Article Text

Abstract
Objectives First, to explore parents’ views on and experiences of managing their febrile child and to assess their behaviour and needs when in search of information about fever; second, to develop and evaluate a hospital discharge information package about fever in children.
Design Mixed methods: (A) qualitative study with semistructured interviews and a focus group discussion (FGD) and (B) quantitative survey.
Setting Emergency department, non-acute hospital setting and day nursery in Rotterdam, The Netherlands.
Participants Parents of children <18 years (interviews, n=22) parents of children under 5 years (FGD (n=14), survey (n=38)).
Intervention Information package about fever in children (leaflet and website including videos).
Outcome measures quantitative survey Knowledge of fever and confidence in caring for a febrile child (Likert scale 0–5).
Results Parents found fever mostly alarming, especially high fever. Help-seeking behaviour was based on either specific symptoms or on an undefined intuition. When parents did not feel recognised in their concern or felt criticised, anxiety increased as well as the threshold to seek healthcare for future illnesses. Information was needed, especially for situations when the general practitioner or social network were less easily available. This information should be reliable, consistent, available in multiple formats and include advice on management of fever at home and precise referral to medical services. Parents reported improved knowledge about fever (p<0.05) and mentioned improved confidence in caring for a child with fever at home after consulting the information package.
Conclusion Parents of children with a fever visiting the hospital are concerned about specific symptoms or based on an undefined intuition. Rather than telling parents that they should manage their child’s illness at home, healthcare professionals should recognise parental intuition and provide clear information on alarming signs and potential diagnoses to empower parents in the management of their febrile child.
- paediatrics
- qualitative research
- infectious diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Using two different data collection methods for the qualitative phase of the study provided opportunities to explore parents’ views and needs in depth, resulting in a better understanding of help and information-seeking behaviour when visiting the emergency department.
The combination of (1) development of a hospital discharge information package based on parents’ needs with (2) evaluation of this intervention afterwards enabled refinement of the information package.
Diversity of the participants, in terms of age, education, experience and cultural background, facilitated the assessment of the appropriateness of the information package for a diverse audience.
Participants were fluent in Dutch reading and writing, limiting the applicability of the information package to non-Dutch speaking/reading parents and those with low literacy.
All participants of the focus group were women, a consequence of the open invitation method, limiting applicability to men.
Introduction
Fever in children is the most frequent reason for parents to seek medical attention.1 2 The majority of these children are under 5 years and have a self-limiting disease. In general practice, around 1% have a serious infection; in an emergency department (ED), this is 5%–15%; the most frequent serious infection being pneumonia.3 4 However, the number of ED admissions continues to increase, mostly for minor illness not needing intervention.5 6
The current problem is twofold:
Parents are well capable of identifying their ill child by describing how their child’s illness differs from previous episodes (parental intuition or gut feeling).3 However, this parental concern is non-specific and also present in non-severe illness.7 Potential reasons might be a lack of knowledge about fever and anxiety about potential harmful consequences.8 9
At the same time, there are still children dying of serious infections due to errors or delays in diagnosis.10 As serious infections often cannot be distinguished from self-limiting disease at an early stage, it is important that parents recognise warning signs during the disease course.
In order to reduce unnecessary ED consultations for self-limiting disease but also to prevent parents from missing a seriously ill child, parents need clear hospital discharge advice about managing their febrile child at home. For this advice to be effective, it should fit well with parent’s needs and worries.11 Even though studies have been done in general practice and in well-child clinics,12 13 knowledge on the necessary information about fever for parents visiting the ED is limited.
The aims of the study are to: (A) explore parents‘ views on, and experiences of, managing their febrile child; (B) to assess their behaviour and needs when in search of information about fever; and (C) to develop and evaluate a hospital discharge information package about fever in children.
Methods
Study design
This was a two-stage project, using exploratory theory building methods for stage 1 (development), followed by an intervention and evaluation for feasibility and piloting in stage 2. This methodology follows the Medical Research Council (MRC) framework for development and evaluation of complex interventions.14
Development
A qualitative design was used to explore parents’ views on, and experiences of, fever in children through the use of semistructured interviews. Based on these findings, we developed an information package consisting of a leaflet (online supplementary file 1) and a website (www.sehzorg.nl/koortskinderen (in Dutch)), both of which included a traffic light system to help parents identify the risk of serious illness after hospital discharge. The website also contained informative videos about fever and pneumonia in general and videos illustrating warning and safety signs in febrile children.
Supplementary file 1
Feasibility and piloting
The complete information package was evaluated to assess its feasibility during a focus group discussion (FGD) with parents of children under 5 years. Emerging themes that arose during the development phase were also further explored in the FGD. In addition, a quantitative survey was used to evaluate the information package in a pilot in the acute and non-acute setting.
Sampling and recruitment
Development
We recruited a purposive sample of parents of children under 16 years for the interviews, both in an acute setting (at the ED) and in a non-acute setting (outpatient department or ward), to obtain maximum variation within the sample. All interview participants were recruited in the Erasmus Medical Centre – Sophia Children’s Hospital (EMC-Sophia) and the Maasstad Hospital, Rotterdam, until a point of data saturation was reached. Out of 29 eligible parents, 22 agreed to participate; seven refused for various reasons (no interest or time and language barrier).
Feasibility and piloting
We recruited parents of children under 5 years for the FGD through an open invitation at day nurseries (digitally and by posters on location) in the Rotterdam area through social media of patient organization Kind en Ziekenhuis (K&Z) and EMC-Sophia and an article in a regional newspaper.15 Participants for the quantitative survey were recruited at the ED of the EMC-Sophia through day nurseries and by open invitation on the information website between July and October 2017.
Research team
The core research team (all female) consisted of an MD/PhD student in paediatrics (JvdM), medical students (DvK and AdH) and a consultant in paediatrics (RO (MD, PhD)). JvdM was trained in qualitative methodology, and we shared expertise with an international expert in this research area and methods (ML (MD, PhD)) and with a social scientist from patient organisation K&Z (ES-C).
Data collection
Development
DvK conducted the semistructured interviews between November 2016 and February 2017 in a hospital room with only the researcher and the participant using a flexible interview guide (online supplementary file 2). All interviews were audio recorded. The relatively short duration of 15 min generated sufficient information and facilitated participation since they took place during waiting time in the hospital.
Supplementary file 2
Feasibility and piloting
The FGD was held in February 2017 at an inner city day nursery near the EMC-Sophia. We chose this setting as a more neutral and more natural environment for parents than a medical setting in order to promote open and rich conversation and to reduce the risk of social desirability bias. ES-C and JvdM led the FGD, using a discussion guide including open questions and example cases (online supplementary file 3). RO and DvK had an observer’s role and interacted occasionally if needed. The FGD was audiorecorded and lasted 2 hours. For the quantitative evaluation, we used a survey with questions on: (1) knowledge about fever in children and about caring for febrile child at home (questions 1–3) and about parents’ confidence in their ability to provide adequate care for a febrile child and in their ability to seek medical attention (questions 4–6), referring to the situation before and after consulting the information package.16 In addition, questions were asked about clarity and layout of the information package (online supplementary file 4).
Supplementary file 3
Supplementary file 4
Demographic information was collected from all participants.
Data analysis
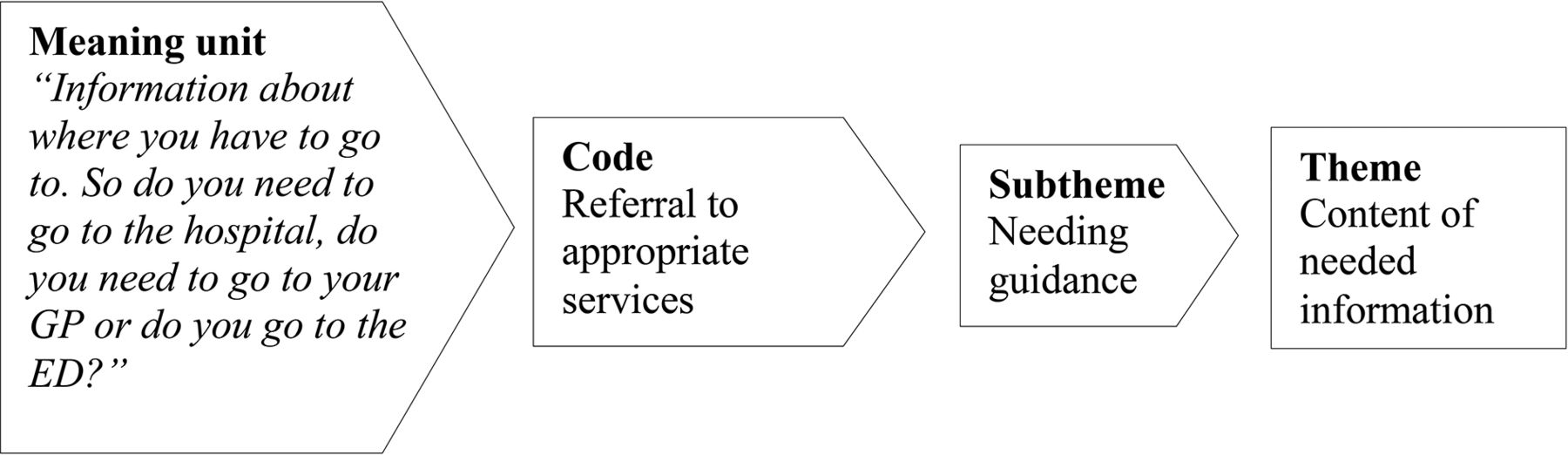
All interviews and the FGD were transcribed verbatim by DvK, including non-verbal information. An interim analysis of 14 interviews guided further exploration of the emerging themes in subsequent interviews. Thematic content analysis was used for all interviews and the FGD, using the qualitative software package Atlas.ti (V.7.5.7).17 18 First, the fully transcribed interview/FGD was read in detail, then meaning units were defined and coded. Initial themes were combined into overarching themes, containing subthemes reflecting their components (figure 1). A pilot of three transcribed interviews and the complete FGD were coded by two authors independently (DvK and JvdM), and final codes and themes were agreed on. The scores on the Likert scale of the quantitative survey were coded from 0 to 5, mean scores were calculated and differences in pre-exposure and postexposure scores were analysed using a paired sample t-test. Statistical code and dataset of the quantitative survey are available as online supplementary files.

Coding process.
Ethics
Written informed consent for the interviews and FGD was obtained from all participants.
Patient and public involvement
This study was performed in close collaboration with ‘Kind en Ziekenhuis’, a patient organisation for children in hospitals, representing the patient’s perspective in study design, protocol development and conduction of the study. We developed and updated the intervention based on parent’s views and needs, as described in this paper. The intervention is publicly available to all end-users.
Results
Participants
A total of 22 semistructured interviews were performed, half in acute setting and half in a non-acute setting (6 men, 16 women). Fourteen women participated in the FGD (13 mothers, 1 aunt). The survey included 38 parents. Baseline characteristics of all participants are presented in table 1. Overall, most participants were female, with a median age between 33 years and 35 years. The participants of the FGD were all female, had less children and younger children than the other participants. There were no differences between participants in the acute or non-acute setting of the interviews and survey, in terms of gender, age and number of children.
Participant characteristics
Development phase
The interviews and FGD results can be divided into three main content areas: (A) views on fever and its treatment, (B) experiences of managing a child with a fever and (C) information seeking. Codes and (sub)themes are reported in online supplementary file 5.
Supplementary file 7
Views on fever and its treatment
Views on (causes of) fever
Most parents believed fever is caused by an infection. Parents with higher levels of education mainly mentioned viruses or bacteria as a cause of infection; those with less formal education were less likely to report the exact cause. Many parents recognised fever as a natural defence mechanism of the body, but it was perceived as both reassuring and alarming: ‘there’s a bacterium in the body that doesn’t belong there and by means of fever, you know, your body tries to destroy the bacterium. (…) But well, if it’s getting too high, you know… I’ve heard stories like: when it’s getting higher than 40, then it’s going to be dangerous’ (father, three children, 5–10 years).
Views on paracetamol and antibiotics
Although with different views, most parents considered paracetamol safe to lower the temperature and relieve discomfort for the child. One mother was worried about its effectiveness when used too often: ‘A slightly increased temperature… you can also give it too soon, I’m talking about high fever. (…) Otherwise they don’t work anymore later on’ (mother, two children, 4–6 years).
Parents had different views on antibiotics, often depending on their own experiences. Most parents mentioned it was indicated ‘only when really needed’ but with different explanations. ‘I think it’s a last choice, like: there’s nothing else, so let’s go for antibiotics’ (mother, one child, 2 years); ‘You [the doctor at the ED] saw his ears, I came urgently by ambulance because he had a febrile fit. Then at least you can give antibiotics!’ (mother, three children, 1–10 years). Two parents mentioned fear for resistance: ‘At a certain time your body just becomes resistant, so if you just keep on taking it…’ (mother, three children, 1–14 years). One parent thought doctors were too conservative in prescribing antibiotics: ‘The whole attitude of waiting too long with antibiotics, I don’t agree with that at all. Not to stuff them with antibiotics immediately, but I think nowadays it is too restrained…’ (mother, two children, 4–5 years).
Experiences of managing a child with a fever
Management of fever at home
Parents mentioned being more alert once they knew their child had a fever: paying extra attention to the child and looking for accompanying symptoms. Most parents try to lower the temperature with paracetamol, but homeopathic medicines were also mentioned, and removal of clothes, cold showers or cold wipes. Parents used paracetamol in various ways: (A) waiting for signs that the child is unwell, ‘I almost never give paracetamol. Because I think: the body has to do it on its own and only if they develop such things as pain… But 9 times out of 10 it just resolves by itself’ (mother, three children, 2–9 years); (B) as soon as there is a fever, ‘Yes, I give paracetamol when there is fever. And then every 6 hours. I try to avoid peaks to help her hopefully a bit’ (mother, one child, 9 months); or (C) based on the child’s preference, ‘We use those suppository things, but he hates them anyway, so…’ (father, two children, 4–6 years).
Help-seeking decisions
Parents decided on seeking medical attention based on their instincts, often difficult to specify: ‘It’s just a feeling. I couldn’t say: one time the fever is less but he looks more ill, while another time he has 39.5 but alert. It is very much just a feeling’ (mother, FGD). ‘It is a sort of gut feeling, you really feel when your child is ill. (…) I cannot describe what it is, but I know there’s something wrong. And then you just want someone to look at him and be reassured’ (mother, FGD). Specific reasons to be alarmed and seek medical attention were young age (not able to express themselves), high fever, long duration of fever and accompanying symptoms like reduced appetite or drowsiness.
Learning about (managing) fever
Many parents mentioned their experience with illness in previous children or in their social background and network as a motivation for their behaviour. ‘It is out of experience and it depends on your personal situation. What family you’re from, what social network you have, if you have any friends… Parents from school whom you can ask questions…’ (mother, five children, 1–8 years). Especially during the FGD, the role of experience was prominent and how it can affect behaviour. One mother: ‘My children have fever very often (…), but at a certain moment you get used to it. You think: I know a paracetamol works in my children, so I give it to him. (…). They have fever so often, it doesn’t surprise me anymore’. Most parents recognised this. However, another mother mentioned a pitfall of relying on reassuring previous experience: ‘sometimes I wait longer with the second child, but then he appears to have a pneumonia and then I think: I should have gone earlier’, and a mother with a first child suffering from febrile fits: ‘Febrile fits run in families, so when I would have a second child with fever, I would be extra stressed out. But that depends on what you’re used to’.
Experiences with healthcare
Parental concern or instinct was often not recognised by healthcare professionals. ‘When your mother feeling says: hey, something is wrong here. Then it is frustrating when a doctor says: no, there’s nothing wrong’ (mother, FGD). Several parents described that when doctors say ‘it’s just a fever’, they give parents the feeling they are not listened to or that they should not have come. ‘As soon as you call the GP, they say: “yes, but fever is normal for a child”. Then I think: you don’t even listen to my story (…), first listen to what I have to say, because I don’t only call because he has a fever!’ (mother, three children, 5–10 years).
In cases of self-limiting disease, some parents said they would be more reassured when the doctor explained which (possibly severe) diseases were excluded, instead of only getting the diagnosis ‘another virus’. These negative experiences increased the threshold for seeking help in the future. ‘Then I thought: yes, but when I call, I will be told “yes mam, the flu is around”. So I didn’t call’ (mother, FGD). Most parents had a good relationship with their own general practitioner and felt no threshold for contacting the GP, but there was a high threshold for contacting the out-of-hours services. ‘He [own GP] takes my child very seriously. (…) The first time he had fever (…) I thought: he is going to die! But the GP always says: it doesn’t matter, if you are worried: call’ (mother, FGD). ‘I find it always a bad experience (…). To go to my own GP, my experience is: hey, he will come, he knows my child. But as soon as you go to the out-of-hours services it becomes difficult. There you have to struggle for an appointment’ (father, two children, 7–8 years).
Information seeking
Information needs
Parents expressed their need for information about fever in children, especially before deciding to seek medical attention. ‘For example in the weekend you cannot call the GP and you don’t call the out-of-hours service when it’s not severe. So then I look it up myself’ (mother, one child, 4 years). When asked when they need information: ‘Especially on Saturday or Sunday, who should you call? Then I think: I won’t call 112 [European emergency number], that’s nonsense. Out-of-hours service maybe, but I find that also difficult. Then there is nobody, besides family, whom you can call’ (mother, FGD).
Some parents wanted more background information on fever, but most parents emphasised the need for clear instructions about what they can and should do at home. ‘Often they only look at dehydration, but I would want to know if she can get something against the cold and the cough’ (mother, three children, 2–9 years); ‘It has to state very clearly: where do you go? First to the out-of-hours GP service, or to the emergency department (…)?’ (father, two children, 2–5 years).
Information sources
Parents reported that the internet was the most commonly used source of information at home but mentioned lack of consistency and reliability as its pitfalls. ‘I always google, but that is not always helpful, because of course you also see very contradictory things’ (mother, three children, 1–14 years). Parents also ask for advice in their social network, like family or peer parents. ‘Parents from school where you can ask things, like “my child has this, did you experience that once?” You know, a network surrounding you matters a lot’ (mother, five children, 1–8 years).
Information delivery preferences
Parents preferred multiple different formats of information: verbal and/or written, on paper and/or online. Most parents preferred verbal information given by a doctor, given the possibility to ask questions. ‘I prefer verbal information. If I don’t understand something, I can ask for clarification’ (mother, three children, 1–10 years). Online information should be clearly reliable. ‘Mostly the information is at those general websites, where you’re overwhelmed with information. I would like the information to be linked to for example a hospital’ (mother, three children, 7 weeks–5 years).
Leaflets could be reread but are often not at hand in the acute situation; written information should also be available digitally, and audio-visual material could be supportive in addition to other means. ‘I think a combination of verbal and written information is best. You read something, but you want it to be confirmed by someone who has professional knowledge. (…) Or maybe with some video support or so’ (father, two children, 7 years).
Feasibility and piloting
Based on the parents’ needs and preferences that we discovered during the development phase and based on the literature, a concept hospital discharge information package was developed: a leaflet (online supplementary file 1) and a website (www.sehzorg.nl/koortskinderen), including a traffic light system for identifying the risk of serious illness. The website also included informative videos about signs and symptoms (www.sehzorg.nl/koortskinderen).
Qualitative evaluation
The parents in the FGD judged this concept package to be clear and comprehensive. They particularly appreciated the traffic light system that included clear instructions about to the severity of symptoms. However, some parents said that reading the alarming signs could raise their anxiety, a feeling not shared by all parents. Also, they expressed the need for a clear statement that whenever they are worried they should be allowed to contact a healthcare professional. The videos of clinical signs and symptoms were judged to be very informative, especially for less experienced parents. Still, they expressed the need for clear instructions concerning what to do when they identified the displayed symptoms in their child. During the FGD, some parents raised their concerns about febrile fits. Even though this concern was new for some parents, all of them agreed they needed information on this issue. For this reason, this was added to the package.
Parents found the combination of the written information, videos and traffic light system most helpful. ‘I just think the combination is great. That there are videos and this leaflet. Because I know for example what retractions are, because I’ve seen it at work, but not everyone knows it. So I think it is good to see it. And with the leaflet to decide whether to do something or not’ (mother, one child, 9 weeks).
Parents said they would be more confident in caring for their children after having read and seen the information. Also, it would empower them in contacting a healthcare professional, as they could support their intuitive worry by mentioning specific signs and symptoms. ‘It makes a clearer impression [on the GP]: “I looked, she’s drinking less, blabla”, then you know these are important things to pay attention to’ (mother, FGD).
Parents recommended that the information should be available in the waiting rooms of general practice, postnatal clinics and on social media.
Quantitative evaluation
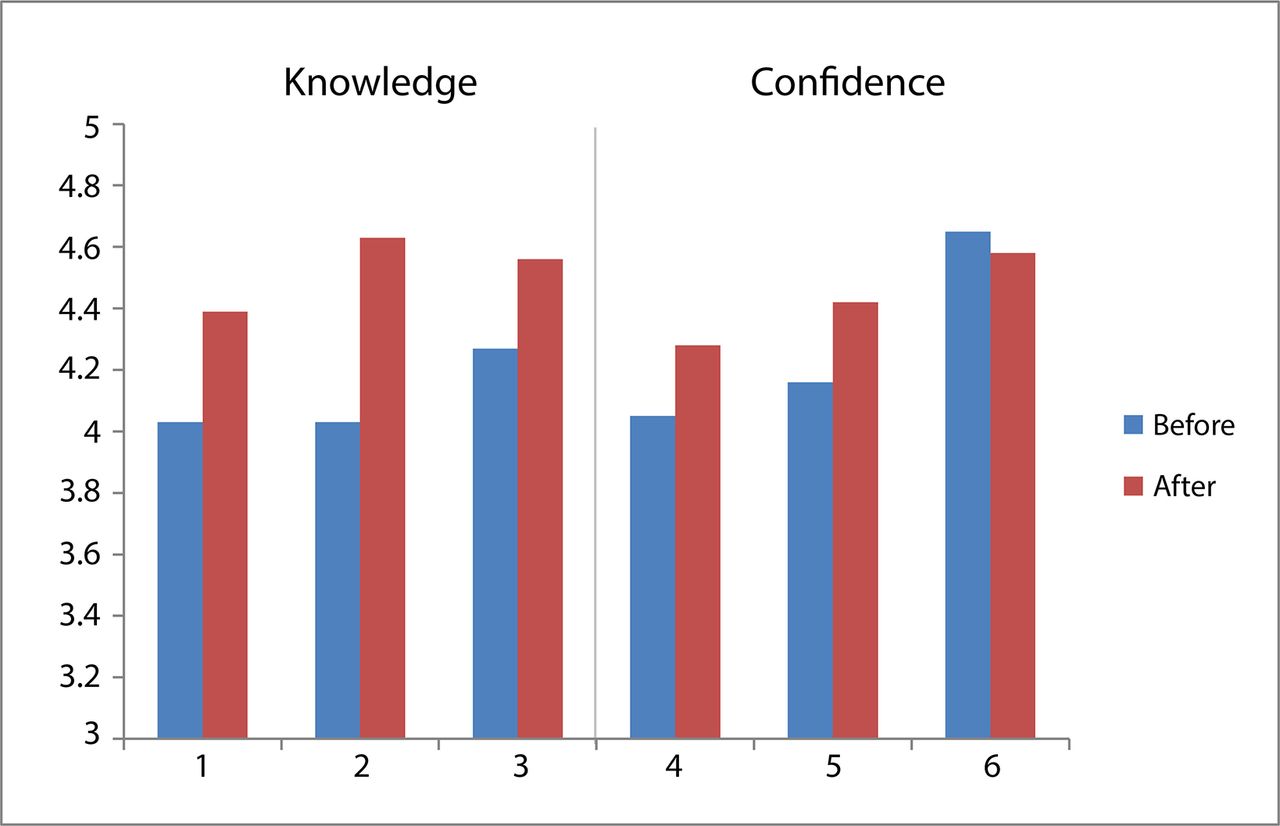
Parents valued the information leaflet as well as the website with videos. Parents valued the information leaflet as well as the website with videos. Mean scores on all items of self-reported knowledge and confidence before and after the information package are presented in figure 2. We observed an increase in both areas of the survey: knowledge about caring for a child with a fever (4.1–4.5 out of 5) and confidence in caring for a child with a fever at home (4.1–4.3) and in help-seeking (4.4–4.5), with significance on the area of knowledge (p<0.05).
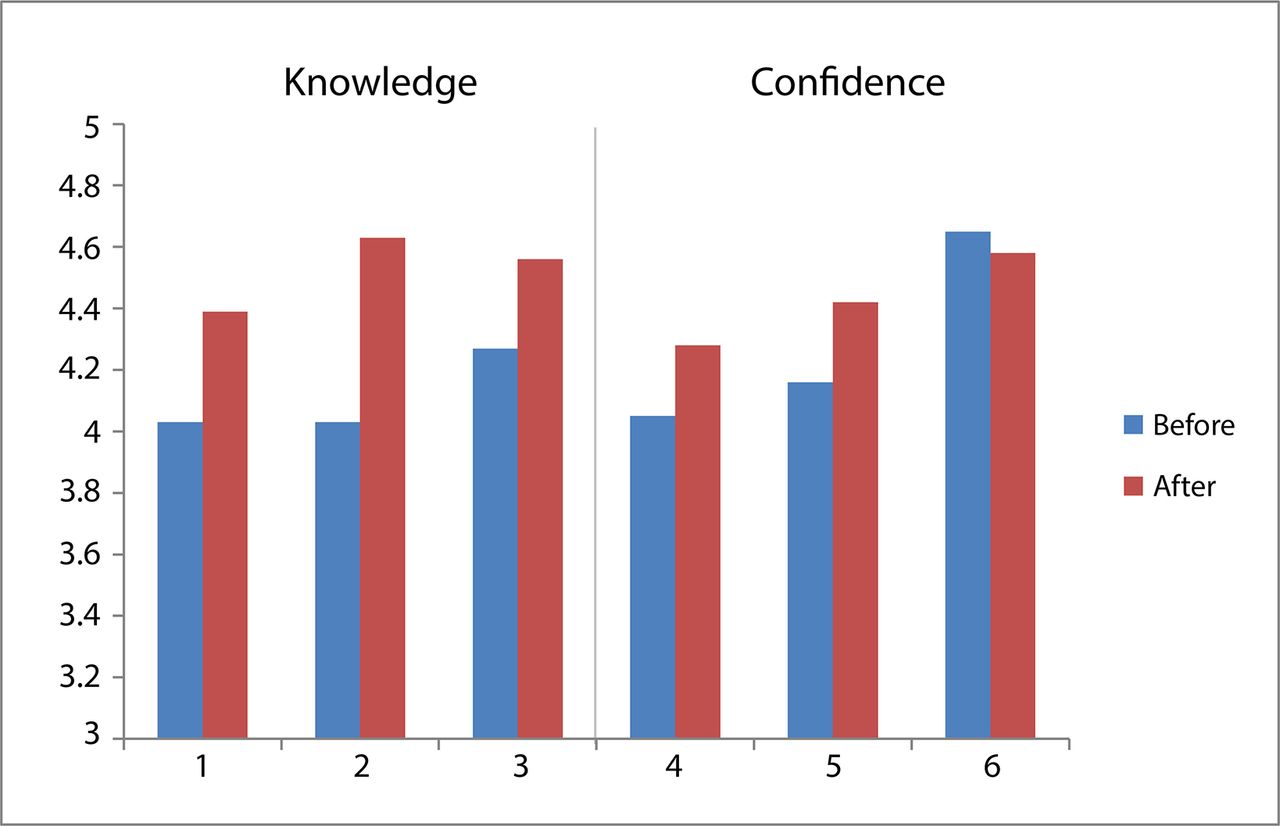
Knowledge and confidence before and after consulting the information package.
Parents gave high scores for layout, comprehensibility of the language, clarity of the message and usefulness of the package (median score 5 out of 5 (IQR 4–5)).
Thematic summary
Summarising our results, we observed that the ability of parents to care for a child with a fever after hospital discharge is influenced by many factors, as visualised in figure 3. These factors can be healthcare related or parent related but have either an empowering or disabling influence on the parent’s ability to care for their child independently. Some factors have a direct influence on parents’ behaviour; other influences are more complex. For example, if a doctor dismisses parents’ concerns by saying ‘it is nothing’ (while meaning that parents can manage this level of illness without seeking help), parents perceive this as criticism that doctors do not consider that the illness warrants medical attention. This perceived criticism increases the barrier for the parent to seek medical attention in the future.

{kind=link}
{kind=link}
{kind=link}
Positive and negative factors influencing parental ability to manage their febrile child. ED, emergency department.
Discussion
Main findings
Our observations in a population of parents of febrile children after hospital discharge suggest that parents in The Netherlands are concerned when their child has a fever, especially when there is a high fever. Paracetamol is perceived as a safe way to treat fever and is used in different ways. Parents preferably do not want antibiotics for their child, as they consider that they should be used ‘only when really necessary’, although the explanation of ‘necessary’ varies. Help-seeking behaviour was often based on an inexplicable parental intuition that ‘something is wrong with the child’, a need for reassurance, or on the presence of specific symptoms like long duration of fever, reduced appetite or drowsiness. Parents often do not feel as though they are taken seriously in their intuition or worry by healthcare professionals and experience a high threshold for contacting healthcare during out-of-hours services.
Interpretation of findings and comparison with the literature
Even though fever was often seen as alarming, we did not find signs of ‘fever phobia’ and overtreatment of fever as has been described in other studies.8 9 19 20
Kai described earlier that help-seeking behaviour is related to the balance between perceived threat of the illness and personal control.21 Also others noted that the ability of parents to manage a child’s illness is influenced by many factors, like experience, social circumstances and expectations, and their own knowledge and health.12 22 A recent review also described the importance of attitudes, beliefs and perceived control on the actual behaviour of seeking healthcare.23 These dynamics are in line with our results as reflected by the balance we presented in figure 3.
Once parents feel the need to seek healthcare, they often describe this as an intuition, which may reflect Van den Bruel’s findings, where parents described their gut feeling as ‘something is different than usual’.24 However, this felt need for help by parents is not always seen as an ‘appropriate’ reason to visit the ED from a healthcare perspective. Ehrich described that not being aware of different meanings and viewpoints of ‘appropriateness’ of a medical consultation can lead to misunderstanding between doctors and parents.25 This might partly explain the mismatch we observed between parents ‘knowing something is wrong’ and doctors ‘saying nothing is wrong’ with the child. We observed that when there is a good relationship with the doctor, he ‘knows the child’ and when parental intuition is taken seriously, parents feel reassured after consultation. However, when they feel criticised, or when the diagnostic process is not explained well, this may increase anxiety and increase the threshold for seeking healthcare in the future (figure 3), as also described by others.26
Weekends or evenings shifts with limited access to the child’s own GP or their social network maybe most sensitive to high thresholds for contacting the out-of-hours services, and at these moments, there is a high need for information. Essential information would be practical advice about management of a child with a fever at home and information about when to seek medical attention and where. Parents prefer information given by healthcare professionals, in addition to clear information in multiple different formats. These findings are consistent with other studies, concluding that parents’ need to be reassured by receiving reliable, consistent information about fever and symptoms.12 13 27 The role of leaflets in improving patient satisfaction after consultation has been reported in general practice.28 29 The need for verbal explanation, supported by written and visual cues, has been reported to be most successful.30
Our information package including a traffic light system with instructions for management at home was deduced from the traffic light system of the National Institute for Health and Care Excellence guideline and appreciated by the parents.1 This system has been used before in information about respiratory tract infections and has proven its added value in informing parents.31
This study was mainly focused on the ED setting, thereby complementary to studies that have been performed in the setting of primary or preventive care. There are several differences between the GP setting and hospital setting, like the a priori risk of serious infection, the diagnostic value of clinical signs and symptoms,32 the clinical experience in assessing young children and the diagnostic process. From a parent’s perspective, visiting the ED is usually a stressful experience, and they mostly encounter a doctor whom they do not know. These factors emphasise even more the importance of ED healthcare professionals winning parent’s trust by taking their concern seriously, clearly explain the diagnostic process and giving information that can be re-consulted after the ED visit.33
Strengths and limitations
The qualitative approach provided the opportunity to explore parents’ views and needs in depth and to gain a better understanding of their help and information seeking behaviour. Through the use of triangulation of methods (interviews and FGD) and due to the flexible design, there was room for exploration of important themes in an open and profound way. Additional to the interviews that were well suited for exploring experiences and ideas of individual parents, the FGD enriched the data through the responses and interaction within a group.34 35 An asset is the diversity of the participants, in terms of age, education, experience (interviews and FGD) and cultural background (interviews). A limitation is that almost all participants were fluent in Dutch reading and writing, limiting the applicability of our conclusions to parents with language barrier or low literacy in our country or generalisation to international settings. A further limitation is that all participants of the FGD were women, a consequence of the open invitation method. However, since women are mostly the primary caregivers in The Netherlands,36 we believe they provided rich information on help-seeking decisions. The open invitation method ensured motivated participants who were involved in the topic and could contribute to the study. To reduce the effect of a possibly intimidating hospital setting, we chose to conduct the FGD in a day nursery. Given the lively and open conversations and the fact that also negative experiences with healthcare professionals were shared, the influence of the medical background of the researchers seems limited. Our quantitative survey was limited in sample size. Also, the difference in knowledge and confidence before and after the information package was self-reported by parents, which has limitations.
Implications for clinical practice and future research
The presented positive healthcare factors from figure 3 should be implemented in clinical practice, in order to empower parents in their capacity to care for a febrile child and to support parents when they are making decisions about seeking help for their child. For healthcare providers, it is essential to build a non-judgemental relationship with parents, so that they feel that they are taken seriously. Recognising parental concern and being open about the diagnostic process (eg, explaining which potentially serious infections are excluded) could add to this. Clear hospital discharge instructions should be supported by information material that can be consulted at home. These recommendations require education of healthcare professionals and the availability of professional and clear information packages. Future research should continue to evaluate and improve information material and assess its impact. Standardised measurement tools should be developed to measure the impact of the information package on healthcare and on parent’s knowledge, skills and confidence. The different ideas and needs of subgroups need further assessment, for example, migrant communities and those with limited literacy. All research should be conducted in collaboration with parents and healthcare professionals.
Conclusion
Parents of children with a fever visiting the ED are concerned about specific symptoms like long duration of fever or reduced appetite of the child or if their parental intuition says that ‘something is wrong with the child’. When they perceive that their concern is not taken seriously by healthcare professionals, they feel criticised, and this experience increases the threshold for future help-seeking. Rather than telling parents that they should manage their child’s illness at home, healthcare professionals should recognise parental intuition and provide clear and reliable information about alarming signs, considered or excluded diagnoses, the management of fever and about available medical services. This information is needed in multiple formats, especially for moments when the doctor or social network are less available for advice. A broad information package (leaflet and website including videos) was produced in collaboration with parents and was found to increase parents’ perceived knowledge about fever and improve their perceived confidence in caring for a child with fever.
Supplementary file 5
Supplementary file 6
Acknowledgments
We would like to thank the parents who participated in the quantitative or qualitative surveys or who attended the focus group discussion for their contribution to this study.
References
Footnotes
Contributors JSvdM supervised the interviews, conducted the focus group discussion (FGD), was responsible for the analyses and the main author of the paper. DvK conducted the interviews, assisted in the focus group discussion, transcribed all interviews and the FGD and assisted in analyses of the qualitative data and writing of the paper. AdH-G was responsible for the data collection and analyses of the quantitative survey. ES-C and HR were responsible for protocol development, preparation and conduction of the FGD. AH was responsible for the production of the website and videos of the information package and editing of the paper. SN had a main contribution to the interpretation of the results and the editing of the paper. ML was responsible for protocol development interpretation of the results and editing of the paper. HAM supervised the protocol development, analyses and writing of the paper. RO was responsible for protocol development and supervised the data collection, analyses and writing of the paper.
Funding This work was supported by Stichting Coolsingel, grant number 485, and by The Netherlands Organization for Health Research and Development (ZonMW), grant number836041001 .
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Ethics approval The Erasmus Medical Centre review board (Rotterdam) considered the study not subject to the Medical Research Involving Human Subjects Act (WMO).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.