Article Text

Abstract
Objective To compare temporal changes in European Society of Cardiology (ESC) acute myocardial infarction (AMI) quality indicator (QI) attainment in the UK and Israel.
Methods Data cross-walking using information from the Myocardial Ischaemia National Audit Project and the Acute Coronary Syndrome in Israel Survey for matching 2-month periods in 2006, 2010 and 2013 was used to compare country-specific attainment of 14 ESC AMI QIs.
Results Patients in the UK (n=17 068) compared with Israel (n=5647) were older, more likely to be women, and had less diabetes, dyslipidaemia and heart failure. Baseline ischaemic risk was lower in Israel than the UK (Global Registry of Acute Coronary Events (GRACE) risk, 110.5 vs 121.0). Overall, rates of coronary angiography (87.6% vs 64.8%) and percutaneous coronary intervention (70.3% vs 41.0%) were higher in Israel compared with the UK. Composite QI performance increased more in the UK (1.0%–86.0%) than Israel (70.2%–78.0%). Mortality rates at 30 days declined in each country, with lower rates in Israel in 2013 (4.2% vs 7.6%). Composite QI adherence adjusted for GRACE risk score was inversely associated with 30-day mortality (OR 0.95; CI 0.95 to 0.97, p<0.001).
Conclusions International comparisons of guideline recommended AMI care and outcomes can be quantified using the ESC AMI QIs. International implementation of the ESC AMI QIs may reveal country-specific opportunities for improved healthcare delivery.
- acute myocardial infarction
- quality and outcomes of care
Statistics from Altmetric.com
Introduction
The evaluation of quality of care that extends beyond clinical outcomes is of growing interest to hospitals, physicians and patients.1 2 Evidence suggests that measuring and reporting healthcare is associated with clinical improvements.3 With this in mind, metrics have been developed by the American College of Cardiology and American Heart Association (ACC/AHA) to assess care quality and to serve as targets for quality improvement initiatives.4 5 In 2016, The European Society of Cardiology (ESC) proposed 20 quality indicators (QIs) for acute myocardial infarction (AMI), based on the ESC guidelines,6 7 spanning seven domains of care.8 These QIs have been externally validated in national clinical registries of AMI and demonstrated a significant inverse association with mortality at 30 days and 3 years.9 10
International consensus recommends the routine recording of demographic, treatments and outcomes data for AMI.5 6 Accordingly, a number of countries participate in the continuous or snapshot data collection of AMI hospitalisations into clinical registries, including the UK Myocardial Ischaemia National Audit Project (MINAP)11 and the Acute Coronary Syndrome in Israel Survey (ACSIS),12 among others.13 14 Although international comparisons have revealed differences in early mortality and between-centre variation in the provision of care following AMI, there are no studies of the temporal changes in care and outcomes between countries as measured according to published AMI QIs. This knowledge gap is important given the fact that AMI performance metrics are associated with delays to implementation of care and potentially avoidable deaths.9 10 15 16 We therefore used data from the MINAP and ACSIS national AMI registries to assess the provision of care according to the ESC AMI QIs between 2006 and 2013.
Methods
ACSIS
ACSIS is a national acute coronary syndrome (ACS) snapshot survey conducted in all 25 cardiology departments in Israel since 1992 over a 2-month period, every 2–3 years.12 ACSIS prospectively collects data pertaining to all ACS hospitalisations using a prespecified case record form, completed by unit physicians and transferred to a central database. The survey is governed and coordinated by the Working Group on Acute Cardiovascular Care, part of the Israeli Heart Society, in participation with the Israeli Association for Cardiovascular Trials (IACT). The data storage, maintenance and processing are performed by the IACT, which also reviews documents to ensure data validity. Mortality data was determined for all patients from hospital charts and by matching identification numbers of patients with the Israeli National Population Register.
MINAP
MINAP is a comprehensive registry of ACS hospitalisations occurring in all acute National Health Service (NHS) hospitals in England and Wales and is mandated by the UK Department of Health. Data regarding patient demographics, treatments and outcomes are collected for each patient, prior to secure electronic transfer to a central database under the auspice of the National Institute for Cardiovascular Outcomes Research (NICOR).11 17 There, data are linked to the Office for National Statistics for vital status and anonymised before distribution for the purposes of service evaluation and research. MINAP undergoes annual data validation by participating hospitals and the data set is reviewed biennially. Comparison of key elements of the two registries and their host health systems is provided in the online supplementary appendix 1 appendix, section 1 and online supplementary table S6.
Supplementary file 1
Analytical cohorts
For MINAP, the analytical cohort (n=17 518) was drawn from all MINAP patients aged ≥18 years with a discharge diagnosis of AMI (n=733 864) between 2006 and 2013, and by means of data cross-walking (ie, ensuring good mapping of cohorts), cases aligned to the ACSIS snapshot time periods (years 2006, 2010 and 2013) were selected. For both cohorts, cases with missing mortality data were excluded (figure 1). Other than that there were no excluded patients. No data were transferred between countries.
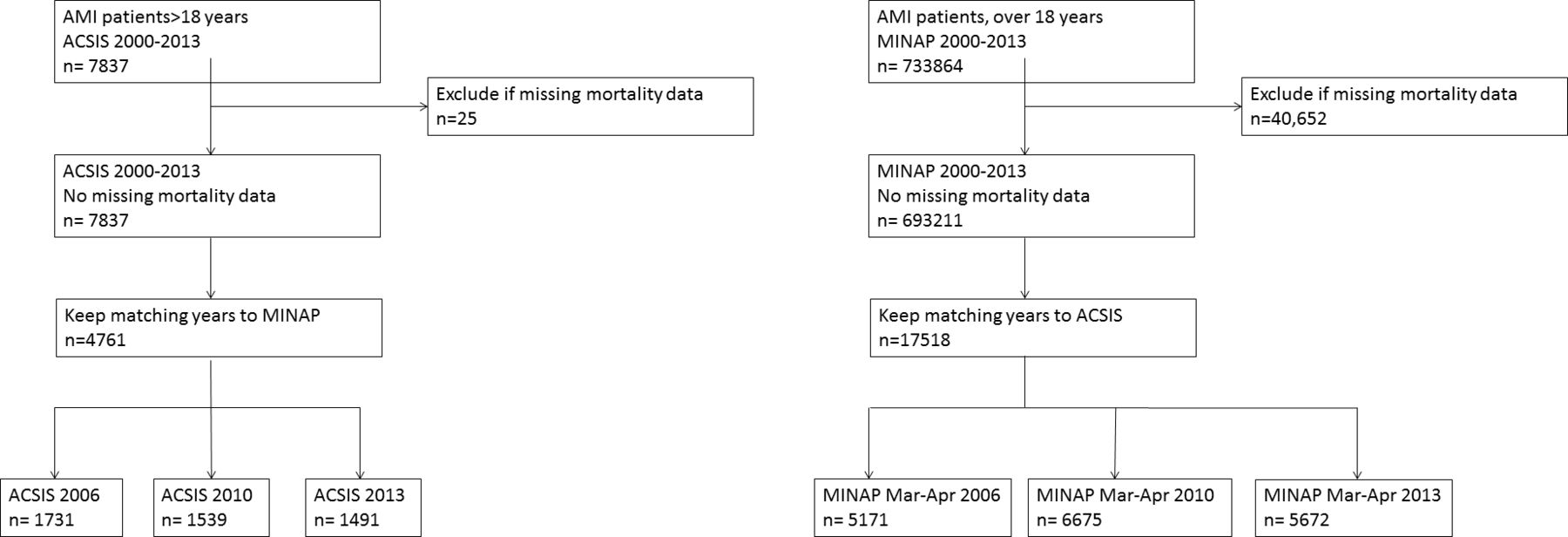
Flow diagram.
Quality indicators
Full details of the ESC AMI QIs are provided in the online supplementary table S1 8. Briefly, each of the 20 ESC AMI QIs was mapped to the respective registry’s data fields to determine those available for derivation. Patient eligibility for care was derived according to the ESC AMI QI definitions.8 Patients who were recorded as having declined treatment or in whom treatment was deemed inappropriate by treating physicians were considered ineligible, as were those with a documented contraindication for specific treatments, as defined in each country. Patients with missing data were excluded from corresponding QIs. Denominators for each QI were calculated separately with the appropriate patient population such that, for example, in-hospital deaths were not included in QIs 4 and 5 which concern medications prescribed at time of discharge from hospital.
Domain 7 of the ESC QIs assesses quality of care by means of composite scores. These were calculated using both an opportunity and all-or-none methodology. The opportunity-based score was calculated using an equal weight method based on the number of times particular care processes were performed (numerator) divided by the number of chances a patient had to receive that care (denominator). Patients achieved the composite score whether the received all of the care interventions they were eligible for. The opportunity composite score originally consisted of 12 measures; however, MINAP data only allows assessment of nine measures combined using an equal weight method.9 QI inclusion and qualification is shown in the online supplementary table S2.
Statistical methods
Patient baseline characteristics were described using numbers and percentages for categorical data, and medians and IQR or means and SD for continuous non-normally and normally distributed data, respectively. For comparison changes between 2006 and 2013, we used Χ2 test for nominal data, t-test for age and Wilcoxon ranked sum for time to arterial passage. The Global Registry of Acute Coronary Events (GRACE) risk score was used for adjusted mortality rates; details are provided in section 2 of the online supplementary appendix. A logistic regression model was fitted to quantify the association between composite opportunity-based QI and 30-day mortality. In line with previous research, for the opportunity-based composite QI, performance was split into three categories: (1) <40%; (2) ≥40% to <80% and (3) ≥80% of eligible interventions received9 18 19 and compared using the Χ2 test. Measures that had ≤30 patients with complete data for either aspect of the QI were excluded. Analysis was performed in parallel without international transfer of analytical cohorts and using R V.2.3 (R Core Team, Vienna, Austria) and Stata MP V.14.0.
Ethics
Data collection for all ACSIS surveys was approved by each hospital’s Institutional Review Board. For this study, fully anonymised data were used, and no ethics approval was required. MINAP data used for the study were fully anonymised and, as such, ethical approval was not required under NHS research governance arrangements as NICOR which includes the MINAP database (Ref: NIGB: ECC 1–06 (d)/2011) had support, under section 251 of the NHS Act 2006, to use patient information for medical research without consent. The study was conducted in compliance with the Declaration of Helsinki.
Results
Patient and treatment characteristics
There were 21 829 patients across the comparison periods, comprising 17 068 from the UK (78.2%) and 4761 from Israel (21.8%). Patients admitted with AMI in the UK were older (69.3 vs 63.8 years), more frequently were women (33.9% vs 22.2%), had lower rates of diabetes (19.6% vs 36.3%), dyslipidaemia (33.0% vs 69.5%), heart failure (5.2% vs 8.5%) and chronic kidney disease (CKD) (5.6% vs 12.9%) (online supplementary table S3). Israel had more patients with ST-segment deviation (69.8% vs 55%). In Israel, there were 2332 (49%) non-ST-segment elevation myocardial infarction (NSTEMI), compared with 10 567 (60%) in the UK.
While the rates of an invasive coronary strategy (coronary angiography (87.6% vs 64.8%), percutaneous coronary intervention (PCI) (70.3% vs 41.0%) and coronary artery bypass surgery (5.3% vs 2.0%) were higher in Israel compared with the UK, the prescription of guideline-indicated medications at the time of hospital discharge (for hospital survivors) varied—being higher in the UK for β-blockers (86.5% vs 79.4%) and ACE inhibitors (ACEi)/angiotensin receptor blockers (ARB) (84.7% vs 76.1%).
Ischaemic risk
The GRACE score was lower for patients in Israel compared with the UK (110.5 vs 121.0). This was driven by lower baseline ischaemic risk for STEMI (96.6 vs 122.3) rather than NSTEMI (123.1 vs 120.2) and, in turn, influenced by a higher age for STEMI in the UK than Israel (mean age 65.8 years vs 61.5 years) (figure 2).
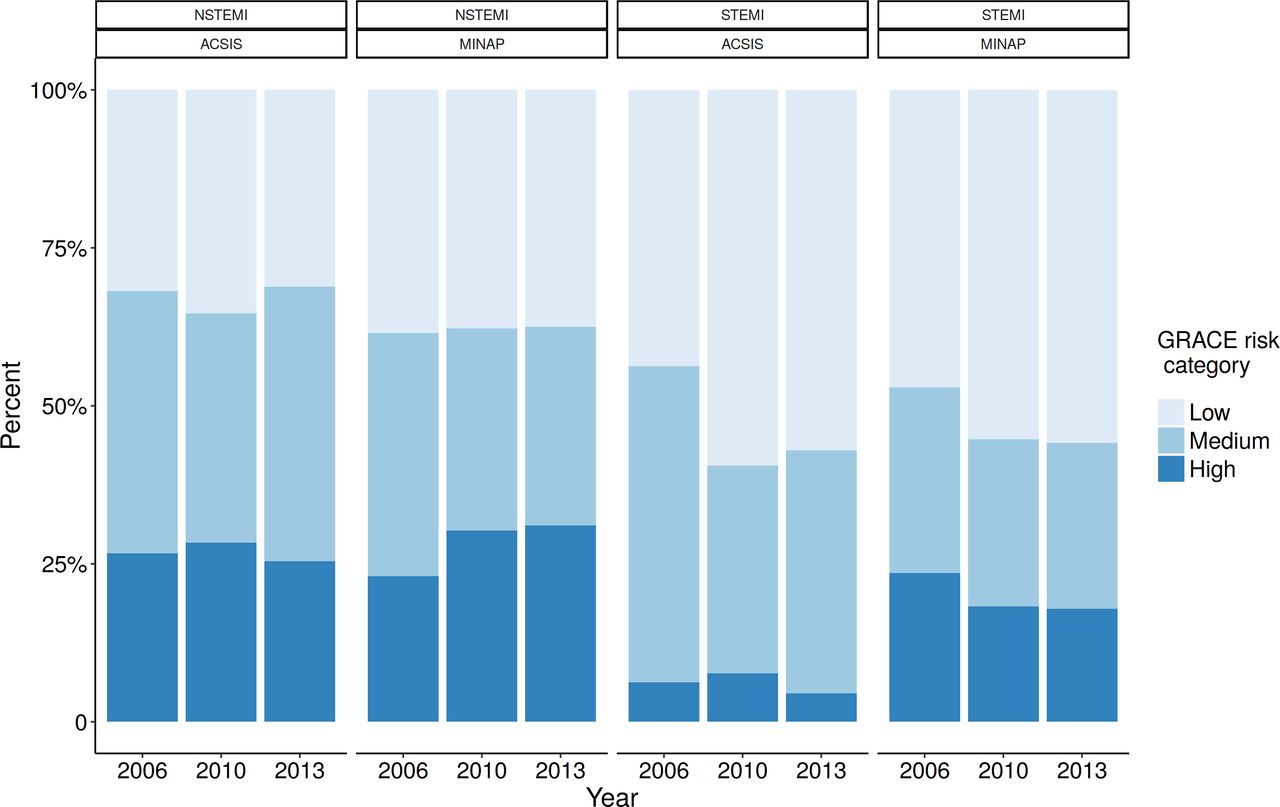
Temporal changes in baseline ischaemic risk (GRACE risk score) from 2006 to 2013 for NSTEMI and STEMI and both. ACSIS, Acute Coronary Syndrome in Israel Survey; GRACE, Global Registry of Acute Coronary Events; MINAP, Myocardial Ischaemia National Audit Project; NSTEMI, non-STEMI; STEMI, ST-segment elevation myocardial infarction.
Temporal trends in patient and treatment characteristics
In Israel from 2006 to 2013, there was an increase in the proportion of patients with hypertension (57.1% vs 65.0%), diabetes (32.3% vs 39.6%) and dyslipidaemia (69.5% vs 74.1%) and a decrease in peripheral vascular disease (10.1% vs 7.9%). Fewer patients presented with ST-segment deviation (72.9% vs 65.8%) and were more frequently in Killip class I (80.1% vs 87.2%). Rates of coronary angiography (83.3% vs 89.7%) and PCI (65.7% vs 73%) increased from a high baseline in 2006.
In the UK, there was a decline in the proportion of patients with a prior AMI (36.4% vs 32.4%), family history of ischaemic heart disease (33.0% vs 28.8%) and cerebrovascular disease (9.4% vs 7.8%) and an increase in dyslipidaemia (30.9% vs 33.2%) and CKD (3.6% vs 6.5%). More patients presented after an out-of-hospital cardiac arrest (1.7% vs 2.9%) and fewer patients with ST-segment deviation (58.7% vs 53.8%). The proportion of patients with a high GRACE risk score (22.8% vs 26.3%) increased. Rates of coronary angiography more than doubled (37.3% vs 85.5%) and rates of PCI more than quadrupled (14.4%–66.0%), both driven by an increase in primary PCI for STEMI (0.6% vs 56.2% vs 80.3%) and an invasive coronary strategy for NSTEMI (35.9% vs 63.9% vs 78.5%).
Quality indicators
Data cross-walking between the two countries found that 14 of the 20 ESC AMI QIs were available for comparison in each country. Centre organisation was not calculated as assumed 100% both in ACSIS and MINAP. For QI 2.2 c (door in and door out), the split by year resulted in very small numbers and was omitted. Both MINAP and ACSIS allow the calculation of the GRACE risk score; however, as the QI specifies recording in the medical record, they were calculated as zero. The CRUSADE score to assess risk of bleeding is not currently recorded or can it be calculated in MINAP or ACSIS, so calculated as zero. For QI 5.1 (secondary prevention with high-dose statins), discharge with statins was used for all patients (MINAP) or were not recorded (ACSIS) as surrogate. In addition, information regarding QI 6.1 (patient satisfaction) is not recorded in both registries and was omitted.
In the UK between 2006 and 2013, the time and range of times to achieve arterial access for PCI was reduced by at least half (80.4 (IQR 135) vs 40.2 (31) min) compared with Israel where they were stable (70.3 (68) vs 67.0 (72) min). By contrast, in Israel, a high proportion of NSTEMI received timely coronary angiography (83.8% vs 64.1% in the UK in 2013). The assessment of left ventricular function on discharge was higher in Israel (72.2% in 2013) despite temporal improvements in the UK (50.1% in 2013 vs 22.1% in 2006). The prescription of P2Y12 inhibitors in the UK increased from 1.1% in 2006 to 94.9% in 2013, compared with 77.4% and 86.3% in Israel for respective periods. In 2013, fondaparinux was rarely used in Israel with higher, yet modest, rates of use in the UK (2.4% vs 49.5%). Healthcare performance as measured by the composite QIs increased in the UK from 46.2% in 2006 to 80.0% in 2013 (7.1, opportunity based score) and from 1.0% in 2006 to 86.0% in 2013 (7.2, all-or-none score), with no change in 7.1 (86.8% vs 85.9%) and an increase in 7.2 in Israel (70.2% vs 78.0%). A heatmap figure with performance of selected QIs by registry and year is presented in figure 3. All QIs appear in the online supplementary table S4.

{kind=link}
{kind=link}
{kind=link}
Proportion of quality indicator adherence by registry and year. ACEi, ACE inhibitor; ACSIS, Acute Coronary Syndrome in Israel Survey; ARB, angiotensin receptor blocker; BB, beta blockers; DAPT, dual antiplatelet therapy; LV, left ventricular; MINAP, Myocardial Ischaemia National Audit Project; NSTEMI, non-STEMI; QI, quality indicator; STEMI, ST segment elevation myocardial infarction.
Mortality
Crude 30-day and 1-year mortality rates declined more between 2006 and 2013 in the UK than in Israel (30 day: −3.2 vs −1.6%; 1 year: −11.9% vs –2.3%), though at the end of the study period were higher in the UK than Israel at 30 days (7.8% vs 3.8%) and at 1 year (10.1% vs 8.6%). After adjustment for baseline ischaemic (GRACE) risk, 30-day mortality rates decreased equally over the study period in the two countries (−0.6% and −0.5%, respectively) and were higher in the UK compared with Israel in 2013 (7.6% vs 4.2%).
In Israel, increasing opportunity-based composite QI attainment from low to intermediate to high was associated with decreasing 30-day mortality (61.0% vs 21.8% vs 2.0% 30-day mortality, p<0.001 for difference). Similarly, higher opportunity-based composite QI attainment was associated with lower GRACE adjusted 30-day mortality (OR 0.95; 95% CI 0.95 to 0.97, p<0.001) with the magnitude and direction of the association remaining after further adjustment for year of hospitalisation (OR 0.98; 95% CI 0.97 to 0.98, p<0.001).
This pattern was mirrored in the UK with a reduction in crude 30-day mortality (43.2% vs 6.2% vs 2.9%; p<0.001 for low, intermediate and high attainment, respectively) and 1-year mortality (53.8% vs 17.0% vs 6.4%; p<0.001, respectively). Equally, opportunity-based QI attainment was associated with decrease in GRACE adjusted 30-day mortality (OR 0.97; 95% CI 0.96 to 0.97, p<0.001) which also remained after adjustment for year of hospitalisation (OR 0.97; 95% CI 0.95 to 0.97, p<0.001). Similar results were observed when examining 1-year mortality in 30-day survivors against QI attainment percentage (OR 0.98; 95% CI 0.97 to 0.98, p<0.001 for both cohorts).
Discussion
In this international study, we used the ESC AMI QIs to compare temporal changes in the delivery of healthcare across Israel and the UK. We found that in Israel, patients with AMI tended to be younger, had a lower baseline ischaemic risk, more frequently received an invasive coronary strategy and had lower mortality rates compared with the UK. Even so, we noted a rapid upturn in the UK in the attainment of guideline-indicated care as quantified by the ESC AMI QIs. Moreover, this study provides evidence for the application of the ESC AMI QIs for comparative evaluation of AMI healthcare delivery to highlight where there may be opportunities for quality improvement and, therefore, improved clinical outcomes for AMI.
We found that adherence to the ESC AMI QIs improved in both countries and more so in the UK from 2006 to 2013. Part of the improvement in the UK could be attributed to slower adoption of guideline-recommended care. In both countries, there was lower proportion of electrocardiographic ST-segment deviation at the time of admission to hospital, likely related to increased use of troponins and of higher sensitivity. In Israel, a high proportion of NSTEMI received timely coronary angiography, which may be explained by the fact that in Israel, all hospitals but one that receive patients with ACS have on-site 24/7 catheterisation laboratories. For the UK, timely coronary angiography and PCI for NSTEMI and STEMI increased. This may be attributed, in part, to comprehensive tracking and auditing of clinical care and timely publications of centre performance20 and through local, regional and national network quality improvement exercises.21 This may also explain the improvement in QI attainment in the UK, in addition to the availability of specific treatments through the NHS. Indeed, the later adoption of dual antiplatelet therapy in the UK compared with Israel demonstrates the influence of system decisions (eg, approval/funding of certain drugs) in adoption and compliance with guideline recommended therapy. Going forward, Israel could, therefore, aspire to improving times to PCI for STEMI, while for the UK timely greater access to and timely revascularisation for NSTEMI deserves greater attention. Both countries require improved assessment of LV function.
Over the study period, as adherence to guideline-indicated care improved in each country, we noted a corresponding decline in mortality. Indeed our findings are in line with earlier research from the UK9 22 and France13 that separately reported a statistically significant inverse association between ESC AMI QI attainment and early and late mortality.
Despite substantial improvements in treatment and associated survival,23 global burden of AMI remains high. Recently, the ESC Atlas project highlighted major between country differences in cardiovascular health, delivery and standardised outcomes across Europe.24 25 Earlier work found that the rates of adoption of cardiovascular health technologies such as primary PCI for STEMI vary between and within countries26 27 and that missed opportunities in the provision of AMI guideline-indicated care were associated with excess mortality.15 28 Notably, the importance of ‘measuring to improve care’ has been emphasised by organisations1 as well as by international guidelines and is a first necessary step in any attempt to reduce variation in cardiovascular disease. While earlier research has revealed disparities in early mortality, suggested to be attributable to level of care, these studies did not map care to internationally recognised performance indices.29 30 To our knowledge, our study is the first time that internationally recognised AMI QIs have been used to compare the levels of provision of guideline-indicated care between two countries. Thus, our investigation may serve as an example and incentive to record and report, both general patient data regarding AMI on a national and hospital level, and of QIs, in order to improve patient care and reduce the burden of disease.
Although this work has strengths, one must appreciate its limitations. Each registry has its own data definitions, mechanisms for identifying potential participants and data recording. The GRACE and CRUSADE scores were not recorded in either registry, nor was patient satisfaction. Assessment of left ventricular systolic function for UK participants was low, and for Israel declined, which may have reduced the available data for assessment of an eligible population for receipt of ACE-inhibitors and β-blockers. Another weakness is the misperception of causation arising from the inverse association between attainment of care and outcomes—we describe association with mortality and not causation. It is certainly possible that other factors may explain and contribute to this association such as lower risk patients receiving more treatments compared with sicker patients with an unrecorded contraindication receiving fewer. In this context, the expected reduction in mortality should be assessed according to relevant randomised controlled trials and not this investigation of care quality.
Key messages
What is already known about this subject?
The European Society of Cardiology has developed a suite of quality indicators for acute myocardial infarction. Increased quality indicator attainment for acute myocardial infarction is associated with decreased mortality.
What does this study add?
The European Society of Cardiology quality indicators for acute myocardial infarction may be used in nationwide continuous and snapshot registries to investigate between and within country care and outcomes for acute myocardial infraction
How might this impact on clinical practice?
Nationwide cardiovascular data interrogation may enable health systems to ascertain where quality improvements may be made for acute myocardial infarction such that premature death from cardiovascular disease is reduced.
Acknowledgments
MH was funded by the Wellcome Trust as a Sir Henry Wellcome Postdoctoral Fellow (reference: 206470/Z/17/Z).
References
Footnotes
†Dr Oren Zusman died on 29 January 2019.
Contributors OZ, OB, ZI and CPG have contributed to the conception or design of the work. OZ, OB, TBD, MH, ZI, CPG and AT have contributed to the acquisition of data. OZ, OB, ZI, CPG, RK, FS, AT and KAAF have contributed to analysis or interpretation of data. OZ, OB, CPG, ZI agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors took part in drafting the work or revising it critically for important intellectual content, and all authors gave final approval of the version published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note We respect Dr. Oren Zusman’s untimely death on January 29th, 2019. Dr. Zusman was an extremely talented and passionate physician-researcher, with a brilliant future ahead of him. He will be deeply missed by all of his colleagues, friends, and family. He is survived by his wife, Maayan, and three children. May his memory be a blessing.
Patient consent for publication Not required.