Article Text

Abstract
Background: The delivery of out-of-hours primary medical care in the United Kingdom has changed substantially since 2004, and there has been little examination of the effect that this has on secondary care.
Aim: The authors aimed to quantify the change in patient type presenting to our emergency department.
Methods: In this study, routinely collected coding data before, during and after the changes were analysed. Each September and October between 1999 and 2006 were included.
Results: There was a steady increase in all attendances at our emergency department. The number and proportions of patients with non-traumatic conditions rose steadily throughout the study period. The number of patients presenting with traumatic conditions stayed the same. The number of patients presenting with non-traumatic conditions out-of-hours rose after the changes were implemented.
Interpretation: The changes to the provision of out-of-hours primary care have been associated with an increase in patients with non-traumatic attendances presenting to our emergency department. This effect is most marked outside of office hours.
Statistics from Altmetric.com
Since 2004, there have been radical changes in the organisation of out-of-hours (OOH) primary care services for patients in the UK. In 2000, the Carson report1 was commissioned by the Department of Health to investigate integration of all OOH medical services. Recommendations were made to standardise care with a single telephone triage call, leading to definitive care provided by the most appropriate provider (a nurse, general practitioner (GP) or paramedic). The report favoured professional OOH providers and it was recognised that GPs should be able to devolve responsibility of OOH care to an accredited organisation with proper indemnity, meeting appropriate standards of service and care.
The new GP contract in 2003 allowed GPs to opt out of OOH provision and required Primary Care Trusts (PCTs) to take on responsibility for OOH services by December 2004. Nationally, around 75% of services are now run by PCTs and 25% are commercially run.2 Around one third of the old co-operatives are still run by the PCT. Within all these organisations, care is provided by multidisciplinary teams, with 44% of services having nurse triage and 21% with nurses prescribing.
In the evenings and weekends, both PCTs in our area operate a primary care centre, at a site remote from the emergency department (ED), with telephone triage and nurse-led services. There are some primary care facilities available for OOH care, including limited access to a GP. We aimed to examine the effect that the changed OOH primary care provision has on a medium-sized UK District General Hospital, seeing around 63 000 patients a year. In particular, we aimed to see if there was an increase in non-traumatic presentations and when this effect was most marked.
Methods
We conducted a longitudinal analysis of routine coding data. At our hospital, most attendances to the ED are coded “trauma” or “non-trauma”. Other categories relate to deaths in the department, and patients coded into these number in single figures. Almost all primary care type patients fall in to the non-trauma category, with the occasional one being coded “no abnormality detected”. We added this tiny number of “no abnormality detected” cases to the non-trauma code. We defined OOH as between 22:00 and 08:00.
We suspected that, if the change in GP OOH provision had affected ED attendances, then non-trauma attendances to the ED would have risen more than trauma attendances would in the period following the changes. Specifically, the increase in non-trauma attendances should be more for the OOH period—nights and weekends—than during GP working hours.
The number of ED attendances was extracted from the ED database in September and October, starting in 1999, the year the current data recording system started, until 2006. We used data from September and October to mitigate the effects of other variables such as school holidays. The data were analysed by using a simple linear regression model to analyse the yearly trend for 1999–2003 and plotting subsequent observed monthly attendances against predicted numbers. The proportion of non-trauma to trauma was calculated for each year. We used the χ2 test for categorical date and the p test for trend to examine trends. All statistical tests were conducted in Stata version 7 (Stata, College Station, Texas, USA).
We did not seek ethical approval as we used routinely collected anonymous aggregate data.
Results
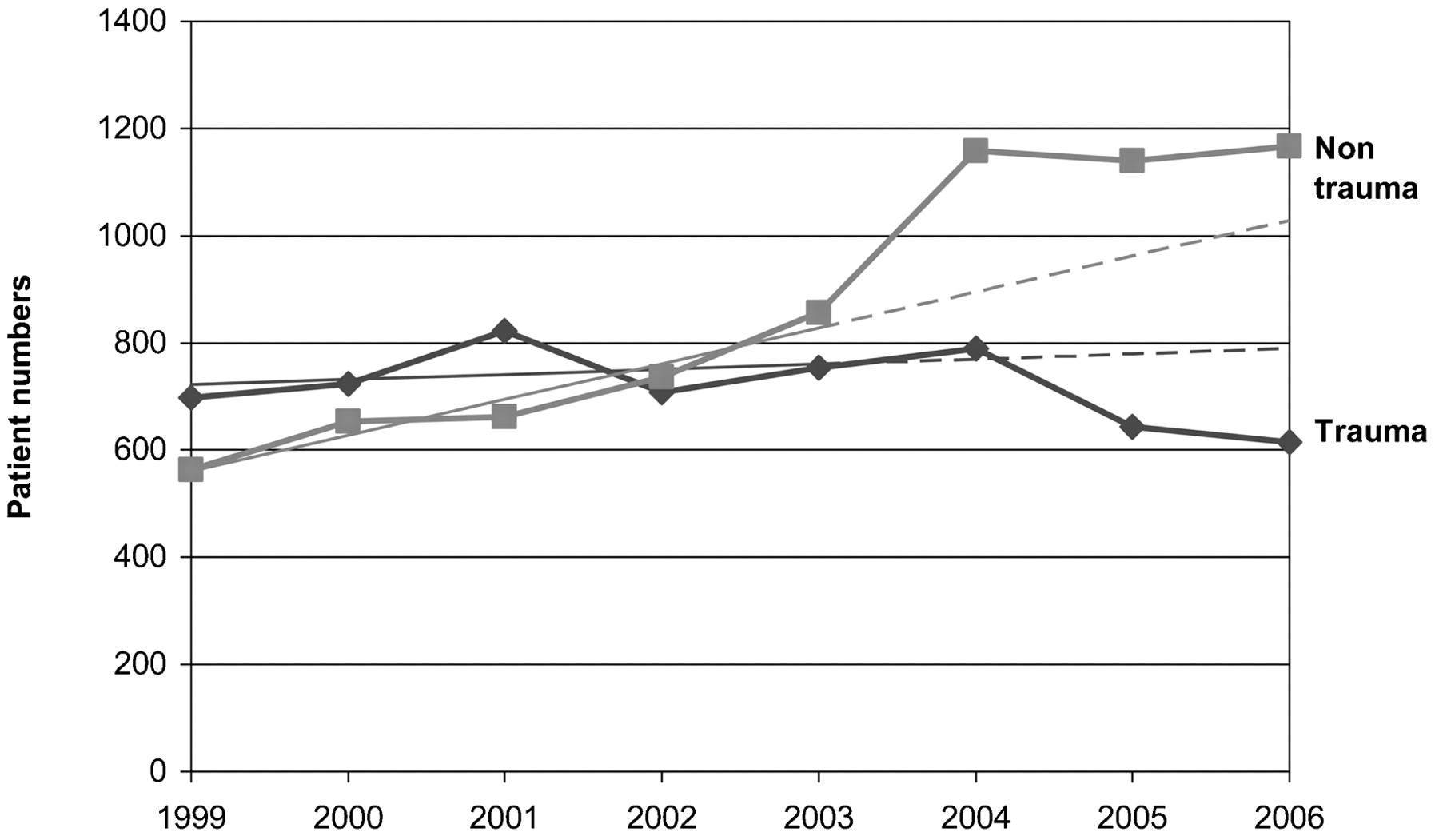
Around 4500 patients in each period attended the ED at our hospital, with an increase throughout the study period. Between 1999 and 2003, there had been an increase in numbers for non-trauma presentations, whereas those for trauma remained stable (see fig 1).

Total presentations (September and October).
When the data for 2005 and 2006 are added, it is possible to see graphically that the OOH non-trauma numbers increased above what would be expected from extrapolation of a simple regression line of best fit from the 1999–2003 data. During the daytime, non-trauma attendances rose, but by less than during the night. The increase in non-trauma presentations began before 2004, and then flattened off after 2005.

Daytime attendances with line of best fit for 1999–2003 extrapolated to 2006 (the dotted lines indicate the predicted number of attendances).
OOH trauma attendances in the same period fell, and daytime trauma increased slowly. Before the study period, neither group showed a trend in either direction.
The number attending with non-trauma during the daytime actually decreased from what was expected. Daytime trauma increased, however.
When the proportion of midweek night-time non-trauma attendances as a percentage of total is plotted (fig 3 and table 1), it can be seen that there is a steady rise throughout the years, from 42.7% of attendances to over 57.3% (a 34% relative increase). For in-hours, when conventional general practice was available, there is only an 11% relative increase, and this was not sustained after 2003.

{kind=link}
{kind=link}
{kind=link}
Daytime attendances with line of best fit for 1999–2003 extrapolated to 2006 (the dotted lines indicate the predicted number of attendances).
Proportion of non-trauma to trauma patients
The rate of increase in the non-trauma to trauma proportion for the months of September and October was at its greatest for the OOH period in 2004, which coincided with the changes in primary care practice.
The increase during daytime hours (including weekend days) has been less marked and had the largest rise the year before in 2003. These had both slowed down in 2006.
Discussion
We have demonstrated that the number and proportion of patients presenting to our ED with non-traumatic conditions have increased. This effect has been mostly marked OOH. This has coincided with nationally negotiated changes in the provision of out-hours care. The effect was more marked at night, which suggests that OOH arrangements were having more effects than the 4-hour target was. We are not entirely sure why the increase in non-traumatic presentations occurred before 2004 or then flattened off afterwards. Another major change to ED services, the 4-hour target, also came into effect in 2004. The target was in place at the beginning of 2004, but departments were to discharge or admit 98% of patients seen within 4 h by December 2004. Because these changes were concurrent, and changes to procedure had already begun to meet the target, it is not possible to separate their effects. However, the effect shown in this study is so much more marked at night, and it is likely that OOH arrangements are having more effect than the 4-hour target is. We suggested that the changes arising from the 4-hour targets would be continuous.
This has implications for the ED, not the least that an increase in patients with non-trauma during night shifts, which are necessarily least well staffed, may lead to increased waiting times and reduced patient satisfaction. Currently, ED attendances cost more than primary care episodes. Increased ED attendances are bad for the local health economy.
Various confounding factors may exist. Our hospital serves a catchment area that is predominantly urban but extends into several surrounding counties. The population of the district is expanding. According to official statistics, there was an increase of 2% in the urban population in the period 1999 to 2005.3 Official figures show that this is not a rapid increase compared with that 15 years before, and any rise would be expected to cause corresponding changes in trauma as well as non-trauma. This is not borne out in practice. The increase in activity that we have described is considerably greater than we would have expected for a population increase of 2%. There has also been a large influx of people from overseas in the area who have different health-seeking behaviour: many are here short-term and do not register with a GP. These demographic changes are difficult to quantify because official data are scarce and not reflected in census data. It is estimated that a significant proportion of total migrants to our region have come to our area, but official data do not record those leaving the area. However, overall, this will place an additional burden on how care is delivered OOH.
Our data fit with national data recently published by The Kings Fund on ED activity.4 They state that “A&E activity had been relatively stable from the late 1980s to 2002/2003, with some upward trend in first attendances but a compensating downward trend in follow-up visits. However, between 2002/2003 and 2005/2006, new attendances rose by >37 per cent, or 4.8 million attendances.” They too attribute this partly to an increased efficiency of EDs—the 4-hour target and partly to changes in primary care OOH arrangements.
There are some limitations to this work. It was conducted in a single centre and it is a matter a judgement of whether these findings apply elsewhere. However, the changes to OOH provision were nationally agreed, and we think it is likely that these findings are reflected nationally. Our study relied on routinely collected data, and there are well-described limitations to this.
Although we have demonstrated that there have been changes in the case mix attending our hospital during the reorganisation of OOH care, we have not proved that these changes are directly due to the changes in OOH provision. To do this, we would have required formal hypothesis testing at set points and control of the confounding variables, such a service reorganisation and the introduction of the 4-hour target. However, these changes happened at a very similar time in 2004. We decided on an analysis of trends because we found these more informative. Our definition of time of OOH may seem particularly late, starting at 22:00, but we would not anticipate much of a difference if we had defined an earlier time, because there were changes throughout the whole 24 hour period.
It will not be possible to further continue the work because there are major organisational changes occurring in our area, which are highly likely to increase the number of all ED attendances. However, it seems likely from these data that changes to primary care OOH services have changed the pattern of attendances to EDs. We have shown this pattern over several years now following the changes, but services are constantly changing, and as OOH providers improve and meet targets, patients may also choose to see them rather than wait for their own GP. What matters is that patients are seen by the most appropriate provider in a timely manner and that primary care continues to be the underpinning of the National Health Service.
There is little other work evaluating the impact that the national changes to primary care have had on ED attendances, and little work has been done in the UK. Those that are available have suggested that there is little change in ED attendances attributed to other changes in OOH provision.5 A study from Sheffield looking at the month before and after a change from deputising service to co-operative showed no impact on ED attendances.6
Conclusion
The change in provision of OOH primary care in 2004 has been associated with an increase in patients with non-traumatic conditions presenting to our ED, although there may be other explanations for this. This effect is most marked outside of office hours.
Footnotes
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.
Linked Articles
- Primary survey