Article Text

Abstract
Objective To strengthen clinicians’ infection control awareness and risk realisation by engaging them in scrutinising footage of their own infection control practices and enabling them to articulate challenges and design improvements.
Design and participants Clinicians and patients from selected wards of 2 hospitals in western Sydney.
Main outcome measures Evidence of risk realisation and new insights into infection control as articulated during video-reflexive feedback meetings.
Results Frontline clinicians identified previously unrecognised infection risks in their own practices and in their team's practices. They also formulated safer ways of dealing with, for example, charts and patient transfers.
Conclusions Video-reflexive ethnography enables frontline clinicians to identify infection risks and to design locally tailored solutions for existing risks and emerging ones.
- Accessible
- Affordable
- Assistive Technology
Statistics from Altmetric.com
Introduction
Healthcare-associated infections (HCAIs) pose considerable risk for hospital patients and incur huge costs for them and for funders. The US Centres for Disease Control and Prevention (CDC) estimates that “more than two million people are sickened every year with antibiotic-resistant infections, with at least 23 000 dying as a result.”1 The costs of these hospital-acquired infections “have ranged as high as US$20 billion in excess direct healthcare costs, with additional costs to society for lost productivity as high as US$35 billion a year (2008 dollars).”1
Moreover, the CDC acknowledges that these estimations “are based on conservative assumptions and are likely minimum estimates.” On its part, the European Centre for Disease Prevention and Control estimated that “4 131 000 patients are affected by approximately 4 544 100 episodes of HCAI every year in Europe”.2
Infection control strategies aiming to address these challenges have largely focused on hand hygiene compliance,3 but raising hand hygiene rates do not unambiguously correspond to lowering nosocomial infection rates.4 The relationship between infections and practice cannot be reduced to hand hygiene and thus, is affected by factors that to date have not been adequately illuminated.
The present article reports on a ‘video-reflexive ethnography’ study5 that involved frontline nursing and medical staff in reviewing footage of their own in situ practices. The study's aim was to illuminate the full complexity of the practices where infection control is imperative in order to render frontline practitioners’ awareness of risk more acute and their infection control more effective.
Since its inception in 2002,6 video-reflexive ethnography has been adopted globally as a means of involving both frontline clinicians and patients in understanding local risks and the redesigning of practices.7 ,8 To date, this methodology has focused on multidisciplinary team communication,6 ,9 clinical handover,8 ward-round redesign10 ,11 and intensive care unit (ICU) spatial design.9 It is only very recently that video-reflexive ethnography has been deployed to strengthen practitioners’ and patients’ infection control.12
Video-reflexive ethnography differs in important ways from trials that apply rigid procedures to large participant samples in the pursuit of context-independent generalisations. Video-reflexive ethnography also differs from chart analyses and surveillance initiatives whose findings make little or no reference to the in situ challenges and competing imperatives that permeate how practitioners conduct their work. Video-reflexive ethnography captures the in situ unfolding of care processes, and involves local stakeholders in decisions about what footage is collected and reviewed, how this is to be analysed and interpreted, and what actions are to flow forth from it.
The remainder of this article reports on outcomes from this process. The hypothesis that underpinned the study reported here is that through confronting footage of how they conduct their work in situ, practitioners (and patients) become aware of the tacit and messy aspects of care, and they are thereby able to strengthen their resourcefulness and resilience in the face of possible infection risk.
Approach, method and study design
Approach
Video-reflexive ethnography makes visible the complexity of in situ infection risks, raising questions about practitioners’ taken-for-granted infection control behaviours. This questioning is done by practitioners themselves when they scrutinise footage of their own real-time infection control practices. Anchored in adult-learning theory,13 video-reflexive ethnography recognises that people learn most effectively when they are enabled to scrutinise their own actual and habituated ways of being, saying and doing, and not just from simulated exercises. Their scrutiny of real-time footage translates into insights and interventions into their own taken-as-given work habits and practice assumptions.5
Ethics and consent
Ethics approvals for this study were obtained from the Western Sydney Local Health District Human Research Ethics Committee and from the investigators respective universities. Owing to the unusual nature of the project, consent was sought at multiple points. Consent was initially sought after study information was distributed through one-page handouts on information boards and via email. Consents for observation, interviews and videoing were then obtained in person after negotiation with individual participants. This involved seeking consent prior to videoing and again afterwards when clips were shown to different audiences such as colleagues or management. Participants were able to ask for video recording to be stopped at any time, or even withdraw from the project at any time.
Method
All aspects of practice that were videoed were first negotiated and agreed on with participating practitioners and patients. Equally, the choice of playback material emerged from discussions and agreements among the researcher(s) and the participants. Solutions proposed during the feedback meetings were also recorded, and made available to both the team and management.
Study design
In the study reported on here, video-reflexive ethnography was deployed in two metropolitan teaching hospitals and involved 177 participants: 87 in hospital A (50 nurses, 21 doctors, 4 allied health practitioners and 12 administrative or cleaning staff) and 90 in hospital B (57 nurses, 23 doctors, 5 allied health practitioners and 5 administrative or cleaning staff). Video-filming and reflexive feedback sessions took place over periods of 3 months in the ICU in hospital A and in two mixed surgical wards in hospital B. A total of 18 reflexive sessions were conducted, including 4 follow-up sessions after the initial ones. Prior to, as well as during, the video-reflexive ethnography, ward observations and interviews were carried out. The study design is summarised in table 1.
Study design—observations, interviews and iterative video and reflexive sessions across three wards in two hospitals
Results
Two types of results are reported here: one centring on how individuals understand their care tasks, and the other focusing on team collaboration.
Individual care results
The first type of results relates to how individuals understand their own care practices. The results presented include participants’ realisations and comments about aspects of their own or others’ practices. Here, video feedback helped practitioners come to terms with the realisation that their existing ways of working exacerbated the risk of cross-contamination:I just noticed [from looking at the video] that I put the dirty crepe bandage on his clean bed.—Nurse, reflexive session, surgical ward 1
Yes, it's very not [done] consciously. I scratch my face when I'm in there and I notice [that] on the video a lot.—Junior doctor, reflexive session, surgical team
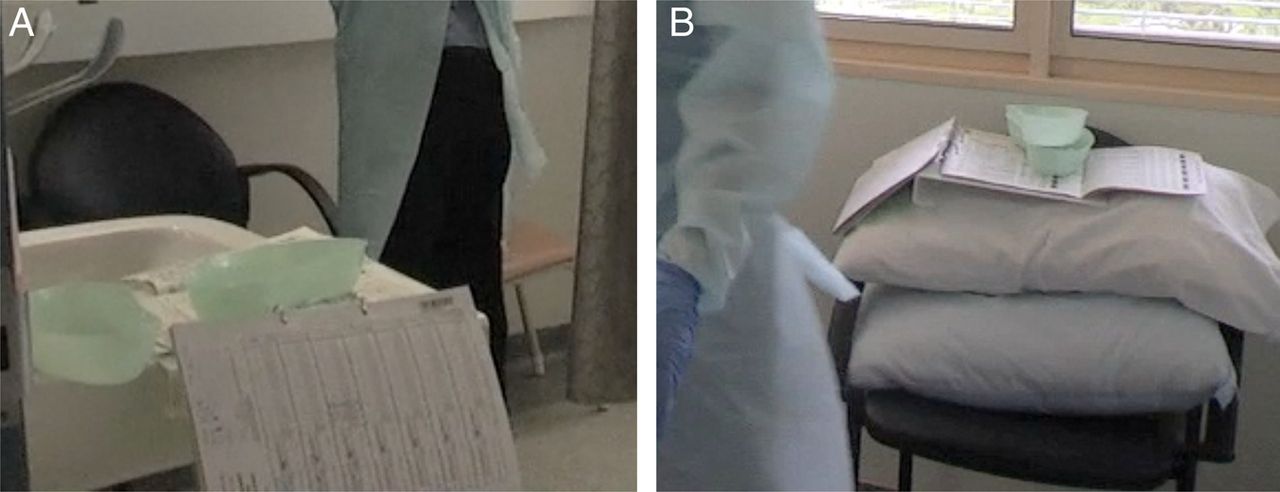
In other footage, surgical ward 2 nurses observed themselves bringing charts holding drug orders into methicillin-resistant Staphylococcus aureus (MRSA)-contaminated single-patients’ rooms when giving medications. They witnessed themselves placing the charts on potentially-contaminated surfaces, such as the patients’ beds, chairs, sinks and tables, and then returning these charts, without cleaning, to their holding area outside the rooms. When seeing this on screen, staff were able to recognise that this practice of bringing charts into infected patients’ rooms constituted a potential cross-contamination risk.
The footage further showed that the charts frequently travelled across clean–dirty boundaries. Thus, these were touched by nurses and doctors, carried between workstations and medication trolleys, and then stacked on top of other patients’ charts. Unprompted, nurses identified this handling of charts to be a problem that needed to be addressed (see figure 1A, B and online supplementary video clip A).

Infection risk potentially created by medical chart. (A) Patient chart leaning against sink and in contact with potentially contaminated kidney dishes. (B) Patient chart placed on top of potentially contaminated pillows.
Nurses next discussed the challenge of checking a patient's medical record number (‘MRN’) against information on the drug order sheet—a standard medication safety precaution—without bringing the charts into the room. In the ensuing discussion, several strategies were discussed, including the following:What I would do, I would hold the chart on my hand, grab his arm, check the MRN, and then go and put the chart out. And then come in and do the…give the heparin or whatever. You know what I mean? Without the chart being, you know, in contact with the patient's room.—Nurse, reflexive session, surgical ward 2
This nurse was suggesting is that the chart could be brought into the room held in one hand, while the nurse checks the patient's MRN on the patient's wristband with the other hand. The nurse would then return the chart to its position outside the room without contaminating it, before returning to deliver the medication.
Another medication delivery clip was shown during the same session where another nurse did as suggested in the quote above. This clip proved the feasibility of the suggested method. Some months later, in a follow-up discussion with the nursing unit manager, it was reported that this realisation and new strategy had been reinforced by peer-to-peer education between nurses and sustained throughout the ward. They had also developed other strategies to avoid contaminating charts, such as by delivering medication in pairs, when possible, or by hanging charts on the curtain railings.
Team collaboration results
Team collaboration results include two or more practitioners designing changes to practices as a result of the video-reflexive feedback discussions. One example included the redesign of how nurses, doctors and wards persons transport MRSA-colonised ICU patients through and out of the wards.
The ICU participating in this study had relatively narrow access paths through the ward. These paths also tended to be partially obstructed with equipment. This became an infection control issue when an infectious patient had to be moved (figure 2). The transfer captured on video (see online supplementary video clip B) involved four nurses and one porter, each of whom was wearing gloves, gowns and masks as personal protective equipment (PPE), and yet the infection control impact of the entire exercise was severely compromised.

{kind=link}
{kind=link}
Transferring a patient from the ward to an isolation room.
As the transfer proceeded through the ward, the video camera captured multiple instances where the staff performing the transfer had to push other equipment—such as computer terminals at other patients’ bed spaces and curtains—out of their way with their gloved hands without an opportunity to perform appropriate hand hygiene.
The reflexive sessions enabled the clinicians involved to identify multiple cross-contamination risks and design site-specific solutions for future patient transfers. Thus, as the discussion in response to the patient transfer footage portrayed in video clip B shows, clinicians proposed to be more cautious about preparing the path through the ward, and appointing one person to the role of obviating any contact between the gowned and gloved clinicians and the patient on the one hand, and other clinicians and equipment on the other hand.
Discussion
The above results show examples of professionals becoming sensitised to infection risks through viewing footage of their own ways of working. Instead of starting from the position of assessing compliance with ready-made solutions promoted in the infection-control literature (such as hand hygiene and PPE use), this video-reflexive study took the complexities and challenges of in situ practice as its point of departure. It did so on the reasoning that frontline staff and patients are rarely given the opportunity to come to terms with these complexities and challenges, and explores how to create a fit between them and generalised guidelines.
To summarise the empirical section above, the effects of the video-reflexive ethnography were threefold. First, participants were enabled to see the minutiae and the consequences of how they enact their tasks, and this enabled them to question the taken-as-given dimensions of their own habits. Second, participants were enabled to witness the connection between their own taken-for-granted actions and local infection risks, and this led them to design targeted solutions. Third, this opportunity for scrutiny, questioning and redesign was not merely relevant to addressing the specific risks revealed in the footage. This opportunity extended beyond these specific risks for highlighting the practical significance of taken-as-given activities. That is, it enabled practitioners to invest greater importance in their own agency, and in their own roles in infection control.
After all, enabling clinicians to observe and rethink their own ways of working is a significantly different strategy compared with relying on prevailing strategies to combat inservice cross-infection. Prevailing strategies fail to engage with the complex circumstances that staff encounter in everyday care. In promoting decontextualised rules and privileging compliance over learning, prevailing strategies provide no resources for local staff to develop an appreciation of and sophisticated approach to infection control that keys in to local circumstances.
In contrast to these prevailing strategies, video-reflexive ethnography reinforces for the frontline staff and patients12 the importance of appreciating the effects that flow forth from what they do and say in situ. Through viewing themselves on screen, they realise the significance of their own roles in creating safety and controlling infection risk. Video-reflexive ethnography achieves this by counter balancing the prevailing emphasis on practitioner compliance with promoting their learning. Learning occurs when we visualise the immense complexity of the work in which they are embedded, and the challenge of retrofitting this complexity into the narrow parameters of guidelines and protocols. Without dismissing the importance of compliance, we contend that learning is critical amidst complex circumstances where the only very abstract rules apply.14
Not surprisingly, there is growing interest in the observation of in situ activities (viz, Studer's ‘rounding’15 and Lean's ‘Gemba walk’16). Yet this is generally done not by frontline practitioners but by managers and leaders. Few opportunities exist as yet for frontline practitioners to observe their own work processes, and yet it is they who organise care processes for increasingly complex patients amidst rising staff turnover, technological churn, and a host of other factors that adversely affect the cohesiveness of care. As has been cogently argued in the literature on health service complexity,17 it is those at the frontline of these services—practitioners and their patients—who are best placed to ‘tame’ this complexity, provided they are enabled to develop the appropriate capacities through targeted learning.
One limitation of this study is that only some teams and limited numbers of clinicians participated in it. That said, the awareness and capability engendered by video-reflexive ethnography appears capable of spreading through peer-to-peer relationships as a novel and sophisticated stance towards work.18 Another limitation is that, as a complex intervention, video-reflexive ethnography is deeply dependent on the relationships that are built up among researchers, practitioners and patients. Claims about the effectiveness and success of video-reflexive ethnography, therefore, are inseparable from the commitment video-reflexive ethnography is able to engender among practitioners and patients to adopt a reflexive attitude towards local care practices. Finally, video-reflexive ethnography is not in the first instance about measurement, evidence and compliance, but about engagement (of practitioners and patients), relevance (for those professionals and patients), and innovation of practice (by those professionals and patients).7 However, as the above analysis has shown, video-reflexive ethnography's effects are tangible, as it instils in frontline practitioners a capacity to tame the complexity of local practice and the ubiquity of infection risk.
Conclusion
A number of recent publications has cast doubt on our ability to effectively tackle acute care infection risk. One such publication proclaims hand hygiene not to be cost-effective since it does not save enough lives to mark a significant difference.19 On its part, a recent WHO report presents the burden of in-hospital-acquired infection harm as a near enough unavoidable byproduct of being in hospital.2 These views, coupled with growing nihilism among frontline hospital staff themselves about the effectiveness of infection control, only serve to raise the cross-infection risks and exacerbate detrimental outcomes for patients.
The video-reflexive approach presented here acknowledges that the complexity of infection risk requires, besides general policies and guidelines, local practice improvement capability and an appreciation of frontline staff's critical role in achieving infection control. This capability and appreciation are contingent on investment in frontline practitioners’ (and patients12) learning and, more specifically, their infection risk awareness.14 Video-reflexive ethnography achieves these aims by involving practitioners (and patients) in observing everyday ways of working, enabling them to identify local infection risks and design safer ways of working.
The focus on involvement of practitioners and patients in tackling infection is critical. This is because no system, however well designed, is forever safe and self-explanatory for practitioners and patients, particularly when they are confronted with complex, exceptional and rapidly shifting situations. Moreover, if given the opportunity, practitioners will draw on already existing competencies and creative capabilities with which to tackle such challenges.7 ,20 For these two reasons, video-reflexive ethnography places local in situ practice and those engaged in it at the centre of attention.
In doing so, video-reflexive ethnography at once promotes learning and improvement. Indeed, video-reflexive ethnography fast tracks the efforts of practitioners and patients to reconcile evidence and policies with the vicissitudes and complexities that permeate everyday clinical work. Regarding best practice solutions as but the beginning of learning and not as final answers, video-reflexive ethnography is unique in strengthening people's involvement in making care effective and safe.7
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online Video-clip-A
- Data supplement 2 - Online Video-clip-B
Footnotes
Contributors RI, CJ, GLG, CH and MVNO conceived the study. S-YH and MW did the everyday research work. All the authors were involved in data analysis, and in the authoring and editing of the present manuscript.
Funding National Health & Medical Research Council Project Grant No. 1009178. Amount awarded: $773 000 (2011: $299 000; 2012: $249 000, 2013: $249 000). RI, GLG, CH, MVNO, CJ (2010) strengthening clinicians' capacity for infection control: a multimethod study to reduce MRSA infection and transmission.
Competing interests None declared.
Disclaimer This study's approach does not conform with any of the now standardised study protocols (eg, PRISM) as it is participative, reflexive, and therefore non-linear.
Ethics approval This study received ethical approval from the Western Sydney Local Health District Human Research Ethics Committee (ID: 2011/3/4.9 (3278) AU RED HREC/11/WMEAD/34), and this approval was ratified by investigators’ respective universities.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement De-identified video data is available. Two sample clips are included with the present submission for publication.