Article Text

Abstract
Aims Since the beginning of the SARS-CoV-2 outbreak, hospitals reported declining numbers of patients admitted with ST-segment elevation myocardial infarction (STEMI), indicating that the pandemic might keep patients from seeking urgent medical treatment. However, data on outcomes and mortality rates are inconsistent between studies.
Methods A literature search and meta-analysis were performed on studies reporting the mortality of patients with STEMI admitted before and during the COVID-19 pandemic using PubMed, Embase and Web of Science. Additionally, prehospital and intrahospital delay times were evaluated.
Results Outcomes of a total of 50 123 patients from 10 studies were assessed. Our study revealed that, despite a significant reduction in overall admission rates of patients with STEMI during the COVID-19 pandemic (incidence rate ratio=0.789, 95% CI 0.730 to 0.852, I2=77%, p<0.01), there was no significant difference in hospital mortality (OR=1.178, 95% CI 0.926 to 1.498, I2=57%, p=0.01) compared with patients with STEMI admitted before the outbreak. Time from the onset of symptoms to first medical contact was similar (mean difference (MD)=33.4 min, 95% CI −10.2 to 77.1, I2=88%, p<0.01) while door-to-balloon time was significantly prolonged in those presenting during the pandemic (MD=7.3 min, 95% CI 3.0 to 11.7, I2=95%, p<0.01).
Conclusion The significant reduction in admission of patients with STEMI was not associated with a significant increase of hospital mortality rates. The causes for reduced incidence rates remain speculative. However, the analysed data indicate that acute and timely medical care of these patients has been maintained during the pandemic in most countries. Long-term data on mortality have yet to be determined.
- acute coronary syndrome
- epidemiology
- meta-analysis
- systematic reviews as topic
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
Since the beginning of the SARS-CoV-2 pandemic, there have been many reports on cardiac collateral damage.1 2 Apart from the direct detrimental effects of SARS-CoV-2 infection on patients with heart disease, it has been suggested that the pandemic keeps patients from seeking and receiving urgent medical advice in the case of an acute cardiac event, potentially deteriorating their prognosis.3 4 For example, the number of patients suffering from acute cardiac ischaemia including patients with ST-segment elevation myocardial infarction (STEMI) dropped significantly during the COVID-19 outbreak.4 5 Presumably, there are a variety of causes that underlie this phenomenon, the most important of which might be the reluctance to engage with medical services out of fear of getting infected while in the hospital.1 It has been suggested that iatrophobia might prolong the time from the onset of symptoms to first medical contact (FMC), leading to adverse outcomes of patients with STEMI admitted during the pandemic.6 7 To date, there have been several reports from around the world observing higher serum troponin levels, worsened left ventricular systolic function and a higher intracoronary thrombotic burden in patients with STEMI admitted during the pandemic.8 9 However, evidence on detrimental effects of the pandemic and restrictions of public life on the in-hospital outcome of patients with STEMI is limited. Most importantly, the effect on mortality rates has not been clarified, since reports are discrepant.5 7 10 Therefore, we performed a meta-analysis to assess the mortality of patients with STEMI admitted during the COVID-19 pandemic.
Methods
Data sources and study selection
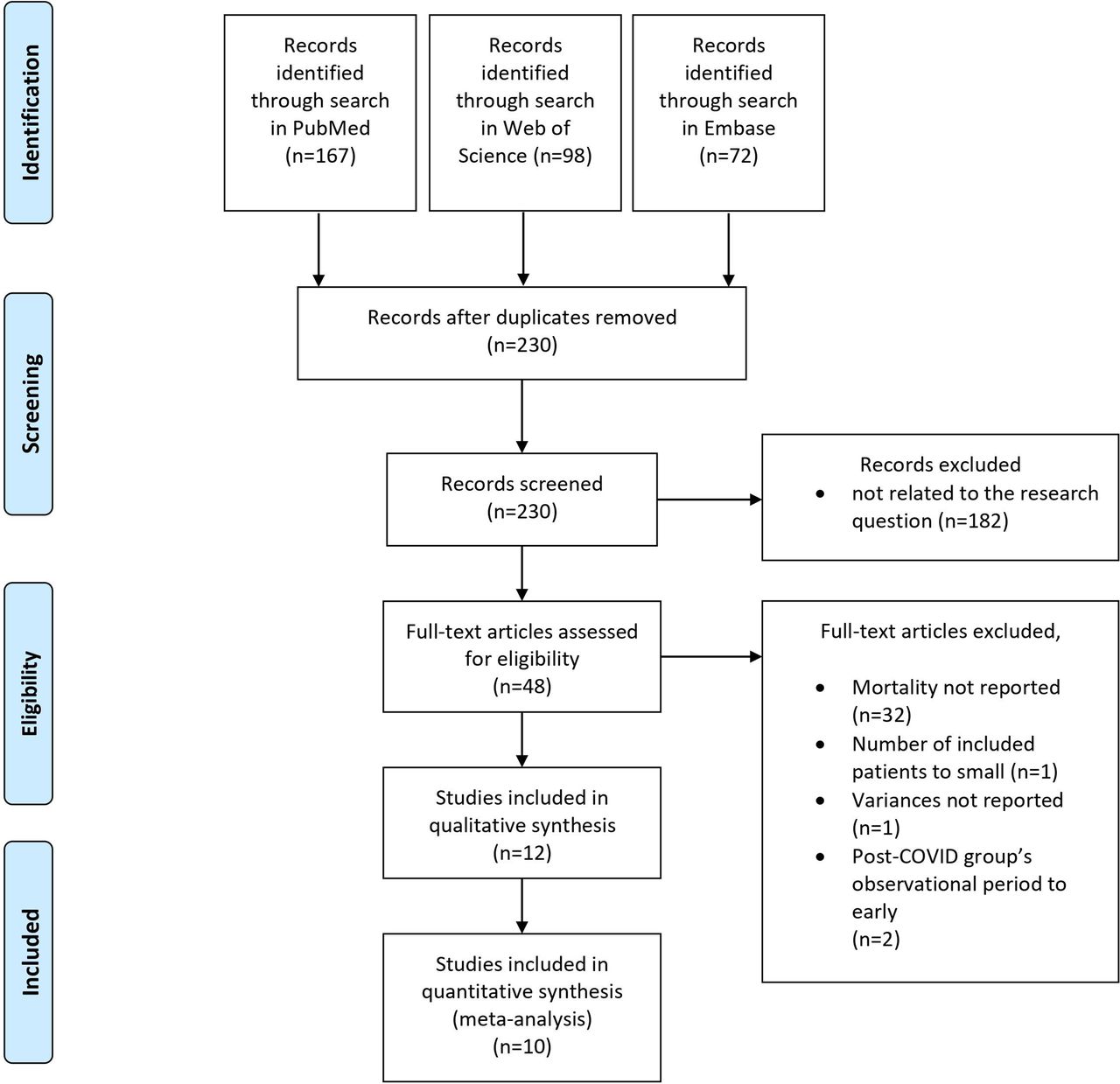
A comprehensive literature search was performed through PubMed, Embase and Web of Science from the first reports of the novel coronavirus (SARS-CoV-2) in December 2019 up to August 2020 using the keywords ‘COVID’ and ‘STEMI’.11 We looked for observational studies, case reports and short communications in English language. We included studies reporting the number of STEMI admissions and the corresponding mortality rates. Every included study defined a specific date which marked the beginning of the COVID pandemic. We adhered to those definitions. Patients with STEMI admitted before the COVID outbreak were defined as the pre-COVID-19 group, and patients admitted during the pandemic were defined as the post-COVID-19 group. Time frames are detailed in online supplemental table 1. Studies were eliminated when the post-COVID-19 group’s observational period started before the first reported patient who was COVID-19 positive in the study site’s country. We excluded conference abstracts, case reports, review articles, posters, manuscripts without reported means/SDs or without medians/IQRs and studies with a sample size <10 patients in either the pre-COVID-19 or post-COVID-19 group. The flow chart of the literature search strategy is presented in figure 1.
Supplemental material

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. Out of 337 identified studies and after application of the inclusion and exclusion criteria, 10 studies were included in the quantitative synthesis.
Data extraction and study quality
Two investigators independently reviewed all the articles, selected eligible studies and extracted valuable data. In case of any discrepancies, a third reviewer made the final decision.
Data extraction used standardised extraction forms including information on authors, site, country, publication year, number of patients with STEMI per group, peak cardiac troponin serum concentration, echocardiographic left ventricular ejection fraction, time from the onset of symptoms to FMC (including time from the onset of symptoms to FMC, time from the onset of symptoms to diagnosis, time from the onset of symptoms to hospital), door-to-balloon (DTB) time (including DTB time, door-to-device time, door-to-reperfusion time, in-hospital time to reperfusion), hospital mortality (including in-hospital mortality, 7-day mortality and 10-day mortality) and baseline characteristics (age, gender, number of patients with arterial hypertension, diabetes mellitus, dyslipidaemia, known coronary artery disease, number of current or former smokers).
The study quality was assessed as detailed by the National Institutes of Health (NIH) Quality Assessment Tool and studies were rated as being of either ‘good’, ‘fair’ or ‘poor’ quality.12
As all analyses were based on previous studies, neither patient consent nor ethical committee approval was required for our study. This meta-analysis has been preregistered at PROSPERO (CRD42020207153). Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research
Statistical analysis
Data were collected in a Microsoft Excel spreadsheet and outcome measures were calculated. If in the included studies only median values with IQR were reported, means and SDs were calculated by making use of the BoxCox method.13 Meta-analyses were done both on binary and on continuous endpoints. The studies are presented by publication year and data are reported as (1) absolute frequencies and/or percentages in case of binary endpoints and (2) as mean± SD in case of continuous endpoints. Additionally, a meta-analysis was performed for the incidence rate ratio (IRR) for STEMI admissions. The random effects model was used to combine the estimates from the different studies. This was preferred over the fixed effects model as moderate or severe heterogeneity was expected in the effect sizes in some endpoints. Moreover, the random effects model gives a more conservative estimate. For binary endpoints, the Mantel-Haenszel method was used and the OR including 95% CI is reported as effect measure. For continuous endpoints, the inverse variance method was used and the mean difference (MD) including 95% CI is reported as an effect measure. For the assessment of heterogeneity among studies, the statistical characteristic I2 and the p value of a χ2 test (the established significance level of <0.05 suggests heterogeneity) are reported. Forest plots are used for graphical representation of results, which included all individual results of the considered studies separately, as well as overall results. Additionally, funnel plots were created to evaluate the risk of publication bias. Meta-analyses were performed using the meta package in the statistical software R V.3.5.1. All tests were two tailed, and results with a p value <0.05 were considered statistically significant. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement was applied in this study.14
Results
Literature search and quality assessment
Based on our search strategy, 337 studies were initially identified from PubMed, Embase and Web of Science databases. After removal of 107 duplicates and exclusion of 182 studies which were not related to the research question, 48 articles were assessed for eligibility. In 32 studies, mortality rates were not reported. In two studies, the observational period of the post-COVID-19 group started before the first patient who was COVID-19 positive was reported in the country of the study’s origin. In one report, the number of included patients did not meet our prespecified criterion and, in one study, variances were not reported. Out of the 12 remaining studies, 10 were included in the quantitative synthesis (figure 1; online supplemental table 1).1 5 7 8 10 15–19 Based on the NIH Study Quality Assessment Tool, one study was of ‘fair’ quality whereas nine studies had ‘good’ methodical quality (table 1).
Summary of included studies and baseline characteristics
Baseline characteristics
A total of 50 123 patients with STEMI were enrolled from the various studies, including 35 262 patients in the pre-COVID-19 group and 14 861 patients in the post-COVID-19 group. Evaluation of baseline characteristics showed that the average age was 64.2 years with 74.3% of patients being male. 19.9% of patients had diabetes mellitus, 52.3% had arterial hypertension, 45.5% had dyslipidaemia, 34.6% were either active smokers or had a history of smoking and 17.9% had known coronary artery disease (weighted arithmetic means). There were no significant differences in baseline characteristics between the two groups in our meta-analysis. Detailed information on baseline population characteristics is listed in table 1 and corresponding forest plots (including CIs to assess the significance of results) and funnel plots are shown in the online supplemental figures 1–7.
Rate of admissions, assessment of treatment delays and mortality
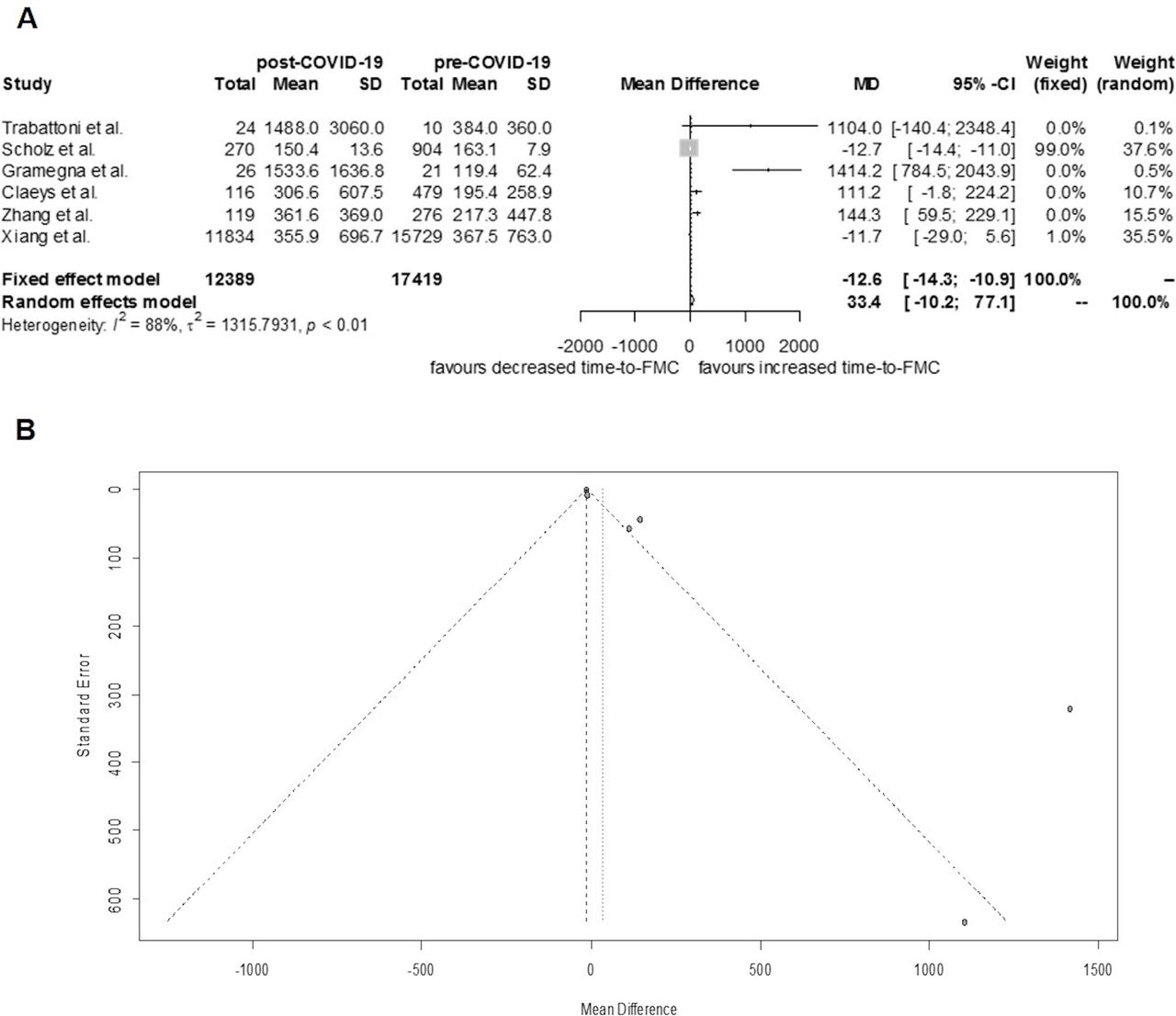
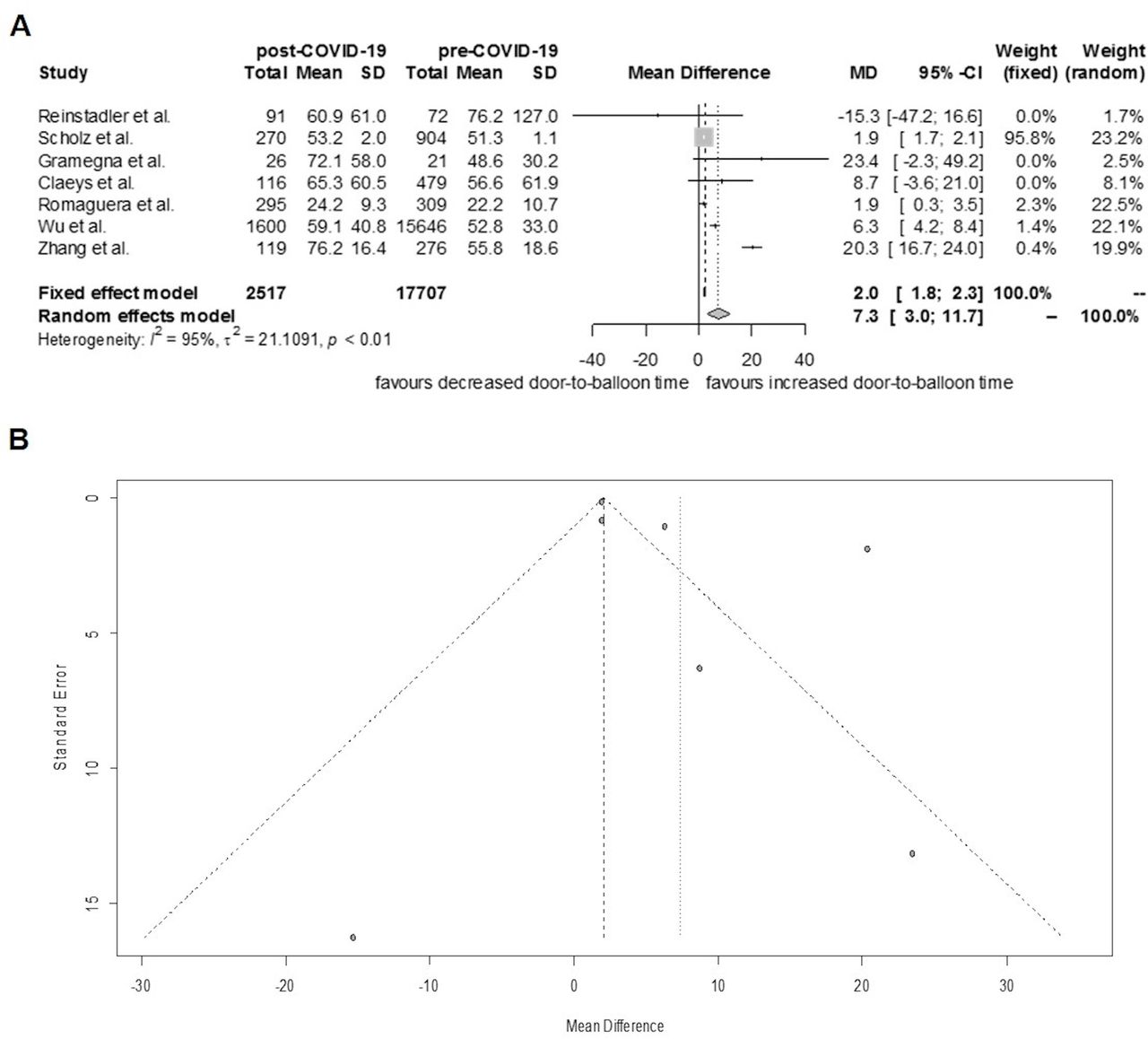
Admission rates of patients with STEMI were reported in all of the included studies. In the pre-COVID-19 group, the number of daily admissions was 11.0. However, in the post-COVID-19 group, only 8.2 patients with STEMI were admitted per day, equalling a reduction of 25.5%. Thus, admissions due to STEMI were significantly lower in times of the COVID-19 pandemic (IRR=0.789, 95% CI 0.730 to 0.852, I2=77%, p<0.01; figure 2). Times from symptom onset to FMC (in minutes) were reported in six studies and did not differ significantly between the post-COVID-19 and the pre-COVID-19 group (MD=33.4, 95% CI −10.2 to 77.1, I²=88%, p<0.01; figure 3). By contrast, assessment of the DTB time (in minutes), which was reported in seven studies, was significantly prolonged in the post-COVID-19 group compared with the pre-COVID-19 group (MD 7.3, 95% CI 3.0 to 11.7, I²=95%, p<0.01; figure 4). All included studies assessed the in-hospital mortality of patients with STEMI admitted before and during the COVID-19 outbreak. It was shown that mortality did not differ significantly between the post-COVID-19 (1957 out of 35 120 patients) and pre-COVID-19 groups (717 out of 14 805 patients) (OR=1.178, 95% CI 0.926 to 1.498, I2=57%, p=0.01; figure 5).

Forest and funnel plots—incidence rate of admissions of patients with ST-segment elevation myocardial infarction (STEMI). In times of COVID-19, significantly less patients with STEMI were admitted to hospital. (A) Forest plot. (B) Funnel plot.

Forest and funnel plots—time from symptom onset to first medical contact. There was no significant difference in the time from symptom onset to first medical contact in both groups. (A) Forest plot. (B) Funnel plot. FMC, first medical contact; MD, mean difference.
Forest and funnel plots—door-to-balloon time. Door-to-balloon time was significantly prolonged in the post-COVID-19 group. (A) Forest plot. (B) Funnel plot. MD, mean difference.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest and funnel plots—in-hospital mortality of patients with ST-segment elevation myocardial infarction (STEMI). There was no significant difference in in-hospital mortality between the pre-COVID-19 and post-COVID-19 groups. (A) Forest plot. (B) Funnel plot. IRR, incidence rate ratio.
Discussion
This is the first meta-analysis on the incidence of STEMI admissions during the COVID-19 pandemic with a focus on prehospital and intrahospital delay times and mortality rate. Overall, a significant decline in STEMI admissions has been observed. Time from the onset of symptoms to FMC did not differ significantly between patients admitted before and during the COVID-19 pandemic. However, DTB time, which represents in-hospital treatment processes of patients with STEMI, was significantly prolonged. However, the in-hospital mortality did not increase.
Incidence of STEMI admissions
Spread of the novel coronavirus (SARS-CoV-2) led to a rapidly expanding global pandemic with substantial regional differences in the number of infected. Apart from the direct detrimental effects of SARS-CoV-2 on the health and lives of many people, physicians reported an increasing SARS-CoV-2-related medical undersupply for patients and soon warned against potential collateral damage.20 21 In April 2020, the phenomenon of declining admission numbers of patients with heart diseases was first published and numerous observations from around the globe reporting on the drop in STEMI admissions followed.2–4 7 16 22–24 In contrast to the majority of reports, some studies observed an increase in patients admitted with STEMI.8 15 Our meta-analysis indicates that overall STEMI admissions significantly decreased. Healthcare professionals suggested various reasons to contribute to the phenomenon of missing STEMIs. Apart from framing issues,5 25 misled altruistic behaviour to not overburden the healthcare system,26 stay-at-home orders, as well as social containment mandates,19 iatrophobia due to the fear of SARS-CoV-2 contagion is suspected to be the main cause.26 27
Interestingly, Scholz et al observed that the way patients with STEMI were admitted to hospital influenced the change in admission rates. They reported that for Germany, admissions of patients with self-referral decreased, while the rate of patients with STEMI admitted by emergency medical services did not change significantly.10 This suggests that patient-related rather than system-related factors, such as iatrophobia and framing issues, contributed to the decrease in STEMI admissions. However, even though admissions by the emergency services did not decrease in this report, healthcare professionals can be misled. Custodis et al reported a 48-year-old man, initially treated for suspected COVID-19, actually died from acute myocardial ischaemia, as confirmed by his autopsy.25 This highlights the importance of educating patients as well as professionals on perceiving cardiovascular symptoms and taking them seriously, especially to guard against the factors framing and misled altruistic behaviour. Regarding the effect of social containment measures on admissions of patients with STEMI, Wu et al showed for England that after social lockdown has been implemented the number of admissions significantly dropped, but after containment measures have been lifted, admission numbers in part recovered, underscoring its potential deteriorating effect on STEMI care.19 Iatrophobia, which is defined as the fear of physicians, medical care or the medical care system, and the associated fear of getting infected with COVID-19 have intensively been discussed to be one of the main reasons keeping patients with STEMI from seeking medical attention.26 27 Several case reports showed that patients with STEMI who delayed their admission out of fear of getting infected suffered from complications and adverse outcomes.28 However, at present, a comprehensive study on the impact of fear of COVID-19 in patients with acute coronary syndrome or STEMI is missing.
Furthermore, even if unlikely, it remains possible that the reduction in incidence of STEMI admissions can in part be attributed to less exposure to STEMI triggers, such as lower physical stress during quarantine. Additionally, some studies suspected an association between declining STEMI numbers and reduction in air pollution.16
From the few current reports on an increased number of patients with STEMI, we can still only speculate on the reasons.8 15 However, since these studies stemmed from hospitals in COVID-19 hot spots, it remains possible that either a SARS-CoV-2 infection itself or an increase in stress contributed to this finding.
Time to FMC
Several studies assessing admission rates of patients suffering from an acute cardiac event during the COVID-19 pandemic reported that times from the onset of typical symptoms of myocardial ischaemia to FMC significantly increased.15 23 Contrary to this, our meta-analysis revealed that, on a global scale, time to FMC did not differ significantly between the pre-COVID-19 and post-COVID-19 groups. This might be related to regional differences. For instance, the Hebei Province was one of four provinces (Hebei, Hubei, Beijing, Tianjin) in China to maintain the national state of emergency the longest, thereby potentially contributing to a longer time to FMC.18 Furthermore, studies from medical centres located in COVID-19 hot spots such as Milan, Italy, reported the most delayed FMC during the COVID-19 outbreak, suggesting a huge impact of local factors, such as fear, lockdown and possibly COVID-19-related structural deficits of the emergency care system.8 15 Remarkably, the three studies included in our meta-analysis on time to FMC observing the largest prolonging effect of COVID-19 on FMC all derived from single centres, possibly accentuating local influences.8 15 18 Inclusion of multicentre studies and reports from regions less impacted by the COVID-19 pandemic (such as Germany) in our meta-analysis possibly levelled the aforementioned effects, giving a more uniform picture of the preclinical delay times during the COVID-19 outbreak.
Soon after the problem of diminishing cardiovascular emergency patients emerged, healthcare professionals rapidly implemented countermeasures, such as national campaigns to raise public awareness with regard to symptoms of myocardial ischaemia.15 This might have contributed to thwarting the trend of both the decline in STEMI admissions as well as FMC times, even in epicentres of the COVID-19 pandemic. This substantiates the need for ongoing public messaging about the importance of seeking urgent medical attention in the presence of heart attack symptoms.15 18
DTB time
Another important criterion influencing the outcome of patients with STEMI is the length of time needed in hospital to treat the culprit lesion by reopening the occluded vessel, namely the door-to-wire, DTB or door-to-reperfusion time.6 Our results show that the DTB time was significantly prolonged in the post-COVID-19 group. This is supposedly caused by the time-consuming but necessary adaption of emergency processes for patients in whom the COVID-19 status is unknown, in order to prevent the in-hospital spread of the virus.29
Mortality
Whether the observation of reduced STEMI admissions during the COVID-19 pandemic and, to some extent, potentially limited and deficient medical supply had an impact on mortality has not been comprehensively evaluated. Several studies have reported that patients with STEMI admitted during the COVID-19 outbreak were in worse condition than those admitted before the pandemic. It has been observed that during the COVID-19 pandemic, patients with STEMI had higher serum troponin levels,8 a lower left ventricular ejection fraction,9 a higher intracoronary thrombotic burden,1 more in-hospital complications and a higher mortality.5 However, these data are highly inconsistent between studies. Regarding the studies included in our meta-analysis, in-hospital mortality of patients with STEMI was only increased in reports from COVID-19 epicentres (Italy; China, Hubei Province).5 7 It appears reasonable to suggest that factors which might deteriorate the outcome of patients with STEMI during a pandemic, such as iatrophobia, framing issues, system delay times and social containment measures, are more pronounced in pandemic epicentres, thereby potentially contributing to a local increase in mortality in COVID-19 hot spots. However, our results suggest that on a more global scale the in-hospital mortality of the post-COVID-19 group is not significantly higher than before the pandemic, which might be related to the rapid implementation of information campaigns and quick optimisation of prehospital and in-hospital procedures by the medical community and cardiology professionals. Our meta-analysis is also in line with the results of a recently published large multicentre registry study, who observed a significant decline in STEMI admissions during lockdown in France, with unchanged times from symptom onset to FMC, and increases in in-hospital delays, but no significant difference in in-hospital deaths.30
Nevertheless, it remains possible that the observational period is still too short to detect a significant difference in mortality. As a consequence, prospective studies comprising a longer follow-up period are necessary to further comment on this issue.
Limitations
As this is a meta-analysis of studies reporting on the mortality of patients with STEMI during the COVID-19 outbreak, it inherently has limitations. As per our prespecified study protocol, data on peak serum troponin levels and left ventricular ejection fraction were extracted but were not sufficient to be included in the analysis and are shown in the supplementary material instead (online supplemental figures 8 and 9). Most studies reported skewed data on time to FMC and DTB time, which has been adjusted appropriately.13 Nonetheless, it remains possible that the BoxCox method used for this purpose might be imprecise in calculating the SD in some cases, which is innate to the method.13 However, to give an unbiased insight on the impact of COVID-19 on patients with STEMI on a global scale, all relevant data available, including skewed data, published until 31 August 2020 were included. Consequently, regarding the differences in study size, this inevitably influences the weighting of the studies, which is inherent to meta-analyses.
Conclusion
This is the first meta-analysis on patients with STEMI admitted during the COVID-19 outbreak, suggesting that in-hospital mortality is not deteriorated by the pandemic. This might be attributable to the rapid implementation of countermeasures undertaken by the healthcare professionals. Prospective studies with a longer follow-up period are needed to further assess the outcomes of patients with STEMI.
Key messages
What is already known on this subject?
Since the beginning of the COVID-19 pandemic, there have been reports on declining numbers of admissions of patients with ST-segment elevation myocardial infarction (STEMI). Healthcare professionals suggest that the outbreak causes cardiac collateral damage, which can potentially deteriorate the patients’ prognosis. However, published data on the outcome and mortality of patients with STEMI are inconsistent between studies.
What might this study add?
This is the first meta-analysis on delay times and hospital mortality of patients with STEMI admitted during the COVID-19 pandemic. Our results suggest that on a global scale, the COVID-19 outbreak was not associated with in-hospital excess mortality of patients with STEMI. Moreover, timely medical care, as measured by the time from symptom onset to first medical contact, has been maintained in most countries. In-hospital treatment processes were significantly prolonged, which is possibly related to the necessary adaptation of emergency processes to protect against COVID-19.
How might this impact on clinical practice?
This study highlights that despite the worldwide phenomenon of missing admissions of patients with STEMI during the COVID-19 pandemic, adequate medical supply has been maintained in most countries. This is possibly related to the rapid implementation of countermeasures, such as information campaigns, and adaptation of emergency processes. Efforts must be maintained to minimise the cardiac collateral damage.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MR and AI had the idea for and designed the study and had full access to all the data. MR and MB collected the data. JD performed the statistical analysis. MR, CW and LS mainly wrote the manuscript with support from AI and KT. AI and WR were mainly responsible for interpretation of the data and supervised the project. All authors provided critical feedback and contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.