Article Text

Abstract
Background The objective of the study was to identify any changes in primary percutaneous coronary intervention (PCI) for ST-elevation myocardial infarction (STEMI) in England by analysing procedural numbers, clinical characteristics and patient outcomes during the COVID-19 pandemic.
Methods We conducted a retrospective cohort study of patients who underwent PCI in England between January 2017 and April 2020 in the British Cardiovascular Intervention Society-National Institute of Cardiovascular Outcomes Research database. Analysis was restricted to 44 hospitals that reported contemporaneous activity on PCI. Only patients with primary PCI for STEMI were included in the analysis.
Results A total of 34 127 patients with STEMI (primary PCI 33 938, facilitated PCI 108, rescue PCI 81) were included in the study. There was a decline in the number of procedures by 43% (n=497) in April 2020 compared with the average monthly procedures between 2017 and 2019 (n=865). For all patients, the median time from symptom to hospital showed increased after the lockdown (150 (99–270) vs 135 (89–250) min, p=0.004) and a longer door-to-balloon time after the lockdown (48 (21–112) vs 37 (16–94) min, p<0.001). The in-hospital mortality rate was 4.8% before the lockdown and 3.5% after the lockdown (p=0.12). Following adjustment for baseline characteristics, no differences were observed for in-hospital death (OR 0.87, 95% CI 0.45 to 1.68, p=0.67) and major adverse cardiovascular events (OR 0.71, 95% CI 0.39 to 1.32, p=0.28).
Conclusions Following the lockdown in England, we observed a decline in primary PCI procedures for STEMI and increases in overall symptom-to-hospital and door-to-balloon time for patients with STEMI. Restructuring health services during COVID-19 has not adversely influenced in-hospital outcomes.
- percutaneous coronary intervention
- acute myocardial infarction
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
In response to the COVID-19 pandemic, routine hospital services including cardiac catheterisation have been restructured in order to increase hospital capacity for patients infected with COVID-19 and reduce the risk of cross-infection. This has led to the cancellation of some elective procedures and reduced access to care for patients without COVID-19 related disorders. Many countries have imposed social containment mandates, known as ‘lockdown’, in order to reduce the spread of the virus, which may have contributed to patient delays in seeking emergency care, because of fear of contracting COVID-19 at hospitals, and this has resulted in a reduction in cardiovascular admissions.1–3 This would inevitably have important consequences especially in conditions such as ST-elevation myocardial infarction (STEMI) in which timely coronary revascularisation is proven to reduce mortality and complications.4
While there are isolated local and regional level reports that the COVID-19 pandemic is associated with a reduction in both presentations with acute myocardial infarction and percutaneous coronary intervention (PCI) procedures,5–9 there have been no previous data regarding its impact on national primary PCI rates and practices and whether there have been changes in either procedural or clinical characteristics of patients or their clinical outcomes.
Following dialogue with the Chief Scientific Advisor to the government of the UK, a series of analyses by the National Institute for Cardiovascular Outcomes Research (NICOR) were endorsed to help inform government decision making. The objective of this current analysis is to identify the changes in primary PCI activity during the COVID-19 pandemic from a national perspective, including any changes in the clinical presentation and characteristics of patients and their clinical outcomes.
Methods
The reporting of this cohort is in accordance with the recommendations of the STrengethening the Reporting of Observational studies in Epidemiology statement.10
The British Cardiovascular Intervention Society (BCIS) registry contains data from all consecutive adults undergoing all PCI in the UK in the National Health Service Hospitals in England. The dataset has around 120 variables covering demographic characteristics, clinical information, periprocedural and outcome variables, as previously described.11–13 BCIS has made it their mandate that all operators record information for all PCI procedures undertaken, and data collection is overseen by NICOR.14
Study design, population and outcomes
We conducted a retrospective cohort study of all patients who underwent PCI for STEMI in England between 1 January 2017 and 30 April 2020 in the BCIS database. Hospitals either enter data directly into a web-based interface provided by NICOR or upload data from their local database. Hospitals were encouraged to upload their data more frequently than usual to facilitate more contemporaneous analysis. To this end, they received special communications from both the British Cardiovascular Society and the BCIS to their members. In addition, staff at NICOR made direct contact with each hospital’s cardiovascular audit team. This project only included data from hospitals that successfully uploaded data on PCI procedures in each month of the current year until the end of April 2020 (by 7 May). This was necessary to ensure only those centres in whom all procedures had been reported and uploaded until the end of April were included, in order to minimise the risk that we included data from centres that had failed to upload their most recent PCI activity. Patients not allocated by gender were excluded as were those who did not have PCI or those admitted to private hospitals, who represent less than 5% of PCI activity in the UK and virtually no primary PCI.
The primary outcome of interest was the number of primary PCI procedures for STEMI undertaken before and after the COVID-19 pandemic lockdown on 23 March 2020, and the secondary outcomes were the in-hospital mortality and major adverse cardiovascular events (MACE; a composite of death, reinfarction and unplanned re-PCI) for these procedures over the same period. Other in-hospital outcomes were receipt of transfusion (blood or platelet), major bleeding, embolic stroke, coronary perforation, retroperitoneal bleed, renal failure/dialysis and re-PCI. Patients who were admitted with STEMI but remained in hospital beyond 30 April 2020 were classified according to whether they had in-hospital mortality at the time of latest follow-up (7 May 2020). Those that remained in hospital and were not discharge were classed as being alive.
Covariates
Data were collected on patient demographics, comorbidities and treatments received (described in online supplementary data 1).
Supplemental material
Statistical analysis
Statistical analyses were performed on Stata/MP V.16.0. We included patients with primary PCI for STEMI, facilitated PCI for STEMI and rescue PCI for STEMI in the cohort, but only those with primary PCI for STEMI were included in the analysis. The cohort was divided into patients who underwent primary PCI for STEMI in 2017–2019 and those who had a primary PCI procedure performed from 1 January to 30 April 2020. For the analysis of trend, the monthly average PCI procedures for the years 2017, 2018 and 2019 were determined, and these averages were compared against the number of procedures in each month in 2020. The date of the UK lockdown was 23 March 2020 and was marked in the figures between the months March and April 2020. Descriptive statistics are presented by whether primary PCI took place before or after the lockdown. Median values and IQRs for continuous variables and the number and percentages for categorical variables were reported. Using all patients admitted in 2017–2019 as a reference group, the Mann-Whitney test for continuous variables and χ2 test for categorical variables were used to determine if there was any statistical difference in patient characteristics, procedural variables and in-hospital outcomes after and before the lockdown. Figures were used to show timing from symptom-to-hospital and door-to-balloon as well as in-hospital death and MACE before and after the lockdown. This was done for the overall primary PCI cohort for STEMI as well as the subgroups that were admitted to the PCI centre directly from the community and those that were transferred to the PCI centre from another hospital. Multiple logistic regression models were used to evaluate the independent odds of in-hospital mortality and MACE. This model was adjusted for all covariates previously mentioned, except for left ventricular function, smoking status and ethnicity because of the extent of missing data for these variables. Additional analyses were performed where the mi impute chained function was used to generate 10 complete datasets to account for missing data. Multiple logistic regressions were then conducted to evaluate the independent odds of in-hospital mortality, and MACE were performed with adjustments all variables including left ventricular function, smoking status and ethnicity. Finally, the descriptive statistics were also presented in tables stratified by indication for PCI. A sensitivity analysis was performed restricting the control group to the same months of January–April in the calendar years 2017, 2018 and 2019 in order to avoid any potential issues related to seasonal differences in the numbers of procedures.
Results
A total of 34 127 patients undergoing PCI with STEMI were included in the analysis (figure 1). The list of hospitals included in the analysis is shown in the online supplementary data 2. This includes STEMI patients undergoing primary PCI (n=33 938), facilitated PCI (n=108) and rescue PCI (n=81). The missing data for the cohort of patients with STEMI who underwent primary PCI is shown in online supplementary table 1.
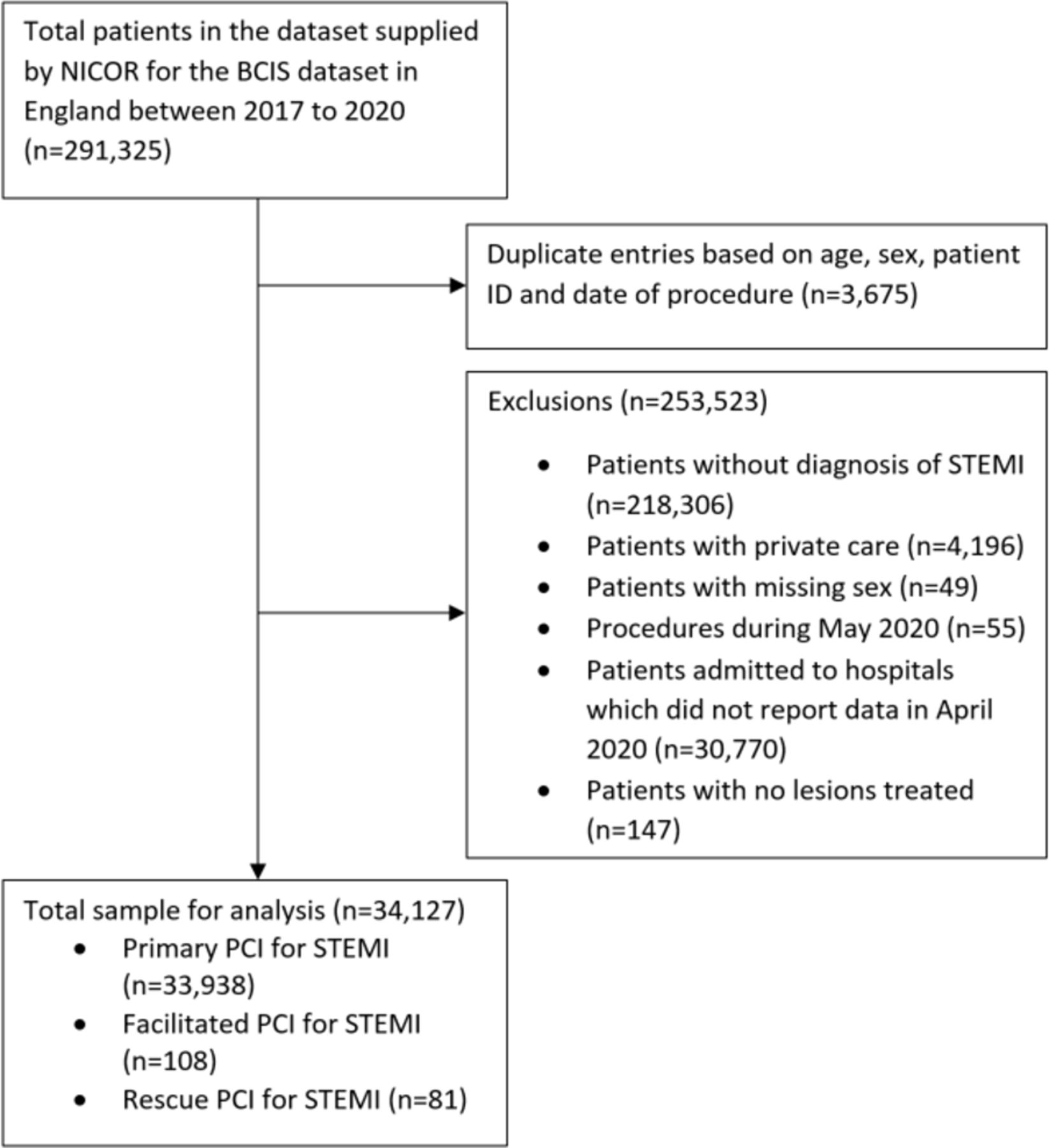
Flow diagram of patient inclusion. BCIS, British Cardiovascular Intervention Society; NICOR, National Institute of Cardiovascular Outcomes Research; PCI, percutaneous coronary intervention; STEMI, ST-elevation myocardial infarction.
The numbers of primary PCI for STEMI over time is illustrated in figure 2. A 43% decline in monthly average procedures was recorded between 2017 and 2019 (865) to 497 in April 2020. The changes in rescue and facilitated PCI for STEMI is shown in online supplementary figure 1, and there were no clinically significant increases.

Rate of primary percutaneous coronary intervention (PCI) for ST-elevation myocardial infarction (STEMI) over time.
The characteristics according to month are shown in online supplementary table 2. Compared with 2017–2019, patients admitted with primary PCI for STEMI in the month of April 2020 were more likely to have radial access (89.1% vs 83.9%, p=0.002), multivessel PCI (16.9% vs 12.8%, p=0.007) and have longer time from symptom-to-hospital (median 135 min vs 153 min, p=0.004) and door-to-balloon time (median 37 min vs 48 min, p<0.001).
The percentage difference comparing the number of procedures after and before the lockdown was not consistent across all primary PCI volume centres as there was a decline of 20.4%, 25.9%, 11.1% and 56.8% across the quartiles 1, 2, 3 and 4 based on volume of primary PCI. It appears that the largest decline was observed in highest volume centres. The patient characteristics for primary PCI prelockdown and postlockdown are shown in table 1. Patients postlockdown had a greater proportion of multivessel intervention (16.0% vs 12.7%, p=0.012) with an increased use of prasugrel (12.9% vs 6.4%, p<0.001), with a decline in clopidogrel (11.0% vs 21.5%, p<0.001), ticagrelor (41.0% vs 48.6%, p<0.001), glycoprotein IIb/IIIa inhibitor (22.6% vs 27.7%, p=0.003) use.
Patient characteristics for patients who underwent primary PCI for ST-elevation myocardial infarction according to those who are admitted prelockdown and postlockdown
The characteristics of patients according to direct admission from community compared with transfer from another hospital are shown in online supplementary table 3 and transferred patients were younger (62 vs 64 years, p<0.001) and a greater proportion were male (76.6% vs 74.3%, p<0.001), of non-Caucasian ethnicity (19.3% vs 13.4%, p<0.001) and had out-of-hours PCI (57.9% vs 53.3%, p<0.001).
The time from symptom to hospital and from door to balloon before and after lockdown are shown in figure 3. For all patients, the time from symptom to hospital was greater after the lockdown (median 150 min vs 135 min, p=0.004) and the door-to-balloon time was also greater after the lockdown (median 48 min vs 37 min, p<0.001). The increase in time from symptom to hospital was observed after lockdown for the subgroup of patients admitted directly from community (median 145 min vs 135 min, p=0.020) as well as those that were transferred between hospitals (median 239 min vs 235 min, p=0.045). The door-to-balloon time was also greater after the lockdown for patients admitted directly from the community (median 41 min vs 28 min, p<0.001) but not statistically different for those with hospital transfer (median 185 min vs 143 min, p=0.13).

Median time to from symptom-to-hospital and door-to-balloon time percutaneous coronary intervention (PCI) prelockdown and postlockdown.
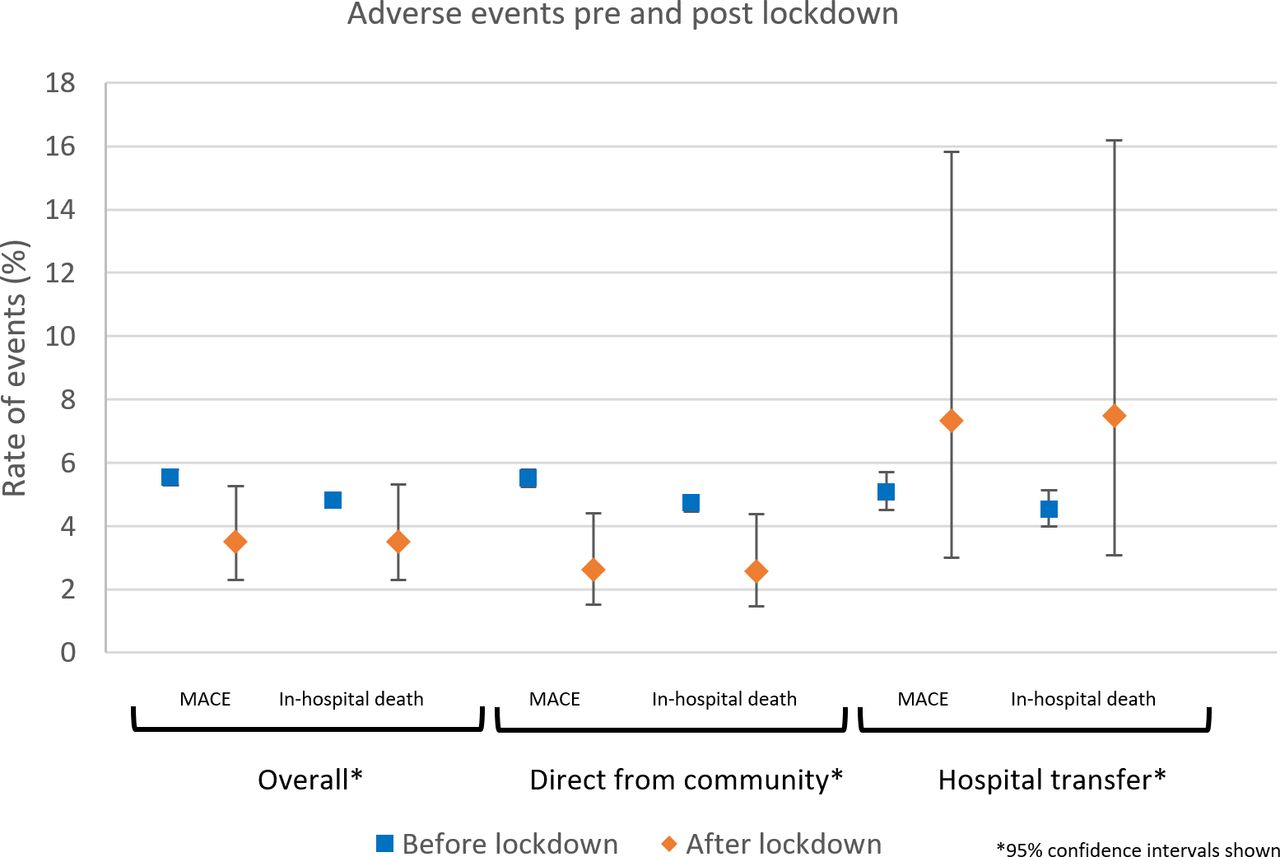
Crude in-hospital patient outcomes prelockdown and postlockdown are shown in table 2 and figure 4. No significant differences in mortality were observed overall (3.5% vs 4.8%, p=0.12), but in-hospital MACE was significantly reduced postlockdown (3.5% vs 5.5%, p=0.022), and there was a shorter median length of stay postlockdown (2 days vs 3 days, p<0.001). Similar patterns were observed for patients who were admitted directly from the community (2.6% vs 4.7%, 2.6% vs 5.5%, respectively). For patients who were transferred from another hospital, there was an increase in both in-hospital death (7.5% vs 4.5%) and MACE (7.3% vs 5.1%).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
In-hospital mortality and major adverse cardiovascular events (MACE) prelockdown and postlockdown.
Patient outcomes for patients who underwent primary PCI for ST-elevation myocardial infarction according to those who are admitted prelockdown and postlockdown
The adjusted odds of in-hospital death and MACE are shown in table 3. No differences were observed for both outcomes overall (OR 0.87, 95% CI 0.45 to 1.68, p=0.67 and OR 0.71, 95% CI 0.39 to 1.32, p=0.28, respectively) or in the subgroups according to direct or interhospital admission. After imputations for missing data, the analysis adjusted additionally for left ventricular function, ethnicity and smoking status and similarly showed no significant differences in in-hospital outcomes.
Multivariable odds of major adverse cardiovascular events (MACE) and in-hospital death for patients prelockdown and postlockdown who underwent primary percutaneous coronary intervention for ST-elevation myocardial infarction
The sensitivity analysis only including the months of January–April for the calendar years 2017–2019 are shown in online supplementary figure 2 and online supplementary table 4. The results are largely similar to those reported in the overall analysis.
Discussion
Our evaluation to describe national cases of primary PCI activity for STEMI during the COVID-19 pandemic has several key findings. First, the decline in number of cases of primary PCI for STEMI started before the lockdown on the 23 March 2020, and there was a 43% decrease by the end of April 2020. Second, the lockdown was associated with increases in symptom-to-hospital time and door-to-balloon time. Third, after the lockdown, the difference in time from symptom to hospital and door to balloon was greatest for patients who underwent hospital transfer. Finally, once differences in baseline characteristics were adjusted for, there were no differences in clinical outcomes (mortality and MACE) before and after lockdown. These findings suggest that primary PCI for STEMI has declined after the national lockdown in England but restructuring of hospital services during the COVID-19 pandemic has not adversely compromised in-hospital outcomes for patients having these procedures.
Our results support the decline in primary PCI procedures for STEMI reported in other studies, but we add some additional value to such observations by describing clinical and procedural characteristics and clinical outcomes after the COVID-19 lockdown using previous years as a reference. During the early phase of COVID-19 pandemic, there was an estimated 38% reduction in US cardiac catheterisation laboratory STEMI activations from nine high-volume centres.8 Another survey of 73 centres in Spain reported a 40% reduction in procedures performed in the STEMI settings.9 We report a 43% reduction in all STEMI-related PCI procedures (including primary, rescue and facilitated) in England in the month after the lockdown. Importantly, our paper shows that patients undergoing primary PCI were not at increased odds of in-hospital death and MACE compared with patients before the lockdown period.
There are several explanations why there may be a decrease in primary PCI for STEMI during the COVID-19 pandemic. One possibility is that there was a lower incidence of STEMI during the outbreak, but this is unlikely. A more convincing explanation is that lower rates of STEMI relate to multiple factors including avoidance of medical care or concerns over contracting COVID-19 in hospital, misdiagnosis and increased use of pharmacological reperfusion due to COVID-19.8 In England, there were clear government recommendations to ‘stay at home and protect the National Health Service (NHS)’ which may have created an atmosphere of fear of contracting COVID-19 by leaving the home and going to hospital. The consequences of not seeking medical care following a STEMI may be significant; for example, a 58% increase in out-of-hospital cardiac arrests was observed between February and March 2020 compared with 2019 in the Lombardia Cardiac Arrest Registry.15 In addition, a reduction in primary PCI activity may be related to reduced catheter laboratory capacity due to staff sickness and redeployments as well as the need for deep cleaning between cases as these were important factors highlighted in a survey of 43 UK primary PCI centres.16
While our findings suggest that there are fewer patients receiving primary PCI, we have shown that the COVID-19 pandemic does not appear to have compromised overall in-hospital clinical outcomes. Our study provides further insight regarding delays to PCI during the COVID-19 pandemic. Specifically, we found evidence of prolonged symptom-to-hospital time after the COVID-19 lockdown in England. This is consistent with the findings from a study of the management of STEMI in Hong Kong reporting a median of 318 min from symptom onset to first medical contact for seven patients since January 2020 compared with 82 min during office hours in 2018–2019 for 48 patients and a prolonged door-to-device time of 110 min compared with 84 min, respectively.4 We have furthered what is known by identifying that the delays were greatest for patients who required interhospital transfer that may relate to hospital COVID-19 policies that delay transfers between hospitals. It is possible that ambulance services have been busier and occupied with the burden of patients with suspected COVID-19, which further contributed to this delay. We also report an increase in delay from door to balloon after the lockdown, which is likely multifactorial. During the COVID-19 pandemic, UK government recommended cancellation of elective procedures,17 allowing hospital services to be restructured to divert more hospital staff and infrastructure to increase capacity for the treatment of COVID-19, reduce the exposure of individual patients and their relatives to the hospital environment and reduce the exposure of healthcare workers to asymptomatic patients with COVID-19. Furthermore, catheter laboratory staff were redeployed to other intensive care environments and that consequently may have decreased catheter lab capacity, introducing delays particularly if more than one STEMI call is activated. Furthermore, new and more intensive evaluation prior to the angiogram procedure due to activities such as chest X-ray and other assessments to ascertain the potential risk of COVID-19 infection, as well as the additional time required to ensure that staff to ‘don’ personal protective equipment may have further contributed to delays.
A few other observations can be made about the population receiving PCI before and after the COVID-19 lockdown. We observed that patients presenting after the lockdown were more likely to receive multivessel PCI. This may reflect recent data from the Complete Revascularization with Multivessel PCI for Myocardial Infarction (COMPLETE) trial that patients with STEMI and multivessel coronary artery disease had lower rates of cardiovascular death and myocardial infarction with complete compared with culprit only revascularisation.18 However, it may also relate to the operator awareness that since elective activity stopped during peak the COVID-19 outbreak, patients with bystander disease discharged with culprit only PCI may be put at a disadvantage in terms of elective access for staged complete revascularisation within 45 days, as used in COMPLETE.
An important consideration around primary PCI services for STEMI during the COVID-19 pandemic is how changes in patient’s health-seeking behaviour, health service delivery and government strategies in mitigating the impact of the pandemic may impact the characteristics of patients that receive treatment and their associated clinical outcomes. Fear of contracting COVID-19 and messages from government about self-isolation and avoiding hospitals unless absolutely necessary may result in patients not seeking or delay seeking medical attention. In the context of STEMI, this could manifest itself as increase in number of out-of-hospital cardiac arrest that has been observed in Italy and France.15 19 It is important to recognise that the patients evaluated in the current study are those that underwent primary PCI, but there may be patients who had STEMI who did not undergo PCI such as those who had an out-of-hospital cardiac arrest and died, or those that chose not seek medical attention, or those that presented late where the infarct was completed and there would be little benefit to PCI. We observed an increase in the use of prasugrel and a decrease in use of ticagrelor and clopidogrel after the lockdown. This is likely because of the changes in practice in response to the Intracoronary Stenting and Antithrombotic Regimen: Rapid Early Action for Coronary Treatment 5 trial,20 which found that death, myocardial infarction and stroke were lower among patients with prasugrel compared with ticagrelor. While not statistically significant, there were a greater proportion of patients with previous stroke in the group before compared with after the lockdown. Prasugrel is contraindicated in patients with previous stroke, and this may partly explain why there may be an increase use of prasugrel postlockdown.
Our study has several limitations. First, not all hospitals in England were included in the analysis because they did not report their PCI activity in either March or April 2020. It was important to exclude these hospitals that had so far not submitted, because the decline in PCI activity could be incorrectly attributed to failure of timely data submission rather than fewer cases. Second, in-hospital outcomes are self-reported and together with early discharge may have result in under-reporting of adverse outcomes. There is no postdischarge follow-up data, and there were missing data particularly regarding left ventricular ejection fraction and smoking status that may confound multivariate adjustment. Nevertheless, the data are subject to logical checks and assessments of internal validity at upload to NICOR. Additionally, the decline in PCI activity that we have observed is in line with that reported in Spain and the USA.8 9 Finally, there is no understanding of how local policies at each hospital may have changed as a result of the COVID-19 crisis, which may be driving the decline in procedures.
In conclusion, our national evaluation demonstrates a 43% decrease in PCI activity following the COVID-19 response lockdown. Although symptom-to-hospital and door-to-balloon times were increased after the lockdown, we did not demonstrate any differences in adverse in-hospital patient outcomes after the lockdown.
Key messages
What is already known on this subject?
Little is known about the impact of the COVID-19 pandemic on ST-elevation myocardial infarction (STEMI) rates and outcomes on a national level.
What might this study add?
Our analysis of 34 127 patients with STEMI showed a decline in STEMI procedures by 43% in April 2020 compared with the average between 2017 and 2019.
After the 23 March lockdown, both the median time from symptom-to-hospital (+15 min, p=0.004) and door-to-balloon time (+11 min, p<0.001) increased.
The in-hospital mortality rate was 4.8% before and 3.5% after the lockdown, but after adjustments, no differences were observed for in-hospital death.
How might this impact on clinical practice?
Restructuring of health services during COVID-19 has not adversely influenced in-hospital outcomes.
Acknowledgments
We are grateful for the UK government for the opportunity to analyse these data and to National Institute of Cardiovascular Outcomes Research (NICOR) and the National Health Service digital team for helping with processing and access of data and facilitating the data analysis on their servers. This work uses data provided by patients and collected by the NHS as part of their care and support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrShingKwok, @cpgale3, @NickCurzen, @dataevan, @MMamas1973
Contributors MM was responsible for the study design and concept. CSK performed the data cleaning and analysis. CSK and MM wrote the first draft of the manuscript, and all authors contributed to the writing of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval In the efforts to understand the impact of the COVID-19 pandemic on cardiology services, extraordinary government permission was obtained to evaluate anonymised records from this database through an agreement with NHS Digital. This work was endorsed by: (A) Scientific Advisory Group for Emergencies (a body responsible for ensuring timely and coordinated scientific advice is made available to decision makers to support UK cross-government decisions in the Cabinet Office Briefing Room), (B) NHS England, a public body of the Department of Health and Social Care and (C) NHS Improvement, responsible for overseeing NHS trusts. NICOR, which houses the British Cardiovascular Intervention Society registry, has support under section 251 of the NHS Act 2006 to use patient information for approved medical research without informed consent. For this rapid NHS evaluation, health data analysis was enabled under Section 254 of the Health and Social Care Act 2012.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.