Article Text

Abstract
Emergency departments are one of the highest risk areas in health care. Emergency physicians have to assemble and manage unrehearsed multidisciplinary teams with little notice and manage critically ill patients. With greater emphasis on management and leadership skills, there is an increasing awareness of the importance of human factors in making changes to improve patient safety. Non-clinical skills are required to achieve this in an information-poor environment and to minimise the risk of errors. Training in these non-clinical skills is a mandatory component in other high-risk industries, such as aviation and, needs to be part of an emergency physician's skill set. Therefore, there remains an educational gap that we need to fill before an emergency physician is equipped to function as a team leader and manager. This review will examine the lessons from aviation and how these are applicable to emergency medicine. Solutions to averting errors are discussed and the need for formal human factors training in emergency medicine.
- Clinical management
- ECG
- effectiveness
- emergency ambulance systems
- emergency care systems
- prehospital care
- resuscitation
- systems
- training
Statistics from Altmetric.com
- Clinical management
- ECG
- effectiveness
- emergency ambulance systems
- emergency care systems
- prehospital care
- resuscitation
- systems
- training
The ambulance alert phone rings, ‘5 year old, hit by a car, multiple injuries, distressed and combative, assisted ventilation in progress, no venous access, ETA 7 minutes’.
This situation is familiar to emergency physicians. As team leader, the emergency physician has just a few minutes to assemble a multidisciplinary hospital team and then manage and coordinate the team's efforts in this challenging and probably terrifying clinical situation.
Within a few minutes the resuscitation room will fill with paediatricians, anaesthetists, surgeons and orthopods, a radiographer or two, additional emergency physicians together with emergency department (ED) and paediatric nurses. These clinicians will be of varying seniority. The team leader may not have worked with these clinicians before and will not know how they work under pressure or what their skills in trauma might be.
Each clinician in the hastily assembled trauma team will have their own priorities and anxieties. The anaesthetist may start going through airway equipment and will ask for drugs to be prepared. He may be very concerned about delivering a rapid sequence induction in a small, multiply injured child. Junior paediatricians will busy themselves preparing cannulas and asking for blood bottles. One of them will probably be completing a ‘WETFAG’ chart on the whiteboard. The surgical members of the team may have anxieties about their ability to operate on a child. The few nursing staff present will be inundated with requests from the medical team members well before the patient has arrived. Those team members who have not found anything to do during this preparation phase will be shuffling nervously, fiddling with equipment on trolleys or just adding to the general noise. The resus room will be noisy and busy and we have not received the patient yet.
After the child is delivered by ambulance, the team will be exposed to the visual impact of a multiply injured child. Some team members will immerse themselves in different parts of patient assessment, while the ambulance crew struggle to give a handover to a team that is too busy to listen. Nursing staff will be connecting the child to monitors. Several team members will try to soothe the child loudly and ineffectively while a paediatric nurse engages with the child’s parents.
Once the team have started to assess the injured child, requests for equipment and assistance will escalate, as will the general noise level. Each specialty representative will have their own clinical priorities. The surgical team may insist on a CT scan before a surgical decision. The anaesthetist may be reluctant to deliver an anaesthetic before a surgical decision. A radiologist may suggest plain films before CT.
To provide effective clinical leadership in this situation, the team leader needs to develop a certain set of non-clinical skills. This situation demands more than currency in advance paediatric life support or advanced trauma life support; it requires the confidence (underpinned by clinical knowledge) to guide, lead and assimilate information from multiple sources to make quick and sound decisions. The team leader will encounter different personalities, seniority, expectations and behaviours from members of the team, each of whom will have their own insecurities, personality, anxieties and ego. Our team leader will need to be able to assert, negotiate, compromise and steer the team towards the rapid and effective delivery of high quality care. This is a situation that invites errors and inefficiencies, which need to be predicted and averted.
Emergency physicians have to function in multidisciplinary clinical and non-clinical environments. At one extreme is the need to assemble and lead an unrehearsed, rapidly assembled clinical team to manage a critically ill or injured patient. However, medical leadership extends to more than managing a multidisciplinary team for a severely injured child. In more routine emergency medicine work, the emergency physician has to negotiate, agree and implement a multitude of clinical pathways and management arrangements across a range of different clinical specialties and management teams within a hospital. Therefore, the emergency physician needs to develop sound team leadership and also team membership skills for the clinical and non-clinical elements of their role.
The medical leadership competency framework (May 2009) provides background and guidance on the skills required to promote optimum medical leadership.1 This document requires doctors throughout the different stages of their career to develop in the following areas:
Demonstrating personal qualities
Working with others
Managing services
Improving services
Setting direction.
The skills required to manage the unrehearsed, multidisciplinary clinical team are transferable to the less urgent challenges of working with multidisciplinary clinical and non-clinical colleagues in the health service. By teaching Emergency physicians to manage the ‘worst case scenario’, we are likely also to prepare them for working well and effectively in these less urgent challenges. In many ED, nurses with extended skills play an active role in team leadership and critical team decisions. There is therefore a need to involve our nursing colleagues in human factors training and it is time for our specialty to explore ways of delivering this training.
Errors
More than a decade ago, the US Institute of Medicine published a comprehensive report in which 44 000–98 000 deaths per year in US hospitals were attributed to medical error that could have been prevented.2 With such high costs to human life, there have been increasing concerns over patient safety, which have led to a search for ways to reduce human error and enhance risk management in medicine. It has been estimated that up to 90% of accidents in the workplace are often attributed to ‘human error’. Some industries involve continuous exposure to human error, notably the aircraft industry and health care.3 Advice from the US Institute of Medicine states:2
‘The experiences of other industries provide valuable insight about how to begin the process of improving safety of health care by learning how to prevent, detect, recover and learn from accidents.’ (p. 137)2
The importance of these human factors is well versed in aviation and is exemplified statistically with an estimated 75% of aircraft accidents or incidents being attributed to human error,3 prompting the National Aeronautics and Space Administration (NASA) to identify the human error aspects of air crashes. How do errors occur? What factors contribute to safety and efficient human and organisational performance? To answer these questions, we must first understand what is meant by human factors.
Human factors
Human factors is about people functioning in their living and working situations, their relationship with technology and the environment and about their relationships with other people.4 Human factors is therefore concerned with all the factors that can influence people and their behaviour, and the recognition of these factors is an important component of safety as they can be the cause of serious human errors.2 5
In his book, ‘Managing the risks of organisational accidents’, Reason6 proposes two approaches to the problem of human fallibility: the person (individual) and the system (organisation), and points out that accidents that can be attributed to both are central to the human error problem.
In his ‘Swiss cheese’ model, Reason7 represents failures as holes in the layers of defence, which when they all line up, result in an accident. The holes are the result of active failures made by people and also the latent conditions of the organisational system (figure 1).

The ‘Swiss cheese’ analogy of accident causation.8
Examples of layers of defence in health care include checking drugs before administration, a preoperative checklist or marking a surgical site before an operation. Holes in the layers of defence may include active failures by people to undertake the appropriate action, due to lack of training perhaps, as well as the latent conditions of the organisation such as poor design, sloppy culture and limited resources. When all these holes are lined up, the window of opportunity for a patient safety incident to occur will increase.8
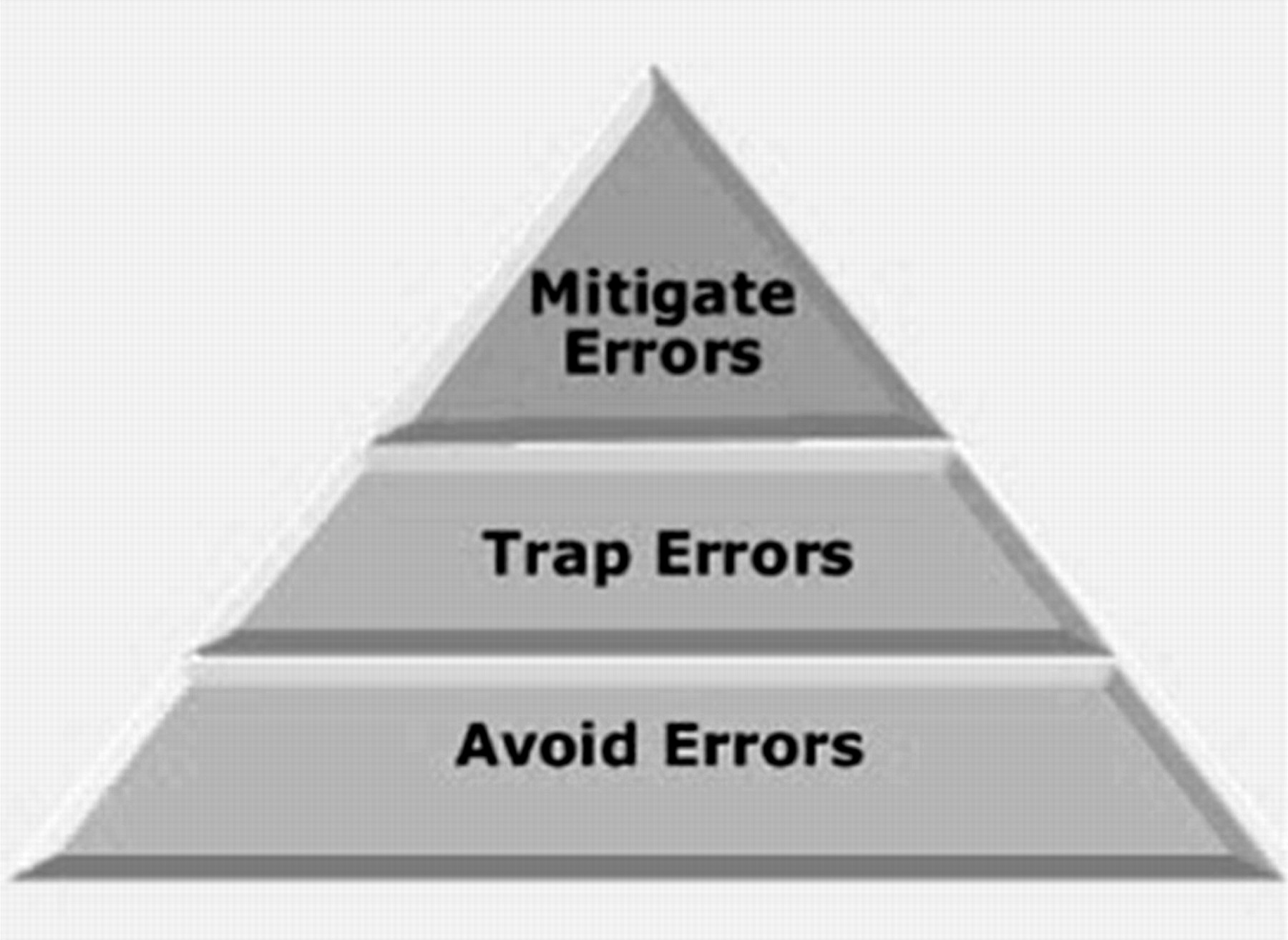
With this in mind, researchers into human factors have developed tools to manage these failures. An error management troika (figure 2), with three lines of defence has been developed with the aim of reducing the opportunity for error, detecting incipient errors and mitigating the consequences of those errors.9
{kind=link}
{kind=link}
The error troika.9
The aim of human factors training is to build defensive layers to avert errors or mitigate their effects. One way of reducing human factor errors is crew resource management (CRM), an area that has become an integral part of aviation training and operation.
CRM, as exemplified in commercial aviation, uses an error management system to reduce the incidence and consequences of human error in aircraft accidents to a minimum. It was developed as a response to new insights into the causes of such accidents. Information from flight and cockpit recordings suggested that a large proportion of air crashes resulted not from technical malfunctioning of the aircraft but from non-technical errors such as inadequate communication between crew members, loss of situational awareness and ultimately to wrong decision-making with adverse consequences.10 CRM emphasises the role of human factors in high-stress, high-risk environments and its principles appear relevant to emergency medicine.
Similarities between emergency medicine and aviation
Whenever aviation is cited as an example of effective team management to the healthcare audience, there is an almost audible sigh. However, there is value in this approach. Gaba and colleagues11 have transferred and adapted the principles of CRM to medicine and called it anaesthesia crisis resource management and have developed the key points of CRM for anaesthetic practice (box 1).12
CRM key points
Know the environment
Anticipate and plan
Call for help early
Exercise leadership and followership
Distribute the workload
Mobilise all available resources
Communicate effectively
Use all available information
Prevent and manage fixation errors
Cross (double) check
Use cognitive aids
Re-evaluate repeatedly
Use good teamwork
Allocate attention wisely
Set priorities dynamically
The ED is perhaps the most stressful and challenging hospital setting with regard to patient safety; its unique operating characteristics (box 2) make it a natural environment for studying error.
The unique operating characteristics of the ED, predisposing to human error
High turnover of patients
Diversity of clinical conditions
Time constraints
Heavy dependence of other services, for example radiology and laboratory
Multiple distractions and interruptions
Limited historical and diagnostic information
Shift work, different shift times across staff groups
Compromised teamwork
Rapidly changing and evolving situations
Involvement of clinicians from other specialties with limited understanding of working in the ED
Human factors and NOTECHS in emergency medicine
Courses such as advanced life support, advanced trauma life support and other ‘acronym’ courses have been developed to ensure that all members of the ‘acute‘ team are working to the same clinical guidelines. These have become ‘must have’ tickets for emergency physicians. While the emphasis on these courses is on clinical skills and aspects of teamwork and leadership are acknowledged, specific non-technical skills are not comprehensively addressed in these courses. There therefore remains an educational gap that we need to fill before an emergency physician is equipped to function as a team leader and manager.
Human factors training is the starting point for providing the basic framework of CRM ideas, and currently all front-line staff in aviation are made aware that systems (however finely tuned) are error-prone but with well-honed error management strategies in place, system failures and individual errors can be trapped by a well-trained team (the error management troika).
When the cognitive and interpersonal skills that underline CRM are assessed in a simulated environment, they are known as non-technical skills (NOTECHS), and refer to all the attitude and behaviours not directly related to the system management or operating procedures.13 NOTECHS have four skills categories and comprise two interpersonal skills (cooperation and leadership) and two cognitive skills (situational awareness and decision-making):
Cooperation
Leadership and managerial skills
Situational awareness
Decision-making.
Communication is inherent in all elements and is therefore not considered as a separate category. Given the temporary nature of teams, NOTECHS measures the CRM skills of each individual rather than the crew as a single entity, and has been used to assess non-technical skills before and after CRM training.14
In aviation, the use of flight simulators such as line-orientated flight training has become increasingly important in training crew members and allowing them to learn and practice CRM.13 Line-orientated flight training is a real-time flight scenario designed for pilots not only to practise line operations, but to test the non-technical skills of the whole crew. Similarly, this important training tool and the increasing availability of high-fidelity simulators in emergency medicine have enabled these skills to be delivered to healthcare professionals.
Predicting, avoiding and mitigating errors
Humans make errors in predictable and patterned ways. Novices make errors due to incomplete knowledge, while experts make errors due to the intrinsic hazards of semi-automated behaviour.7 When humans work in complex systems such as the National Health Service, the opportunities for error-inducing conditions are almost unlimited and may be exaggerated by culture and system deficiencies. Very often, no harm results from ‘routine’ errors, but eventually the consequences of these familiar and generally tolerated conditions may coincide and culminate in a disastrous outcome. An error-prone department will also significantly degrade the value of staff and the atmosphere of the workplace. We become more error prone when we experience fatigue, stress, illness, overload, inexperience or complacency, not uncommon among emergency physicians.7
Humans working in complex systems are most likely to make cognitive-type errors.7 The four triggers for these errors are:
Interruptions and distractions
Tasks required out of the normal sequence
Unanticipated new tasks
Interweaving multiple tasks.
These occur when a normally automatic process has to be consciously over-ridden. We can teach people to recognise when these situations arise and provide them with the tools to avoid error. This is where human factors training starts.
‘Every day in the NHS, tens of thousands of patients are treated safely by dedicated healthcare professionals who are motivated to providing high quality and safe clinical care. For the vast majority of patients, the treatment they receive alleviates or improves their symptoms and is a positive experience. However, an unacceptable number of patients are harmed as a result of their treatment or as a consequence of their admission to hospital.’8
This is the situation that developed at the Mid-Staffordshire Hospital Trust and it seems likely that the enquiry will identify cultural and leadership deficiencies as key causes of the system failure that has been implicated in many avoidable deaths.15
Solutions
There have been attempts to avert errors in medicine.
Checklists?
In January 2009, the national patient safety alert advised that it was mandatory for all trusts to implement the WHO surgical safety checklist from February 2010, with the aim of improving communication and teamwork and thus identifying safety issues and preventable problems. In a New England Journal of Medicine article published in 2009, Haynes and colleagues16 demonstrated that the use of a 19-item safety checklist carried out in eight different hospitals spanning the globe reduced operative complications from a baseline of 11% to 7% and inhospital death rates from 1.5% to 0.8%. As with briefing and debriefing, the checklist, if used appropriately, can open up lines of communication by creating an environment in which each member of the team feels free to speak out, thus preventing important checklist steps from being missed out and preventing an error.
In the UK, the National Patient Safety Agency advised trusts on the implementation of checklists.17 Trusts have implemented checklists in a variety of ways ranging from the development of training initiatives for theatre staff to mass email delivery.
However, a checklist is just one element of a human factors approach to safety and efficiency. As a stand-alone tool it will add little value unless supported by an overall understanding of human factors and team dynamics by the team using it. The introduction of a checklist in isolation is likely to meet resistance and fail. It needs to be integrated into routine work patterns and the benefits explained to a team who have undergone training in team function, team leadership, team dynamics and behaviour management. This will often require a culture change.
In trusts in which the checklist has been introduced as part of a human factors training intervention, with subsequent coaching in theatres, the following have been reported:
The entire team share the same plan of the day ahead
The atmosphere created empowers any team member to ask questions and challenge decisions
Monitoring vital actions becomes easier as the plan is clear
Defined expectations allow team members to be assertive
Minor errors are trapped preventing major errors.
Situation, background, assessment, recommendation (SBAR)
Communication tools such as situation, background, assessment, recommendation have been increasingly used to improve team communication by making conversations more succinct providing greater clarity of information and expectations of the actions required. This is a particularly useful communication tool when used to express concerns about the deterioration of a patient and can be used to structure further conversations.
The ‘magnificent seven’
Training staff to understand and use the ‘magnificent seven’ has been shown to make an immediate difference to the performance of surgical teams. None of these are effective unless introduced and supported by human factors training. Extending these to emergency medicine teams is also likely to be effective with appropriate training:
Briefings and debriefings
Checklists when appropriate
Effective question types
Assertion techniques
Closed-loop communication
Standardising handover
Red flags indicating loss of situation awareness.
Briefing and debriefing
In aviation, briefings are a ‘must-do’ not an optional extra. They are performed before every take-off and every landing. They serve to share the plan for what should happen, what could happen, to distribute the workload efficiently and to prevent and manage unexpected problems.
So how could we fit briefings into emergency medicine? Even though staff may be reluctant to leave the computer screen in a busy department, it is likely to be worth assembling the team for a few minutes to provide some order and structure to a busy department and plan the shift.
Briefing points should cover:
The current situation
Who is present on the team and their experience level
Who is best suited to which patients and crises so that the most effective deployment of team members occurs rather than a haphazard arrangement
The identification of possible traps and hazards such as staff shortages ahead of time
Shared opinions and concerns.
At the end of the shift a short debriefing is useful to thank staff and identify what went well and what did not. Positive outcomes and initiatives can be agreed.
Briefings and debriefings should also be undertaken before and after complex team actions. This is particularly useful in the resuscitation room.
Looking ahead
In aviation the use of high fidelity simulation allows researchers to observe and analyse teams under the most stressful of situations. Humans (however expert, dedicated and professional) will make errors and violate rules. We need to train our staff to understand when and why error is more likely to occur, and empower the team to trap or mitigate these errors. High fidelity simulators are becoming increasingly available in medical training and, therefore, we can now deliver effective human factors training in the appropriate and most useful training environment, centred around clinical scenarios.
At present, there is no formal training in emergency medicine to improve team function. Currently, CRM is not a standard part of training in emergency medicine and, despite some research, there is no clearcut evidence that it improves patient outcome, and large numbers would be needed for such a study. Nevertheless, we do know that human factors training is an integral and accepted part of aviation training and in other industries where there is high-risk activity and in which human errors can lead to adverse events. If it works for them, it should work for us.
To improve patient safety in the ED, the principles of CRM and its application must be supported by decision-makers and accompanied by organisational improvements. Although CRM/human factors training is a relatively new concept in emergency medicine, its role in preventing errors and improving safety in other specialities is well recognised, particularly in anaesthesia and critical care. With the ED posing similar levels of risk, it is time to embrace this concept and improve patient safety.
The College of Emergency Medicine has sponsored a number of courses and educational initiatives to explore the introduction of formal ‘must-have’ training in team leadership skills for the emergency physician of the future. It is anticipated that emergency physicians will have to get another ‘acronym’ ticket in medical leadership in addition to the standard ‘acronym’ life support courses.
The results of these trials will guide our specialty towards selecting and introducing the most appropriate and effective methods of training emergency physicians to meet the challenges of leading the service in an error prevention culture.
Footnotes
Competing interests AB, TD and SB have been awarded a grant to provide a pilot course in human factors training by the College of Emergency Medicine. TD is Director of Atrainability Ltd. SS: none declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Primary survey