taking behaviour including the Morisky Medication Adherence, Adherence Estimator, a modified version of the Single Question Questionnaire, Beliefs about Medicines Questionnaire and other adherence probing questions.29–33
Before each participant is sent a questionnaire their mortality status is checked using the NHS Summary Care Record. Non-responders are issued a second and third questionnaire, and/or contacted directly by telephone. Each patient’s data are tracked for cause-specific mortality and date of death (from linkage to the Office for National Statistics).
Attrition rate
Figure 4 shows that of the survivors, 99.1%, 82.9%, 72.7% and 61.2% completed in-hospital, 1, 6 and 12 month questionnaires, respectively. At these latter time points 0.4%, 0.9%, 2.5% and 2.1% of the questionnaire data attrition was due to deaths. The characteristics of patients by return or not of their questionnaires are shown in table 3.
Patient characteristics by response to questionnaire

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Flow diagram showing number of EMMACE-3 participants at each phase of the study (ACS, acute coronary syndrome; EMMACE, Evaluation of the Methods and Management of Acute Coronary Events).
Electronic health records linkage
EMMACE-3 embraces the efficiency of contemporary observational research design. It imports, pools and links EHR information derived from existing national clinical and administrative data warehouses to patient-level repeated measures survey data. For mortality status the linkage success was 96%. Presently, for MINAP and hospital cardiovascular facilities data, the import success is 66.2% and 100%, respectively (table 4).
Data sources, types of data and collection system linked in the EMMACE-3 study
International cardiovascular research platform
Each participant was asked if they would be willing to have their contact details and clinical data securely stored on a database, and to be contacted for potential participation in future observational studies and clinical trials. In total, 5375 consented to participate in EMMACE-3 and 3875 to have their data stored for the purposes of re-contact for future research.
Statistical analysis
Shared frailty survival models (nesting patients within hospitals) will be used to estimate factors associated with time to primary endpoint. Factors to be evaluated will include medications, health-related quality of life and hospital facilities data and baseline clinical characteristics using a significance level of 0.05. Sequential health-related quality of life data will be studied as a measure of outcome (recovery pattern) and predictor of outcome (prognostic marker). Missing data will be multiply imputed, with values derived from an imputation model based on the observed values.34 Statistical analyses will be performed using Stata V.12.1 (StataCorp).
Collaboration
One of the goals of EMMACE-3 is to enable and facilitate national and international collaborations. The rich patient-level data will be an important resource for the identification of cardiovascular participants into trials. Further information about the study is available at ClinicalTrial.gov (NCT01808027), EMMACE.org. Collaborators are invited to contact the chief investigator (CPG) at c.p.gale@leeds.ac.uk. Data will be available to non-commercial research organisations subject to approval by CPG. Only pseudonymised data will be released to collaborators.
EMMACE-3X
EMMACE-3X is an EMMACE-3 extension study with favourable ethical opinion (13/YH/0277) and is adopted onto the NIHR CRN portfolio. Patients recruited to the EMMACE-3 study are being re-contacted and invited to participate in the EMMACE-3X study. EMMACE-3X aims to collect health-related quality of life data using the EQ-5D25 and MacNew35 questionnaires as well as medication data for each participant annually until death or up to 10 years. Furthermore, EMMACE-3X will link EMMACE-3 data with Hospital Episode Statistics (HES) and primary care data (figure 3). Further information about EMMACE-3X is available at ClinicalTrial.gov (NCT01955525), EMMACE.org.
EMMACE-4
EMMACE-4 has favourable ethical opinion (12/WM/0431) and is the latest active study in the EMMACE series. It is adopted onto the NIHR CRN portfolio and will accrue 8000 participants across England. It, also, is a longitudinal study of ACS trajectories of recovery after hospitalisation with ACS. EMMACE-4 will enhance its data collection using EHR data from primary care (using databases such as: The Phoenix Partnership (TPP) Research One and The Clinical Practice Research Datalink (CPRD)), pharmacy databases and from linkage to HES data. In addition, it is collecting patient-reported experience measures (The Picker Patient Experience Questionnaire PPE-15),36 repeated measures of EQ-5D,25 Brief Illness Perception (IPQ),37 the Satisfaction with Information about Medicines Scale (SIMS),38 a modified version of the Single Question Questionnaire,32 medications adherence and cause-specific mortality (figure 3). Further information about EMMACE-4 is available at ClinicalTrial.gov (NCT01819103), EMMACE.org.
Strengths and limitations
EMMACE-3 is a contemporary longitudinal study of detailed trajectories of quality of healthcare and outcomes for ACS. Other observational cardiovascular studies have been instrumental in realising the research potential of linked EHRs, but have been limited by their lack of data for health-related quality of life and medication adherence.39 The study strengths are:
National and representative sample of contemporary ACS hospitalisations;
Multicentre design allowing comparative analyses;
Repeated multidimensional validated measures of health-related quality of life and medication adherence profiles;
Efficiency of research data enhancement through bespoke linkages to clinical and administrative electronic healthcare records;
Participant consent to enter future research studies;
Scalability through responsive funding from the NIHR;
Potential for health economic evaluations.
There are, however, a number of limitations. Case ascertainment is not 100% and there is evidence for survivorship bias. However, recruitment of all ACS was not the remit of EMMACE-3. If necessary, more complete case ascertainment of ACS may be estimated through the pooling of multiple secondary and primary care sources of EHRs.39 For the questionnaire data, missingness varied between 2% and 40%, and for MINAP data fields varied between 1% and 10%.
Dissemination
On successful application, study data will be shared with academic collaborators. The findings from EMMACE-3 will be disseminated through peer-reviewed publications, at scientific conferences, the media, and through patient and public involvement.
Acknowledgments
The authors gratefully acknowledge the participation of the EMMACE hospitals, their research staff, principal investigators and the EMMACE study team.
References
Footnotes
Collaborators EMMACE-3 investigators: Basel Hanbali Airedale NHS Foundation Trust, John Davies Basildon and Thurrock University Hospitals NHS Foundation Trust, Ranjit More Blackpool Teaching Hospitals NHS Foundation Trust, Steve Lindsay Bradford Teaching Hospitals NHS Foundation Trust, Piers Clifford Buckinghamshire Healthcare NHS Trust, Tim Reynolds Burton Hospitals NHS Foundation Trust, S Grant Calderdale and Huddersfield NHS Foundation Trust, Justin Cooke Chesterfield Royal Hospital NHS Foundation Trust, Shahid Junejo and Samuel McClure City Hospitals Sunderland NHS Foundation Trust, Mark Scoote Colchester Hospital University NHS Foundation Trust, Mohammed Ahmed El-Harari County Durham and Darlington NHS Foundation Trust, John McDonald East Lancashire Hospitals NHS Trust, Matthew Faircloth Frimley Park Hospital NHS Foundation Trust, Mark Appleby Harrogate and District NHS Foundation Trust, Mohammed Al-Obaidi Heatherwood and Wexham Park Hospitals NHS Foundation Trust, Farqad Almagir Hull and East Yorkshire Hospitals NHS Trust, Simon Hetherington Kettering General Hospital NHS Foundation Trust, Somnath Kumar Lancashire Teaching Hospitals NHS Foundation Trust, CPG Leeds Teaching Hospitals NHS Trust and York Teaching Hospital NHS Foundation Trust, Nicola Brooks Medway NHS Foundation Trust, Ted Lo Mid Staffordshire NHS Foundation Trust, Philip Batin Mid Yorkshire Hospitals NHS Trust, Raj Khiani Milton Keynes Hospital NHS Foundation Trust, Alan Bagnall Newcastle Hospitals NHS Foundation Trust, Roger Moore North Cumbria University Hospitals NHS Trust, Christopher Gibbs Northern Devon Healthcare NHS Trust, Sudipta Chattopadhyay Northern Lincolnshire and Goole Hospitals NHS Foundation Trust, Honey Thomas Northumbria Healthcare NHS Foundation Trust, Jolanta Sobolewska Pennine Acute Hospitals NHS Trust, Dr Jo Porter Peterborough and Stamford Hospitals Trust, Venkatesan Suresh Plymouth Hospitals NHS Trust, Paul Kalra Portsmouth Hospitals NHS Trust, Usman El-Sheikh Royal Devon and Exeter NHS Foundation Trust, Anwar Memon Scarborough and North East Yorkshire Health Care NHS Trust, John Rowley Sherwood Forest Hospitals NHS Foundation Trust, Nigel Capps Shrewsbury and Telford Hospitals NHS Trust, Philip Keeling South Devon Healthcare NHS Foundation Trust, Mark De Belder South Tees Hospitals NHS Foundation Trust, Thuraia Nageh Southend University Hospitals NHS Foundation Trust, Philip Lewis Stockport NHS Foundation Trust, Mark Dayer Taunton and Somerset NHS Foundation Trust, Alan Baonall The Newcastle Upon Tyne Hospitals NHS Foundation Trust, Adrian Brodison University Hospital of Morecambe Bay NHS Foundation Trust, Ian Hudson University Hospitals of Leicester NHS Trust, Francesco Lo Monaco West Middlesex University Hospital NHS Trust, Telal Mudawi Wrightington Wigan and Leigh NHS Foundation Trust.
Contributors CPG led the development of the protocol, organisation and funding. OAA undertook the drafting of the manuscript and data analyses. RGG, RMW, RK and ASH were involved in the design of the study. All authors have read the draft critically to make contributions and approved the final text.
Funding This work was supported by the National Institute for Health Research as part of a Clinician Scientist Award (Reference number: NIHR/CS/009/004).
Competing interests None.
Patient consent Obtained.
Ethics approval Leeds (West) Research Ethics committee (REC reference number: 10/H131374).
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.
Data sharing statement Only pseudonymised data will be released to collaborators.