Article Text

Abstract
Introduction Prescribing antibiotics is an error-prone activity and one of the more challenging responsibilities for doctors in training. The nature and extent of challenges experienced by them at different stages of the antibiotic prescribing process are not well described, meaning that interventions may not target the most problematic areas.
Objectives Our aim was to explore doctors in training experiences of common problems in the antibiotic prescribing process using cultural–historical activity theory (CHAT). Our research questions were as follows: What are the intended stages in the antibiotic prescribing process? What are the challenges and where in the prescribing process do these occur?
Methods We developed a process model based on how antibiotic prescribing is intended to occur in a ‘typical’ National Health Service hospital in the UK. The model was first informed by literature and refined through consultation with practising healthcare professionals and medical educators. Then, drawing on CHAT, we analysed 33 doctors in training narratives of their antibiotic prescribing experiences to identify and interpret common problems in the process.
Results Our analysis revealed five main disturbances commonly occurring during the antibiotic prescribing process: consultation challenges, lack of continuity, process variation, challenges in patient handover and partial loss of object. Our process model, with 31 stages and multiple practitioners, captures the complexity, inconsistency and unpredictability of the process. The model also highlights ‘hot spots’ in the process, which are the stages that doctors in training are most likely to have difficulty navigating.
Conclusions Our study widens the understanding of doctors in training prescribing experiences and development needs regarding the prescribing process. Our process model, identifying the common disturbances and hot spots in the process, can facilitate the development of antibiotic prescribing activities and the optimal design of interventions to support doctors in training.
- antibiotic prescribing
- trainee doctor
- disturbance
- cultural historical activity theory
- process
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We use innovative methods to demonstrate that, rather than being a clear-cut process, antibiotic prescribing is a highly complex, error-prone activity.
We provide a novel, holistic model locating the most problematic steps in the process.
Our findings can guide interventions to support doctors in training.
Our study only considers hospitalised patients with infections, so cannot inform prophylactic antibiotic use or prescribing in primary care.
We also acknowledge that cultural–historical activity theory provides only one possible lens to the analysis and the interpretation of the antibiotic prescribing process.
Introduction
Prescribing medications is an error-prone activity within healthcare and is one of the more challenging responsibilities for doctors in training once they transition from medical school into clinical practice.1 2 Prescribing errors are common, affecting 7% of medication orders and 50% of hospital admissions,3 although these do not all result in clinical harm.4 Errors in prescribing antimicrobials (of which antibiotics are the major group) are reported to be more common than the prescribing of other medications in hospital inpatients4 and can lead to significant consequences, including drug allergy and the development of antibiotic resistance.5 In 2050, it is predicted that there will be 10 million deaths globally due to antimicrobial resistance and a reduction in Gross Domestic Product of 2.0%–3.5%.6
Traditionally, prescribing has been thought of as an activity undertaken by an individual, with a single prescriber signing off the prescription and taking responsibility for the prescribing decision. However, more recent research highlights the importance of the coworking of doctors in training with pharmacists and consultants in prescribing7 and the significance of multidisciplinary teams in delivering high-quality healthcare.8 9 Research in hospital settings emphasises that many decisions, including prescribing decisions, are made by senior clinicians and are enacted by more junior ones.10 11 In addition, other key groups of healthcare professionals are usually involved in prescribing antibiotics in hospital settings. For example, pharmacists typically check the prescription, nurses typically administer the medication and patients ultimately decide whether to take the medication as prescribed, particularly after they are discharged from the hospital.7 12 13 However, high complexity and historically evolved professional boundaries often challenge the linear proceeding of the intended healthcare processes,14 15 including prescribing processes.16–18 The potential for miscommunication and error is therefore high.
Despite recent research on the challenges experienced by doctors in training when prescribing antibiotics and other medications in hospital settings,1 7 19 20 the nature and extent of the challenges experienced at different stages of the antibiotic prescribing process are still not well differentiated. Research has also shown that integrated care pathways have the potential to provide substantial benefits for patients.21 However, existing guidelines and models do not necessarily serve junior doctors in overcoming the challenges they face during the prescribing process, because challenges often relate to the social and professional contexts in which the work occurs, rather than to the work per se.13 20 This means that interventions to improve antibiotic prescribing practices may not target the most problematic areas, let alone do so in the optimal and sustainable way.22 23
In this qualitative study, therefore, we sought to understand antibiotic prescribing as a holistic process involving multiple professional groups caring for a patient with an infection. To unravel the inherent complexity, we drew on cultural–historical activity theory (CHAT) as a framework.24 It is well-suited for our purposes, given its focus on practices, multiple actors and its belief that disturbances, when collectively revealed (ie, identifying and looking at all the problems together) and dealt with (as in the organisation seeks to address the issues), are potential drivers for change and development.25
CHAT as an analytical lens
CHAT has been used extensively to study workplace learning. In the medical education literature, a growing number of studies have applied CHAT to research into medical student and junior doctors’ learning.26–30 In activity-theoretical studies, the analytical focus is on multiple organisational activity systems, in other words, professional groups with their specific objects of activity, artefacts/tools, rules, communities and the division of labour between these.31 This perspective is particularly helpful when considering prescribing processes within hospitals, which are large, multifaceted and complex organisations, and where the objects, rules, community and division of labour (see online appendix 1) are often profession specific, unclear, implicit and/or fluctuating.14 29 Activity systems (eg, of doctors, pharmacists and nurses) within organisations, such as hospitals, are interdependent and at the same time in tension-laden relationships with each other, generating disturbances: A disturbance stands for deviations from the normal scripted course of events in the work process, normal being defined by plans, explicit rules and instructions, or tacitly assumed traditions. It may occur between people and their instruments (eg, care pathway guidelines), or between two or more people. Disturbances can appear in the form of a tension, obstacle, difficulty, failure, disagreement or conflict.32
Supplemental material
In our study, the concept of disturbance will be used to explore antibiotic prescribing processes, presented as a patient’s antibiotic pathway in a hospital setting. The disturbances in care processes may hinder holistic management of patient care.29 However, instead of being viewed as error-causing phenomena, we view disturbances as an inherent feature of work processes and as drivers for change and development.33 34
The CHAT based concept of object,33–35 with its special focus on the ‘misalignment’ of multiple, often competing objects in organisations,29 can widen our understanding of why disturbances take place in antibiotic prescribing processes. For example, for a junior doctor, the specific object may be learning to conduct a prescribing-relevant task, such as writing up a drug chart while simultaneously developing as a physician, and trying to please more senior doctors in the medical hierarchy.20 The flexible aligning of different, competing objects calls for the collective reflection, negotiation and reconceptualisation of the object to enhance collaboration in the provision of patient care.29
Methods
Objectives
Our aim was to explore doctors in training experiences of common problems in the antibiotic prescribing process using CHAT. Our research questions were as follows: What are the intended stages in the antibiotic prescribing process? What are the challenges and where in the prescribing process do these occur?
Study context
Our study involved two ‘typical’ National Health Service (NHS) hospitals, one in England and one in Scotland. Both hospitals had an overarching antibiotic policy aligned to national guidance,36 but specific treatment guidelines vary by medical specialty as a result of differing types and sites of infection. The qualitative data analysed were narratives from 33 junior doctors in their first or second year after graduating from medical school, at a stage of training called foundation year (FY) 1 or 2 in the UK. Prior to graduation, as medical students, they would have received teaching sessions, learning opportunities and assessments relating to diagnosing and managing patients with infections, including choice of antibiotics and their underpinning modes of action. However, as undergraduates, they would not have been able to prescribe antibiotics independently.
Data sources
First, in May 2017, using PubMed, Google Scholar and Google, we conducted a brief search on antibiotic prescribing, with no date restrictions to try to locate any existing antibiotic prescribing ‘process maps’. Second, we analysed existing narrative interview data1 that explored the antibiotic prescribing experiences of doctors in training overseeing the care of patients with infections in two NHS hospitals. The 33 doctors in training were interviewed once, and they engaged in 20 interviews (14 individual and 6 group interviews), arranged according to individual preferences and availability. Participants were recruited by email via deanery circulation lists, through posters and verbal presentations at educational sessions and through a snowballing approach.
Interviews were semistructured and began with an orienting question: ‘What is your understanding of antimicrobial prescribing?’ Following this, a narrative interviewing approach was used to explore FY doctors’ prescribing experiences. Participants were free to choose their own examples to discuss as a result of the narrative interview approach. Note that we did not ask questions that related to particular parts of the prescribing process. No questions were asked specifically about disturbances to the prescribing process. At the end of the interviews, the interviewer asked about the educational needs of FY doctors during their transition to clinical practice.
Consent was obtained from all the interviewees and data were anonymised. Interviews usually took place at the medical schools and ranged from 26 to 82 min (mean 58 min). The 20 interviews (approximately 19 hours 20 min of audio data) were transcribed verbatim. Further information relating to these interviews can be found in the primary publication,1 which was focused on the individual prescribing experiences of FY doctors, the current paper using CHAT as a way of analysing system-level disturbances in the prescribing process. Research ethics approval was granted by both medical schools.
Patient and public involvement
Given the focus on junior doctors’ prescribing experiences for the original study on which this secondary analysis was based, patients and the public were not involved in the design, data collection or data analysis.
Data analysis
Data analysis comprised four stages, outlined below.
Developing the antibiotic prescribing process model
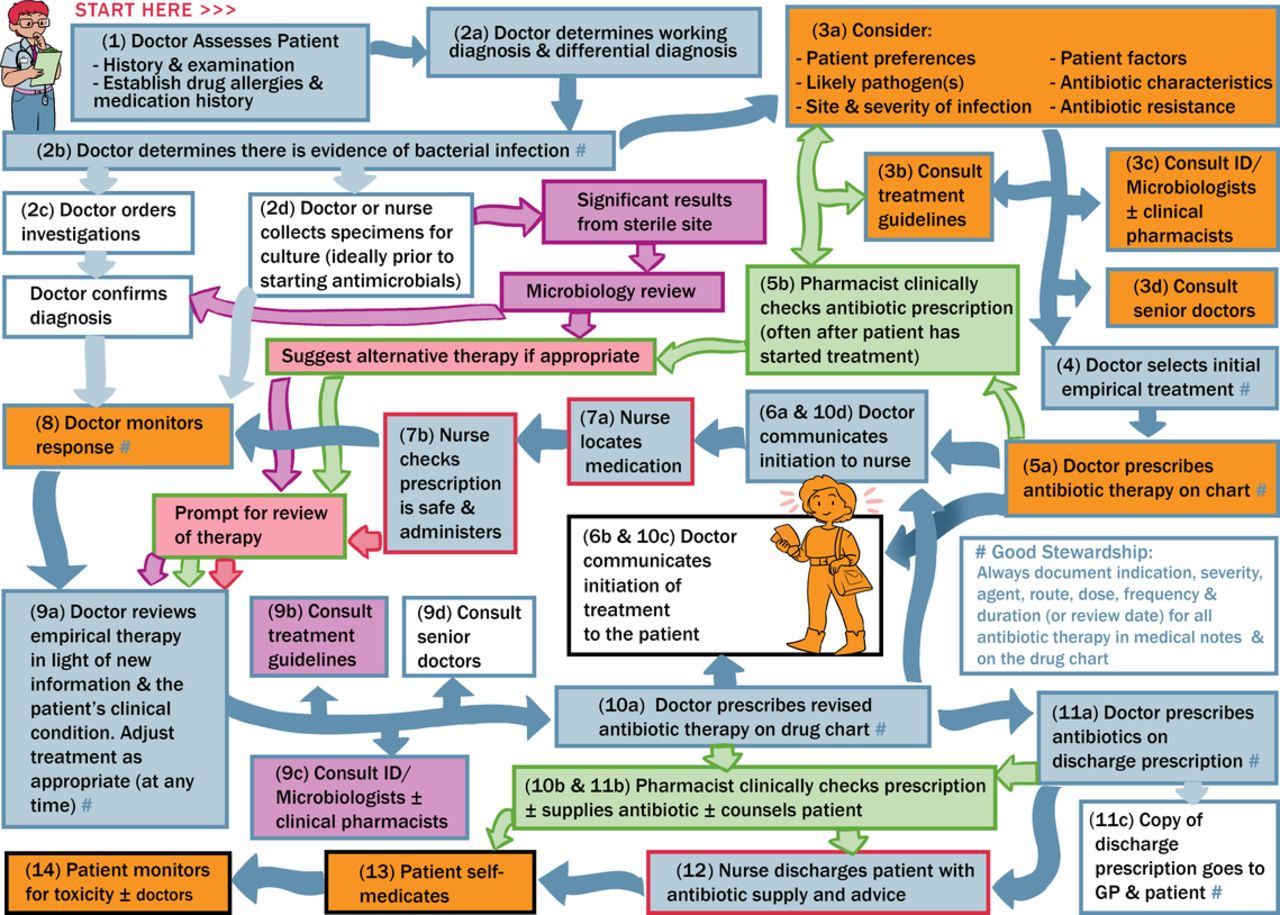
The antibiotic prescribing process maps that we discovered from brief searches using PubMed, Google Scholar and Google images did not fulfil our requirement for a process model depicting the stages of antibiotic prescribing expected to occur in a typical NHS hospital. Consequently, we started to develop our own model informed by national antibiotic prescribing guidance36 37 and first-hand practice and research experience (eg, author 3 is an NHS antibiotic pharmacist). We then showed our model to hospital healthcare workers (two doctors and one pharmacist; see Acknowledgements) and two medical educators (authors of this paper) who agreed that the model reflected the antimicrobial prescribing process as it is intended in a typical NHS hospital. We then commissioned an artist to present the model visually (presented in figure 1). This process model formed the starting point for data analysis, but our understanding of the process continued to develop throughout the analytic process.

Model of the intended antibiotic prescribing process in UK hospitals. Dark blue arrows show the patient journey. Other arrow and box border colours relate to the professionals most commonly providing the input: green, pharmacy; purple, microbiology; red, nursing; pink, microbiologists, pharmacists and nurses. Black box borders represent the patient. Pale blue arrows represent ideal practice.
Mapping of the narratives
We first identified 173 narratives relating to antibiotic prescribing within the 20 transcripts, where events were recounted as stories. Most of the narratives related to times when doctors in training narrated specific events, which we refer to as personal incident narratives (PINs); a minority related to generalised incident narratives (GINs), when multiple events tended to blur into a more generalised story. Data sitting outside the narratives were excluded since they typically did not relate to participants’ actual experiences of prescribing. Each narrative was then mapped to one or more stages in the process model. Individual narratives varied substantially in their length, richness and degree of focus on a particular stage in the process model, with some narratives referring only to one stage and others referring to multiple stages. The presence or the absence of reference to each model stage for each narrative was coded in an Excel spreadsheet. Two of the authors of this paper who were part of the previous study1 undertook the analysis to protect participant confidentiality and to ensure a deep understanding of the research context.38 39 Although two hospitals were under study, we did not look for differences between the two since previous work concluded that there was more variation between wards within a single hospital than between hospitals.1
Identifying disturbances in the process
Then, drawing from the CHAT concept of disturbance,24 32 we identified deviations (ie, tensions, obstacles, difficulties, failures, disagreements or conflicts) from the intended antibiotic prescribing processes from the doctors in training narratives. We wanted to see when, where, how and why processes ‘as narrated’ differed from the processes portrayed by the model and what types of disturbances took place, given the messy realities of complex practice. As the analysis progressed, we were able to form categories of groups of disturbances. Through discussion among all authors of this paper, consensus was reached around five main categories of disturbance, which can be considered as ‘themes’ that were identified qualitatively, and which partially overlapped and interacted.
Locating disturbances as ’hot spots' on the process model
Having mapped the narratives against the process model and identified five categories of disturbances, we then highlighted parts of the model (figure 1) in orange to emphasise that the deviations from the intended processes are most likely to occur—so called hot spots (presented in figure 2). The hot spots correspond to the process stages that were most frequently narrated and/or those where disturbances were articulated by the junior doctors.
{kind=link}
{kind=link}
This is the model of antibiotic prescribing in hospitals but with the particularly problematic components (as identified by junior doctors) shown in orange. These were parts of the process mentioned in ≥25% of the narratives analysed and/or one of the five frequently narrated categories of disturbance.
Findings
Process model
The process model developed (see figure 1) depicts, holistically, the multistage antibiotic prescribing process with 31 stages and multiple practitioners in a typical NHS hospital. It starts with the admission to the hospital of a patient with an infection, moving to diagnosis, through antibiotic treatment and review in the hospital, to discharge from the hospital with antibiotics. It highlights the involvement of multiple professional groups, in other words, ‘activity systems’ of junior and senior doctors, pharmacists and nurses. Numerous ‘checks’ are provided by multiple professionals at different stages, both prior to and after antibiotic therapy has been prescribed and administered. Antibiotic treatment should be reviewed after 24–72 hours or as more information comes to light (eg, culture results or a change in the patient’s clinical condition), which provides further complexity. Doctors are the most frequent prescribers. Nurses usually administer medications, providing checks, such as confirming the patient’s allergy status. Both are often involved with specimen retrieval/collection. Clinical pharmacists usually check the appropriateness of the treatment choice based on guidelines and patient parameters, ensure therapy is physically available, and support the discharge process. All professional groups communicate with and monitor the patient, which may prompt a review of therapy. For example, once a patient is eating and drinking, the nurse or the pharmacist may ask for a review of intravenous therapy (as the patient may be ready for oral treatment). Microbiologists may also request a review of treatment (or review it themselves) in the event of positive cultures, particularly from sterile sites (eg, blood). A detailed description of each process stage and the types of healthcare professional typically involved in them are provided as online appendix 2.
Mapping of narratives
Most doctors in training narratives referred to more than one stage in the process model (median of 3 out of 31 possible stages, minimum of 0, maximum of 12, IQR of 2–5). An example narrative is provided in box 1. This narrative was chosen because it is a ‘rich but concise’ narrative that articulates several model stages, as well as two disturbance categories (see below). The percentage of narratives referring to each model stage ranged from 0% to 36%. ‘Considerations and consultation’ (stage 3) was mentioned the most frequently by far, with ‘consultation’ representing three quarters of the mentions for this stage. ‘Prescribing and checks’ (stage 5) was mentioned next most frequently, followed by ‘monitoring response’ (stage 9). Other model stages received little attention in the narratives, for example, tasks undertaken by non-medics, the discharge process and the arrangements for patients’ monitoring after leaving the hospital. We anticipate that model stages referred to frequently are those that were most memorable to our trainee doctor participants, for example, because they were inherently challenging in some way. Conversely, low levels of attention might indicate unproblematic model stages or those of least interest to them, perhaps because they were not involved in these. This could be because participants did not regard these things as part of the prescribing process, or they overlooked their potential role. They may, for example, regard discharging a patient as something separate, even though it involves prescribing an antibiotic for the patient to take at home.
Exemplar narrative, which refers to multiple stages of the process model, highlighted in square brackets.
E1M3: I can think of an incident which happened more recently which was a male on … one of the colorectal wards. He is fairly elderly, fairly frail and he needed an operation and would have been treated for an infection prior to that, related to the underlying problem which was … basically a fistula connecting the colon and the bladder so he was getting a lot of waterworks infections so he was on antibiotics for that. He had the operation and needed to go to intensive care after, came back and developed a hospital-acquired pneumonia… I think clinically he looked better, biochemically his markers information his white blood cells and such were going up. So he was he had his antibiotics changed over a night on a weekend to something which the person who did the prescribing felt was the next step up in the kind of antibiotic regime [stages 8, 9a, 10a] but actually wasn’t it was a step down from where he was and so he actually got worse over the weekend and then had to be changed back again onto the antibiotic he had originally started on [stages 8, 9a, 10a] and obviously there was a lack of clarity and purpose and such with relation to the prescribing of those antibiotics. That was just a patient I happened to be looking after I wasn’t involved with the prescribing as such.
Interviewer: So, who did the prescribing?
E1M3: So, the original prescription would have been someone on my team so whether I don’t remember whether it was myself or my other colleague or the SHO (senior house officer) or potentially even the registrar. The switch in antibiotics was done by the house officer on call at night over a weekend so there was no, there was no one to really check with (such as an infection expert) as to whether this was the right thing [stage 9 c, disturbance category 3].
Interviewer: So, it wasn’t one of the original team somebody changed it? …
E1M3: I think they felt that, we have these cards [stage 9b] and they felt that they were moving up a level in terms of the treatment for hospital acquired pneumonia but weren’t they were moving down a level. It wasn’t that the antibiotic was wrong in the context of this is a hospital acquired pneumonia it’s moderate to severe because the antibiotic they had chosen was correct however he had already been on the antibiotic for hospital acquired pneumonia graded severe and so it really needed it was a kind of it was the kind of thing that needed discussion with microbiology if it was felt that he wasn’t responding that’s what our microbiologists are here for unfortunately they are not on call out of hours and they are difficult to get hold of over a weekend [disturbance category 3].
Interviewer: Okay so how did that feel? I mean, what did you take from that? How did it feel when this was…
E1M3: It was obviously a slightly difficult situation for the person involved feeling that they needed to do something not having the support that they probably needed to make the decisions and then you know the patient came out the other side of it more unwell so you know that was disappointing from my point of view you a patient who had been with us for some time so you grow quite fond of them and it was just such a shame that he’d you know he’d gone backwards rather than continuing to improve.
Interviewer: What about now, I mean what was the outcome for him eventually?
E1M3: I think he’s made a reasonable recovery overall considering it was quite a big procedure that they had complicated with his stay on intensive care and various infections that he had but I don’t know I was away on nights last week err or the week before I haven’t been in for a week or two now so I didn’t see him on the ward so I presume he’s now gone home [disturbance category 2] certainly the end of that week he was looking a lot better so.
Disturbances in the antibiotic prescribing process
The doctors in training narratives provide rich insights into their prescribing experiences, from the perspective of those working within the process rather than designing it. They revealed occasions when processes differed from the intended ones outlined by the process model (see figure 1). Five categories of frequently narrated disturbances were identified. Illustrative quotes are presented below, with gender and stage of training provided to contextualise the data.
Consultation challenges
The most commonly narrated disturbance was the difficulties in consulting multiple individuals, who were usually more senior doctors (eg, ward-based consultants and consultant microbiologists), and/or information sources prior to prescribing an antibiotic. This was particularly evident in relation to stages 3c and 3d, but to some extent in stages 3a and 3b (shaded orange in figure 2) and frequently related to the medical hierarchy. In the following quote, the junior doctor explains the uncomfortable situation created when ward-based consultants propose a course of action different from their own judgement or that of another person (eg, consultant microbiologist or antibiotic pharmacist):
I think it’s horrifically awkward because as the junior, you are often … stuck in the middle, because, if your consultant is telling you one thing, it’s quite difficult to go against your consultant, especially if it’s going to be bloomin’ obvious that you’ve gone against your consultant, ‘cos they are going to look on the drug chart and see that [they] weren’t getting what they asked for (Female, FY 2 doctor, Location 1, Number 5).
This example depicts how the central role of the senior doctor creates a tension in the attempt to meet the needs of doctors in training developing their expertise during the care process of a patient. In this situation, the tendency is for the opinion of the ward-based consultant, who has ultimate responsibility for the patient and is the direct supervisor for the junior doctor, to prevail. This example demonstrates how a consultation, with its aim of promoting patient-centred prescribing and care, can be challenged by the hierarchy-specific division of labour in which the junior doctor has to follow the tasks and instructions of the senior.
Lack of continuity
A second commonly narrated disturbance was the lack of continuity of care when the patient is transferred (ie, physically moves) from one care provider to the next during the stages of the prescribing process. This was particularly evident in relation to stages 13 and 14 (see figure 2, shaded in orange) and exacerbated by the frequent transfer of patients between wards within the hospitals and shift work. The doctors in training often lacked awareness of what ultimately happened to the patient, whether the antibiotic they prescribed had helped and whether it was the most appropriate choice for the patient. They had to be proactive to find out what happened to patients who moved wards or were discharged from the hospital, and this is challenging in a busy work environment, with long patient care pathways and shift working:
… when you prescribe something and then you don’t necessarily follow the patients up and you don’t receive feedback on whether you prescribed something appropriately or not. I think that’s one of the struggles because the patients come in, you see them, you go home and they’ve gone to the next ward by the following day and you are never really sure if, well I feel I am not sure if I’ve actually prescribed something appropriately sometimes (Female, FY 2 doctor, Location 1, Number 1).
In this example, we witness that as well as lacking patient outcome information, doctors in training do not always receive feedback on their prescribing decision-making process. The quote above also highlights that the provision of care takes place in multiple locations and is fragmented across multiple professional groups, adding to the complexity.
Process variation
The third commonly narrated disturbance was that the prescribing process varied when working ‘out-of-hours’ (ie, at night and at the weekend) or on different wards. This was evident with regard to the prescribing process as a whole (represented as an orange box around the whole of figure 2). This inconsistency created unpredictability, confusion, lack of confidence and fear of making mistakes among the doctors in training. Hierarchies and power relations added to the complexity as help-seeking was often experienced as problematic due to junior doctors’ lower status. In the following quote, we hear how the threshold for prescribing antibiotics was perceived to be different when working out-of-hours. This may be because doctors feel safer giving an antibiotic than not and are responding to a perceived need to err on the side of caution when working with patients or in settings that are less familiar to them, or when support and advice is less available:
I think that overnight, and over the weekends in particular, people [patients] will get given antibiotics more readily. I think that there is generally a thing of safety, it’s better for someone to be on an antibiotic than off them and I’ve seen cases where SHOs [junior doctors] will willy-nilly prescribe antibiotics without necessarily looking directly at the patient (Male, FY 1 doctor, Location 1, Number 2).
This quote highlights the challenges of working out-of-hours and shows how doctors in training perceive prescribing decisions to be different at these times. The otherwise quite strict, profession-specific and hierarchical division of labour seems to become unclear, implicit and/or fluctuating out-of-hours. The example also points to a lack of overall management of the prescribing process across time, such as from the daytime to out-of-hours. The well-framed strategies that are used by distinct activity systems (professional groups), such as the antibiotic guidelines, may not work as flexible tools for depicting the stages.
Challenges of patient handover
The fourth commonly narrated disturbance was the tangible problem of coordination of care. As in the previous category, this disturbance concerned the prescribing process as a whole (see orange box around the whole of figure 2). The most common example of this was difficulties in the handover of care between healthcare professions (eg, the day team to the night team), both within the medical profession and between professions. Such handovers mostly happened verbally, although there were some positive stories of when tools (eg, email handovers) had helped. This category overlapped with the third category already discussed, in that this often related to differences between working in-hours and out-of-hours, but the focus here is different. Disturbances in this category related to poor information flows as expressed in the following quote:
… in the hospital the policy is essentially that if you have got the responsibility of looking up the blood result then you should be prescribing it [the gentamicin] and there were quite a few incidences in my second job when I was on general surgery, well, when I was on the acute surgical receiving ward, where the person on nights didn’t chase up the blood results, and therefore they didn’t write up for the next dose of the gentamicin, and it was only picked up accidentally, or sort of incidentally, or by the pharmacist that they had had one dose and no more doses had been given (Female, FY 1 doctor, Location 2, Number 1).
The quote above highlights the specific challenges for prescribing antibiotics and, in particular, gentamicin and vancomycin, which require therapeutic drug monitoring and dose adjustment based on the levels to avoid toxicity. This example demonstrates an urgent need for healthcare professionals to coordinate their practices to achieve the desired outcomes (relating to handovers in the prescribing activity). Despite some positive stories of functional tools mediating the communication in specific parts of the process, a need for system-level tools that would improve the communication between participants, for example, between doctors working in and out of hours), was depicted.
Partial loss of the common object
The final commonly narrated disturbance was what is called ‘partial loss of object’ in activity theoretical terms, referring also to the misalignment of the objects held by the medical professional treating a patient who is subjected to the prescribing process (see the patient icon shaded in orange in figure 2). In other words, rather than the focus of the prescribing process always being on patient care, the several professional groups involved were often preoccupied with other specific, well-framed goals designated to them within the process, and the patient did not always seem to be the foremost consideration. For example, the following quote depicts the contradiction junior doctors typically said they face in training: while they are highly dependent on supervision and advice from more senior medical professionals involved in the prescribing process, they are often expected to manage the complexity alone, without sufficient support and functional tools. This contradiction diverts doctors in training attention away from the object of the activity, that is, the patient:
Yeah, so obviously I mean F1s [first year junior doctors] by day they are, you know, they, we don’t make a whole lot of independent choices I would say and, really our job is to collect tasks and make sure they are completed and then suddenly at night, everyone disappears, and we’re expected to charge around, and you know display a whole amount of extra knowledge and autonomy. So, it’s an interesting contrast, and it’s, when you first go on nights it’s very daunting, and suddenly you make these decisions, including the decisions about antibiotics, but that’s just how it is that’s the way it goes (Male, FY 1 doctor, Location 1, Number 1).
This quote is a prime example of how, in the multiorganisational field of healthcare, the historically established division of labour and the distinct objects between healthcare professions and medical specialties define the doctors in training specific positions and tasks. It also demonstrates how this junior doctor saw the object of their prescribing activity as primarily about collecting and completing discrete tasks, and trying to avoid mistakes and negative feedback, by carefully following orders given to them by their senior colleagues.
To sum up, all the disturbance categories reported in our study call for interventions to support doctors in training. These could be organisational change efforts to clarify the division of labour and the distinct objects of the professional groups within the organisation.
Hot spots on the process model
The analysis of the narratives and disturbances (identified from the narratives using CHAT analysis of narrated disturbances) against the process model allowed us to locate hot spots, referring to the stages that doctors in training are most likely to have difficulty navigating, marked in orange on a revised model (figure 2). As mentioned, we anticipate that the frequently mentioned model stages are the more memorable ones, which may indicate that they are experienced as particularly challenging by the doctors in training. Similarly, the model stages described as deviating from the intended process are also likely experienced as problematic. The hot spots highlighted in orange in figure 2 were mentioned in ≥25% narratives analysed (stages 3a, 3b, 3c, 3d, 5a and 8) and/or were one of the five categories of disturbance: consultation challenges (stages 3a, 3b, 3c and 3d); lack of continuity of care (stages 13 and 14); process variation (an orange box around the whole of figure 2); challenges of patient handover (an orange box around the whole of figure 2) and partial loss of the common object of the prescribing process (patient icon shaded orange).
Discussion and conclusions
This study, in which CHAT was employed, aimed to explore doctors in training experiences of common problems in the antibiotic prescribing process. Our analysis makes three original contributions to research on the processes of prescribing of antibiotics and to activity theoretical studies in medical education. First, it offers a novel, holistic model identifying the different intended stages of the antibiotic prescribing process. Second, it expands current understandings of the complex and disturbance-laden prescribing process, which may be impossible to predict fully. Finally, by locating the hot spots in the process, the study can inform future interventions to target the development of the most problematic areas in the prescribing process.
Our first finding was that while prescribing is complex (with 31 stages and involving multiple practitioners), doctors in training typically described relatively few stages in each prescribing narrative. Other research has similarly depicted the complexity of antibiotic prescribing processes. For example, Papoutsi et al 20 depicted the social and professional influences that determine antibiotic prescribing behaviours among doctors in training and highlighted the complexity that results from difficult judgements being made by a team of healthcare professionals in a fast-moving clinical environment. However, we are not aware of any previous research that has analysed this prescribing complexity from a doctors in training perspective along a patient pathway.
Our study also highlights which parts of the process were the most difficult for doctors in training, as indicated by how frequently they referred to them in their antibiotic prescribing narratives. By unravelling and locating the commonly narrated disturbances and the hot spots in the prescribing process, our findings add to recent studies that highlight the pivotal role of multidisciplinary teams in delivering high-quality healthcare.7 13 The disturbances and the hot spots in our study may be turned into drivers for change and the development of prescribing processes and optimal design of interventions to support doctors in training.
In terms of the disturbances between junior and senior doctors in the consultation stages of prescribing, these were commonplace in our data and often involved infection experts and/or more senior ward-based doctors across multiple consultations. The result was conflicting advice that was difficult to resolve, causing anguish to doctors in training and often creating tension, which may detract from patient-centred prescribing and care. Such consultation challenges in relation to prescribing medications have been described previously.1 15 20 One might wonder why the doctors in training did not ask for further clarification from their consultants, but from our dataset, it is clear that the medical hierarchy and the locally adopted prescribing etiquette can pose considerable barriers to communication, consistent with previous research.13 15 40
The disturbances around doctors in training reporting a lack of continuity of the prescribing process and care, whereby they appeared to have little insight into patient outcomes, represent a very concerning finding, particularly when combined with the dearth of feedback on prescribing practices reported in this study and elsewhere.41 It is hard to see how doctors in training can develop their expertise and act efficiently in multidisciplinary teams without such information.
In terms of process variation, our study shows how doctors in training experience care processes when working at different times or places, out-of-hours or on different wards. This suggests a need for the development of more functional management strategies and practice-oriented tools to support doctors in training when transitioning between settings and beginning to work more independently.2 With respect to the disturbances around the uncoordinated character of care (such as situations of patient handover), whereby information is shared and tasks are transferred between healthcare teams at the end of a shift, problems have also been reported elsewhere.42
Finally, regarding the disturbances around the partial loss of the common object of the prescribing activity, our study has highlighted the several, distinct activity systems involved in the antibiotic prescribing process, pursuing their specific and often misaligned ‘objects of care activity’.29 This disturbance category illustrates how the object of activity can be perceived and acted on differently by different stakeholders involved in prescribing, meaning that patients can seem neglected, at least as reported in the trainee doctor narratives here. The existence of these distinct objects and their misalignment in the prescribing activity29 provide insights into how and why disturbances emerge, which in turn provides clues as to how they might be resolved and turned into drivers for change and the development of the collective prescribing activity. Our process model for antibiotic prescribing offers one potentially powerful mediator and a tool for multiple professional groups, such as doctors in training, senior doctors, pharmacists and nurses to reflect on their practices towards patient-centred prescribing. The partial loss of a common object might be resolved by implementing activity theoretical interventions (Change Laboratories). These have been used successfully by researchers internationally to transform healthcare, for example, through adaptations of care pathways and new forms of service delivery arising from them.30 43
Methodological strengths and challenges
Our study has several strengths, including the development of the process model, mapping of narratives and in-depth analysis using an activity-theoretical framework.24 32 CHAT allowed us to analyse the disturbances and hot spots throughout the whole prescribing process, viewing them as potential drivers for change and development, an issue rarely highlighted in previous studies. The process model was developed through a literature review and our own knowledge and experience, supplemented with consultations with medical practitioners to increase the credibility and authenticity. Our model, which includes multiple actors and objects, provides a holistic view of the complexity and multidimensionality of the antibiotic prescribing process. Moreover, our findings may inform other medication prescribing processes and their development more broadly.
Our study also has some challenges. It only considers hospitalised patients with infections, so cannot inform prophylactic antibiotic use or prescribing in primary care. Many activity-theoretical studies investigate work processes and workplace interactions by carrying out lengthy participatory observations, together with interviews within the analysed context. Unfortunately, we did not have enough resources to collect new data from multiple participant groups (eg, nurses, pharmacists and patients), and to incorporate observation, we rely on narrative interview data from 33 participants. Furthermore, narratives are accounts of experiences by interviewees that may or may not map onto what actually happened.44 We also acknowledge that CHAT provides only one possible lens to the analysis and the interpretation of the prescribing process.
Implications for policy and practice
From this analysis, communication and information flows seem to be the highest priorities for targeting interventions since they are highlighted through both approaches (ie, frequently narrated stages and themes identified as a category of disturbance). Indeed, previous research has explored ways to improve the situation, for example, through communication strategies and other educational interventions.30 42 45 46
Greater scrutiny of prescribing processes by applying process models such as ours will also be beneficial to future prescribing policy and practice. Indeed, due to the high complexity and multiple types of disturbances involved, the development of the prescribing processes will require continuous, collective efforts over time. We suggest that instead of viewing disturbances as error-causing and harmful phenomena, they need to be seen as important tools towards rethinking and developing care processes. To develop practice, real patient cases (including disturbances) need to be discussed among senior and junior clinicians and other key groups of healthcare professionals and researchers. Our process model can aid in stimulating these discussions.
Within the workplace, doctors in training will still need to navigate disturbances and conflicting views and combine them into a single ‘good’ prescribing decision, underpinned by a clear rationale. More opportunities in medical school to practice these challenging conversations, and seniors articulating clear rationales for decisions would be helpful. The development of a common object (patient-centred care) between different stakeholders should be supported by collective efforts of developing interprofessional teamwork in prescribing processes, as has been suggested by others.7 29 Finally, workplace opportunities for doctors in training to receive real-time feedback on their prescribing decisions, combined with information on patient outcomes, will also be needed for the development of expertise and confidence.
Implications for future research
Our study contributes to research on prescribing processes, to doctors in training antibiotic prescribing experiences and to activity theoretical studies in medical education. Future studies would benefit from direct observation of the antibiotic prescribing process in other healthcare units and countries. From our current research, neither the doctors in training nor the patients appear to have much power to influence the prescribing process. However, once out of hospital, patients are critical decision-makers who decide whether and how to take their medications, and the threshold criteria for seeking further help. It would be useful to understand this posthospital pathway from the patient’s perspective. Future research might also explore how process maps (like ours) used via mobile technologies during real-time prescribing processes could improve communications within and between healthcare teams. Strategies to provide doctors in training with more feedback on their prescribing decisions and patient outcomes, to enhance their subsequent practice, are urgently required.
Acknowledgments
We would like to acknowledge the healthcare professionals Dr Aiden Plant, Dr Robert Porter and Mr Odran Farrell who gave feedback on the model, Dr Narcie Kelly who was involved in data collection for the original study and Ashling Larkin, the artist who helped us to develop Figures 1 and 2.
References
Footnotes
Twitter @AKajamaa
Contributors AK and the KM conceived and designed the study. KM and HP gathered and preliminarily analysed the data. HP was responsible for the first version of the process model. AK, together with KM, AH and CR, helped to further analyse the data and elaborated the process model. AK and AH contributed especially to the activity theoretical framework and analysis in the paper. All authors approved the final manuscript for publication.
Funding The British Society of Antimicrobial Chemotherapy provided funding for the data collection and data analysis through an education grant.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement We do not have ethics approval to make raw data from this study available for sharing.
Patient consent for publication Not required.