Article Text

Abstract
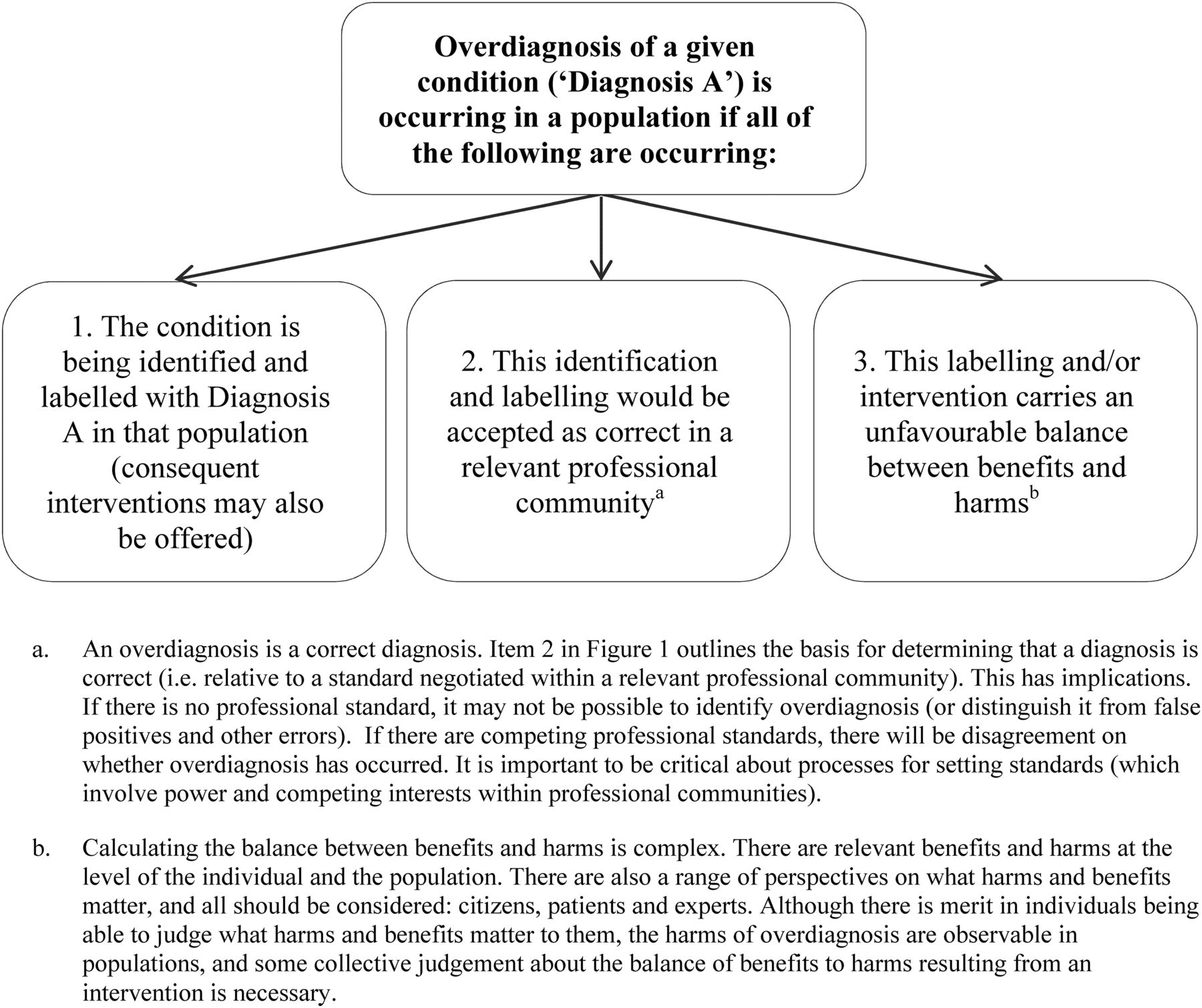
Overdiagnosis is an emerging problem in health policy and practice: we address its definition and ethical implications. We argue that the definition of overdiagnosis should be expressed at the level of populations. Consider a condition prevalent in a population, customarily labelled with diagnosis A. We propose that overdiagnosis is occurring in respect of that condition in that population when (1) the condition is being identified and labelled with diagnosis A in that population (consequent interventions may also be offered); (2) this identification and labelling would be accepted as correct in a relevant professional community; but (3) the resulting label and/or intervention carries an unfavourable balance between benefits and harms. We identify challenges in determining and weighting relevant harms, then propose three central ethical considerations in overdiagnosis: the extent of harm done, whether harm is avoidable and whether the primary goal of the actor/s concerned is to benefit themselves or the patient, citizen or society. This distinguishes predatory (avoidable, self-benefiting), misdirected (avoidable, other-benefiting) and tragic (unavoidable, other-benefiting) overdiagnosis; the degree of harm moderates the justifiability of each type. We end with four normative challenges: (1) methods for adjudicating between professional standards and identifying relevant harms and benefits should be procedurally just; (2) individuals, organisations and states are differently responsible for addressing overdiagnosis; (3) overdiagnosis is a matter for distributive justice: the burdens of both overdiagnosis and its prevention could fall on the least-well-off; and (4) communicating about overdiagnosis risks harming those unaware that they may have been overdiagnosed. These challenges will need to be addressed as the field develops.
- Public Health Ethics
- Philosophy of Medicine
Statistics from Altmetric.com
Overdiagnosis occurs when someone is diagnosed with a disease that would not have harmed them, often as a result of undergoing screening, and evidence is emerging that many people are overdiagnosed and labelled unnecessarily across a range of conditions.1
[Cancer] overdiagnosis refers to the detection of cancers that, in the absence of screening, would not present symptomatically.2
Overdiagnosis is commonly defined as diagnosing a person without symptoms with a disease that will never cause symptoms or death during the person's lifetime.3
[Cancer] overdiagnosis is the detection of cancers that would not have been identified clinically in someone's remaining lifetime.4
Narrowly defined, overdiagnosis occurs when people without symptoms are diagnosed with a disease that ultimately will not cause them to experience symptoms or early death. More broadly defined, overdiagnosis refers to the related problems of overmedicalization and subsequent overtreatment, diagnosis creep, shifting thresholds, and disease mongering, all processes helping to reclassify healthy people with mild problems or at low risk as sick.5
Overdiagnosis, the detection and diagnosis of a condition that would not go on to cause symptoms or death in the patient's lifetime, is an inevitable harm of screening… A patient who is overdiagnosed cannot benefit from the diagnosis or treatment but can only be harmed…6
Overdiagnosis is the term used when a condition is diagnosed that would otherwise not go on to cause symptoms or death…[Cancer] overdiagnosis should not be confused with false-positive results, that is, a positive test in an individual who is subsequently recognized not to have cancer. By contrast, an overdiagnosed patient [with cancer] has a tumor that fulfils the pathological criteria for cancer.7
Overdiagnosis is a relatively new, rapidly growing field of inquiry; its foundations are still being established.5 In our earlier work, we noted (as others have done)3 that there are many ‘over’ terms, including overdetection, overtreatment, overutilisation and (over) medicalisation; there has been a tendency in the literature to use the label ‘overdiagnosis’ to refer to all of these.8 Contra this, we and others have argued for the distinctness of these concepts, and for a narrower conception of overdiagnosis.8 ,9 Here, we focus on the narrow, not the broad, meaning.i
We contribute to the overdiagnosis literature by answering two interrelated questions: (1) How should overdiagnosis be defined? (2) What are the ethical implications of overdiagnosis?
Defining overdiagnosis
Most articles about overdiagnosis assert a brief working definition, then get on with the task at hand, which is usually to (1) quantify overdiagnosis, (2) determine the consequences of overdiagnosis and/or (3) describe the causal pathways by which overdiagnosis occurs. Considerable work has been done on causal pathways in particular. These include expanded disease definitions, the creation of ‘pre-diseases’, increasingly sensitive tests, incidental test findings of uncertain significance, more frequent and intensive testing, commercial interests that seek to expand markets for treatments, and increasing acceptance of risk reduction as an indicator of effectiveness of intervention.3 ,5 ,9–11
Few authors have focused on defining overdiagnosis. Marcus et al2 (who describe cancer overdiagnosis as the detection of cancers that, in the absence of screening, would not present symptomatically) recently published a ‘tumour–patient classification’ of cancer overdiagnosis, with the goal of differentiating ways in which cancer overdiagnosis occurs (table 1). Wendy Rogers and Yishai Mintzker have distinguished between misclassification overdiagnosis (occurring when a diagnostic threshold is set such that non-harmful disease is often diagnosed) and maldetection diagnosis (arising from the inability to distinguish between harmful and non-harmful cases of the index disease).12 Bjørn Hofmann has published on both the conceptualisation of overdiagnosis and its relationship to medicalisation.3 ,9 He proposed a new nomenclature to replace the term overdiagnosis, which has not yet been taken up in the literature, perhaps partly because of its complexity.3 These typologies each make a contribution; in our view, the literature still lacks a general and well-justified definition of overdiagnosis.
The tumour–patient classification of cancer overdiagnosis2
We began by quoting the brief definitions asserted by leaders in the field. These demonstrate a rough meaning-in-use for overdiagnosis: ‘a correct diagnosis that does not benefit’. This suggests that correctness and failure to benefit are necessary features of any instance of overdiagnosis, and thus that defining overdiagnosis will require (1) distinguishing correct from incorrect diagnoses and (2) determining what should count as a benefit. We will consider each of these in the following sections, but begin with two observations.
First, overdiagnosis does not only occur in the clinic. In particular, as testing, genetic sequencing and biomonitoring become increasingly available and networked, more citizens will detect and diagnose health risks or diseases for themselves, sometimes assisted by commercial interests. Second, it seems that overdiagnosis can occur only when something is identified as a health-related problem. So when doctors say ‘that mole looks worrying’ or ‘you are clinically depressed’ or ‘I'll refer you to the specialist’ or ‘we should cut that out’ or ‘you should take this medication’, overdiagnosis could occur, but not when doctors advise that there is no problem. Relatedly, the offering of an intervention should be considered a probable but non-necessary component of an overdiagnosis for two reasons. A small amount of benefit may accrue simply from being diagnosed (eg, the psychosocial benefit of ‘knowing what's wrong’), but diagnoses benefit most by attracting interventions, such as treatment for the experienced problem. Conversely, diagnosis does not always attract an intervention—for example, when a clinician labels a disease but has no effective treatment available to use—and it seems important that these instances are open to being classed as overdiagnosis.
This suggests a revision of the definition, from ‘a correct diagnosis that does not benefit’ to this: overdiagnosis occurs when a health-related problem is correctly identified and labelled (an intervention may also be offered) but this does not benefit.
Overdiagnosis is ‘correct’ diagnosis
If overdiagnosis must be correct, then it must be possible to distinguish correct from incorrect diagnosis. The question is how this should be done. In the overdiagnosis literature, authors frequently rely on a correspondence standard for this task.4 ,5 ,7 A correspondence standard implies that a correct judgement or action corresponds to material or biological reality: a cancer diagnosis, for example, is correct when a person ‘truly has cancer’ and the resulting treatment is correct when a cancer ‘really goes into remission’. These assumptions are generally implicit rather than being argued out, but they align loosely with a materialist or objectivist conception of disease and diagnosis in the philosophy of science.13
In our view, noticing and modifying these assumptions is vital to the development of thinking about overdiagnosis. The arguments for softening a strong objectivist model of disease are well-worked.13 Throughout history, diagnostic judgements and actions thought to correspond to material reality have repeatedly arisen, become accepted and then been abandoned as the seat of disease was again reconceptualised.14 Diabetes, for example, was understood to be a disorder of carbohydrate metabolism, then a pancreatic dysfunction, then a problem of glucose control and regulation; the corresponding diagnostic tests—urinalysis, then oral glucose tolerance tests, then haemoglobin A1C titres—reflected and shaped understandings of diabetes as a condition.15 ,16 Unitary conceptions of diseases have given way to diverse pathological conceptions (eg, in cancer). Many overdiagnosis-related problems stem from the continuous nature of pathological criteria, such that thresholds for distinguishing disease from non-disease are a matter for negotiation and interpretation.3 Conceptions of ‘correct’ treatment and of how treatments work on disease biology have shifted radically: consider starving therapy, then pancreatic extracts, then insulin and lifestyle therapy for diabetes.15 ,16 And treatments considered ‘correct’ are never universally effective (so their effectiveness cannot be used as a reliable marker of their correctness).17 All of this makes it improbable that even present conceptions of disease correspond exactly to an underlying reality: history suggests that contemporary diagnoses and treatments will be overturned in future.ii
Our preferred alternative: a professional community standard
For these reasons, we prefer a professional community standard for distinguishing correct from incorrect diagnosis.19 By this we mean the following: ‘correct’ diagnoses are those that are accepted as correct within a relevant professional community. This recognises that medical and scientific expertise is important when adjudicating between correctness and incorrectness, and that health-related judgements and actions that occur outside the clinic can reasonably be judged against the knowledge of relevant professional communities. However, it also acknowledges that standards for determining correct action are actively produced by members of a professional community, meaning that evidence is necessary but never sufficient to the task.
Sometimes, the active creation of ‘correct’ diagnoses is obvious: for example, in the negotiation of the relatively new diagnosis of pre-cancers, such as ductal carcinoma in situ (DCIS) or high- and low-grade squamous intraepithelial lesion.20 ,21 However, this also occurs more subtly. For example, the shift from morphological criteria to immunophenotyping as the basis for classifying and diagnosing leukaemia and lymphomas involved active creation and coordination of equivalences between seemingly incommensurable clinical understandings, pathological descriptions, qualitative and quantitative diagnostic criteria, and professional interests in an otherwise clearly defined clinical domain.22 ,23
Professions are communities of practice; members of these communities produce and instantiate the best available standard for practice at any given time. Explicit standard production is preferable because this requires greater justification and accountability from participants. But standards can also develop implicitly, first instantiated through practice routines and then tacitly shared. A new test or drug, for example, can enter everyday practice through individual practitioners and their networks, without any formal endorsement from expert bodies.
These observations again revise the definition of overdiagnosis to the following. Overdiagnosis occurs when a health-related problem is identified and labelled (an intervention may also be offered), this identification and labelling would be accepted as correct in a relevant professional community, but it does not benefit.
A professional community standard: implications
There are three implications of recognising that the standard for ‘correct’ judgements and actions is negotiated intersubjectively in professional communities.
First, overdiagnosis cannot be identified until a standard exists. There are several consequences of this. One is that the line between overdiagnosis and error, particularly false positives, may be less clear than is usually assumed. To date, the idea that overdiagnoses are correct and false positives incorrect has been central to the conception of overdiagnosis. But a tacit or explicit standard must exist, and be recognisable, for correct judgements and actions to be distinguished from incorrect ones. This means that, particularly in the earliest days of a practice or technology before standards are established, overdiagnosis and false positives may be indistinguishable.
This is further complicated by conflict between professionals. Often, subspecialties or different disciplines hold competing understandings of conditions. Take peripheral vascular disease (atherosclerosis of the lower limb), which pathologists diagnose by narrow calcified vessel walls, cardiologists by low blood pressure in the legs, physiotherapists by the presence of claudication and radiologists by narrowed vessels in a contrast study.24 ,25 Each discipline focuses on a different object—vessel walls, blood pressure, pain and so on—demonstrating that standards are acts of coordination that somehow fold these different objects into one disease. If we acknowledge that the line separating ‘correct’ from ‘incorrect’ is negotiated within professional communities, and that different communities may work from quite different conceptions of conditions, it becomes apparent that disagreements about the prevalence of overdiagnosis may sometimes be disagreements within or between professional communities about what the reference standard for identifying a condition should be.
Second, acknowledging that standards are produced in and by professional communities forces attention to the process by which they are developed, and so provides better analytic tools for dealing with disagreement over overdiagnosis. Recall the example of peripheral vascular disease. Advocates of a correspondence standard may insist that science should be able to determine which definition is truly ‘correct’, and thus dismiss the other partial or ‘incorrect’ accounts. But this is of limited use as all disciplines will have scientific cases to make. The professional community standard encourages us to ask how competing standards are arrived at and by whom, and to understand disagreements about overdiagnosis as the result of differing processes of production, rather than as a result of one group being ‘right’ and the others ‘wrong’.
The third implication follows: the professional community conception is the best basis for considering the vested interests, political pressures, and social norms and conventions that have been key concerns for those studying the drivers of overdiagnosis.26
What conception of benefit (and harm) should we employ?
Having considered the standard for ‘correctness’, we now move to the related issues of benefit and harm. Benefit or harm are good and bad consequences, respectively, so are unavoidably normative. This means we cannot have a purely descriptive conception of overdiagnosis: normativity is built into the concept. Benefits and harms are not only physical: they can be of other kinds. Russell Harris and colleagues, for example, divide the harms of cancer screening into physical effects, psychological effects, financial strain and opportunity costs.27
Benefit and harm in individuals and populations
The definitions quoted at the beginning of this paper all contain a particular implicit conception of non-benefit: the condition diagnosed would not have caused symptoms in the individual in their lifetime, such that there is no benefit to be had from the diagnosis. These definitions implicitly work at the level of the individual. They assume a (perhaps hypothetical) patient and doctor, and attempt to point to situations in which that doctor overdiagnoses that patient. We propose, in contrast, that because overdiagnosis is almost exclusively observable at the level of populations, and non-observable at the level of the individual, it should be defined at the level of populations. This move is also made implicitly in Hofmann's nomenclature, although it is not explicitly defended in those terms.3
This issue can be usefully considered via Widdows and Cordell's distinction between aggregative and corporate communal goods.28 ‘Aggregative communal goods’ are constituted of goods that attach to individuals: these individual goods aggregate to a communal good. In contrast, corporate goods attach to whole communities, emerging only as a property of that community. An increase in average lifespan or a decrease in cancer incidence are aggregative communal goods; a universal healthcare system is a corporate communal good.
Overdiagnosis occurs in individuals, and these instances aggregate in populations. Critically, overdiagnosis can only be observed statistically, estimated via studies of whole populations. If a cancer screening programme increases the incidence of early-stage disease without reducing the incidence of late-stage disease, for example, overdiagnosis will be statistically inferred. This may be occurring because there is no treatment available, because treatment is not beneficial or (as in Marcus' tumour A and tumour B types)2 because screening-identified conditions would have remained unsymptomatic, so there was no benefit of detection to outweigh the resulting harmful labelling and intervention. The screening programme is harming, or in the best case failing to benefit, individuals. These individual cases aggregate to the observable population-level rate of overdiagnosis, but the individual cases can rarely be identified.3
Imagine two asymptomatic women diagnosed with early-stage invasive breast cancer following mammographic screening. Both have a mastectomy. For each, the harm of removing a breast is readily observable. However, the benefit for each woman cannot be known because it is unknown how each woman's life would have proceeded without the diagnosis and surgery. Perhaps one of those women was going to develop life-threatening invasive breast cancer and the other was not. Perhaps, if left unscreened, one of these women would have died of a heart attack within 5 years (before being diagnosed with breast cancer) but the other would have developed life-threatening invasive cancer in 10 years. In either of these scenarios, one woman has likely been overdiagnosed, and the other not. However, this cannot be known for the individual women. This is what Hofmann describes as the problem of counterfactuality: that it is impossible to know what would have happened if a screened person had not been screened.3 Hofmann is correct about counterfactuality at an individual level; we would add to his observation, however, that each woman represents a case of early-stage breast cancer in a population, and their cases can be aggregated with others to estimate overdiagnosis in that population.
This pattern can be seen across a range of conditions. For example, when ventilation-perfusion scanning was replaced by more sensitive CT pulmonary angiography, rates of diagnosis of pulmonary embolism increased; population-level data were required to reveal that this had increased rates of complications of anticoagulation but not reduced mortality rates.29 The diagnostic criteria for mild cognitive impairment and ‘pre-dementia’ are broadening, supported by new cognitive screening tests, cerebrospinal fluid biomarkers and neuroimaging. Population data suggest that such diagnoses often spontaneously resolve, are not consistently associated with progression to dementia and produce a range of harms.30 Changes in testing technology and threshold changes have increased the prevalence of ‘pre-diabetes’ twofold to threefold, with massive prevalence in some populations (eg, 50% in Chinese adults). However, population-level data suggest this is not beneficial and may be producing new harms and costs.31 The counterfactuality problem makes it impossible for an individual diagnosed with pulmonary embolism, pre-dementia or pre-diabetes to know what would have occurred had they not received the diagnosis and intervention. However, their outcomes can be aggregated, and this—at a population level—can allow overdiagnosis to be inferred.
So, although overdiagnosis does occur in individuals, it can rarely be observed in individuals.iii It follows that, to be useful, the definition of overdiagnosis must be expressed at a population level rather than an individual level. Even if we were able to generate a satisfying individual-level definition, it could rarely be used. A useful definition of overdiagnosis will operate at a population level and can be used as a guide to policy and practice. The goal would be to alter diagnostic practices in such a way that cases of overdiagnosis—the (largely unidentifiable) cases that would have aggregated to create the population-level rate of overdiagnosis—do not occur.
Expressing the benefit and/or harm component of overdiagnosis in population terms requires thinking statistically or probabilistically. In addition, because treatment may cause harm in order to benefit, these two must be held in relation to one another in the definition. Cancer treatment, for example, is often harmful (eg, causing nausea or bodily disfigurement) but can prevent early death, providing recipients with the benefit of decades more of life. Because of this, we judge it to be beneficial on balance despite the harms. Following this, the component of overdiagnosis relating to consequences should be expressed in terms of an unfavourable balance between benefits and harms.
The unfavourable balance between benefits and harms relates to the aggregative good or bad of overdiagnoses. However, overdiagnosis also produces corporate harms. Overdiagnosis mostly arises from system-level shifts: changing the definition of conditions, introducing new technologies and aggressively promoting testing. Because the balance between benefits and harms caused by the diagnosis is unfavourable, the economic cost of these activities to the health system is not justified by their outcome. They effectively divert resources from more to less effective care.32 This has an aggregative component (the harms experienced by individuals whose care is compromised). But it is also a corporate harm: it produces a less responsive, less trustworthy, less effective healthcare system.iv Taking the resource allocation implications of overdiagnosis seriously entails identifying services most likely to do aggregative or corporate harm or wrong. This leads to the next question: how to define which benefits, harms or wrongs matter.
Who should judge benefit and harm?
There are two possible answers to the question of who should determine which benefits, harms or wrongs matter, each supported by reasonable arguments. Although these answers may seem incommensurable, they are likely to be combined in practice.
The first answer is: individuals receiving interventions should be free to judge which benefits, harms and costs matter to them. This is a proceduralist view: it suggests that what matters is due process. Individuals, in this view, should not be coerced into interventions; some would suggest they should also be supported to choose in accordance with their values.35 This view loosely reflects classical liberalism, founded in the intrinsic political and moral significance of (1) having one's autonomy respected, and (2) having the liberty or freedom to pursue what one values. Such freedoms are unquestionably important, but this model is not uncomplicated.
Aronowitz has made the important observation that once diagnosed people may act in accordance with the worst-case scenario rather than their own situation. For example, rates of prophylactic mastectomy have been increasing. Women diagnosed as ‘high risk’ for breast cancer (eg, through genetic testing) have been electing to have mastectomies. Women diagnosed with stage I, II and III breast cancer in one breast have been electing to have both breasts removed.11 Other work has also shown an increasing US trend for American women diagnosed with DCIS, a pre-cancer or cancer risk factor, to opt for bilateral mastectomy.36 Importantly, although the likelihood of benefit of prophylactic mastectomy will likely differ between these groups, uptake has been steadily increasing across all groups.11 Women may, of course, have excellent and carefully considered reasons for such choices. However, this analysis suggests it is also possible that risk perception can lead us to accept interventions that are disproportionate to the problem, particularly if healthcare systems actively make them available to us.
Other challenges face the proceduralist view. It may be difficult for clinicians to balance the preferences of individuals against resource implications for the system. Shared decision-making is resource-intense, and dedicated efforts are required to ensure equitable outcomes.37 ,38 There is also a disjunct between this method of judging the balance of benefits to harms and our contention that overdiagnosis can only be defined at population level. While there may be intrinsic moral goods in allowing or supporting each individual to judge what matters to her, this provides little guidance for determining whether or not a pattern of care is causing overdiagnosis in a population.
An alternative could be characterised as a substantive view: that is, a view that experts or authorities should define which benefits, harms and costs are important in each case, and determine how they should be measured. Overdiagnosis cannot be estimated in populations, and medicine cannot function, without some substantive view of which benefits and harms matter. Those who emphasise a substantive view may prioritise minimisation of harm (even at the expense of individual choice) or hold that decision-making should rely on expert, not lay, knowledge. A substantive position also has weaknesses: experts are likely to disagree on which harms or benefits matter, and may seek to coercively impose the interventions they prefer onto individuals. Somehow the significant heterogeneity of risk, disease and illness experience needs to be adequately reflected in the substantive position taken. And even if experts attempt to take ‘the patient perspective’ into account, they can never completely capture and reflect what matters to any given individual. To quote Greenhalgh and colleagues:… [Patients] live in the messy, idiosyncratic, and unpredictable world of a particular person in a particular family context (or, for some, in a context of social isolation and/or abandonment by family) … patients' priorities ‘on average’ … can never fully capture the situated, fluctuating granularity of what matters most to a particular patient and carer at a particular point in the illness journey.39
Greenhalgh and colleagues go on to argue that evidence-based medicine (which is, at its heart, an attempt to integrate best evidence of benefits and harms into clinical practice) is biased in systematic ways that de-privilege human experience and exclude what matters to people.v Thus, while a birds-eye, population-level, average view of benefits and harms is necessary even to determine whether overdiagnosis is occurring, it needs to be nuanced and responsive to heterogeneity in experience and values, and it can never be sufficient, particularly when intervening with individuals.
Although they may seem incommensurable, proceduralist and substantive views are likely to be combined in practice. Substantive assessments of benefit and harm may be strengthened if they are procedurally just (eg, by including citizens and being transparent). Conversely, individuals cannot make good choices about interventions without some substantive content to consider. The balance between substantive and procedural concerns will likely shift depending on the case. If experts agree that a test or procedure is extremely harmful to many people, for example, few would argue that all patients should be offered the test and invited to fully consider its benefits and harms. More frequently, however, the benefits and harms of an intervention will be equivocal. Diagnosis of and intervention for cardiovascular disease risk in most people, for example, is of equivocal benefit.40 In such situations, the determination of the rate of overdiagnosis will need to be contextualised in careful qualification about how benefits and harms were selected and valued, it may be appropriate to run processes such as community juries that seek citizen guidance for policymaking, and shared decision-making may become especially important in the clinic.
Defining overdiagnosis: a summary
Our first guiding question was: How should overdiagnosis be defined? We began with the common meaning-in-use of overdiagnosis—a correct diagnosis that does not benefit—and developed and contextualised it further. Our argument thus has produced the following definition of overdiagnosis.
Consider a condition prevalent in a population, customarily labelled with diagnosis A. We propose that overdiagnosis is occurring in respect of that condition in that population when
the condition is being identified and labelled with diagnosis A in that population (consequent interventions may also be offered);
this identification and labelling would be accepted as correct in a relevant professional community;
the resulting label and/or intervention carries an unfavourable balance between benefits and harms.
As we have shown, benefits and harms occur at the level of individuals and populations; citizens, patients and experts have a role in identifying and weighting relevant benefits and harms.
The normative significance of overdiagnosis
Our second guiding question was: What are the ethical implications of overdiagnosis? We have already noted that overdiagnosis is unavoidably normative: it cannot be defined without considering benefit and harm. However, normative arguments about overdiagnosis tend to be underdeveloped. The moral wrong of overdiagnosis is tacitly assumed to be equivalent to the harm done: the more harm, the more wrong; the less harm, the less wrong. We aim to capture a wider range of relevant moral considerations and sketch a framework for making moral judgements about overdiagnosis. Although this aim suggests a certain degree of generalisability, we note that the foundation for any judgements about overdiagnosis must be in the details of the particular case, including
what relevant professional communities accept as correct judgements and actions;
the process by which these positions were formed;
an account of what benefits and harms are relevant, with a balance between substantive and procedural, population and individual concerns.
It seems reasonable for moral evaluation to be founded in consequences, that is, to assume that more harmful and costly overdiagnosis will undermine utility most strongly, and thus be more ethically problematic. However, we propose adding two further considerations:
The degree to which overdiagnosis is avoidable: the more avoidable, the less morally justifiable.
The goal of the actors involved, especially whether the actor seeks to benefit themselves, or to benefit patients or citizens. This distinguishes overdiagnosing judgements and actions designed primarily to benefit patients or society from those designed primarily to benefit the actor (clinician, corporation or state). This distinction is by no means dichotomous, and one actor may have multiple goals.
Three types of overdiagnosing action with different normative implications
The degree of harm, avoidability of harm and actors' goals interact to produce a typology of overdiagnosing actions. We propose these as ideal types in a sociological sense: they are referents against which messy, real cases can be compared. They do not seem morally equivalent. We have named the three types predatory, tragic and misdirected overdiagnosis. Recall that, in all three types, the balance between benefits and harms must be unfavourable (as specified in the definition of overdiagnosis), and that the greater the harm, the more morally problematic. This is assumed in the following sections.
Predatory overdiagnosing actions
Predatory overdiagnosis occurs in situations where consequent harms are avoidable, and the goal of the actor or actors is self-benefit. Predatory overdiagnosing actions include those that expand a professional standard for personal gain or apply such an expanded standard for personal gain. They tend to be characterised by novelty, adding to the diagnoses considered correct in a professional community, or redefining new practices, or previously ‘incorrect’ practices, as correct. Predatory actions may include coining new conditions, expanding the definition of conditions, increasing testing frequency or introducing new, more sensitive testing technologies. Actors engaged in predatory overdiagnosis use patients primarily as a means to their own ends as their main goal is to benefit themselves.
Take, for example, a pharmaceutical company that owns an approved drug. They create and promote a new, unapproved therapeutic indication for use of that drug. Through academic detailing to promote off-label prescribing to GPs, they achieve a meteoric rise in the diagnosis of this condition, use of the drug, and their own profits. However, the drug has considerable negative effects, leading to widespread harm. Without changing formal clinical guidelines, the company has established a new ‘reasonable practice’ in a relevant professional community. Imagine then a clinician who sets up a specialist clinic providing only this new treatment for profit. In both cases, the harm was entirely avoidable, and the actors (primarily, but not necessarily solely) set out to benefit themselves financially and reputationally. An example: notwithstanding the uncertain evidence and professional disagreement regarding the balance of benefits to harms of testosterone therapy in ageing men,41 the ‘Low T’ (low testosterone) campaign appears to have some predatory overdiagnosing characteristics.42
Predatory overdiagnosis seems the least morally justifiable of the three forms. If proven, penalties and constraints on future liberty of relevant actions may be reasonable (eg, banning a company from academic detailing or contributing directly or indirectly to guideline development). One basis for arguing this would be an objection to individuals being used primarily as means to others' ends. This conduct also seems blameworthy because it undermines the very basis of medicine: it is a knowing attempt to undermine professional standards that are hard-won, necessary for clinical care, and the grounds for a relationship of trust between the profession and the community.
Tragic overdiagnosis
Tragic overdiagnosis, in contrast, seems the least blameworthy and may be morally justifiable. In this case, harms are unavoidable and the goal of the actor or actors is mainly to benefit others (eg, people with the condition). Tragic overdiagnosis may occur when relevant professional communities do not yet recognise that a test or treatment may cause harm, or when there is great disagreement in relevant professional communities or when guidance to clinicians is unclear. It is likely that tragic overdiagnosis can be seen only in retrospect, when it becomes apparent that the balance of benefits to harms of a diagnosis is substantially worse than was originally thought.
One example of tragic overdiagnosis may be the Japanese programme to screen infants for neuroblastoma.2 This cancer occurs almost exclusively in small children, is (now known to be) highly heterogeneous, is usually detected after metastasis and can regress.43 Japan started screening infants for neuroblastoma in 1984, when awareness of overdiagnosis in cancer screening was low; it seems plausible that relevant professional communities expected screening to help patients. In 2002, Canadian and German studies of neuroblastoma screening showed no mortality benefit; the Japanese government consequently organised a review of the programme; it was disbanded in March 2004.44 The fact that the programme ended (rather than continuing in the face of contradictory evidence) suggests a goal of benefiting children outweighed any goal of benefiting clinicians or the health service. Taken together, this suggests that, especially in its earliest incarnation, the overdiagnosis in the Japanese neuroblastoma screening programme was largely tragic.
As we previously noted, tragic and predatory overdiagnosis are not strongly dichotomous categories: rather, they are opposite ends of a continuum. Between them, and even more complex, is misdirected overdiagnosis.
Misdirected overdiagnosis
Misdirected overdiagnosis sits between tragic and predatory overdiagnosis: it occurs when harm is avoidable, but the goal of the actor or actors is primarily to benefit others (patients or citizens). Take, for example, a group of specialists committed to a new imaging technology: they believe it will revolutionise early detection of a disease. They work with their college to introduce the technology to standard practice. There is a resulting rapid increase in the incidence of the disease but outcomes do not improve. Some people are actively harmed by further unnecessary tests and treatments. Misdirected overdiagnosis has occurred. This may not become apparent immediately, depending on how attentive researchers or evaluators are to the outcomes being generated by the interventions at a population level. Eventually, however, there will be at least one professional group who make an evidence-based case that the balance of benefits to harms of the intervention is not as favourable as was suggested by its proponents.
It will often be a matter for argument whether a particular instance of overdiagnosis is predatory, misdirected or tragic. Take CT screening for early detection of lung cancer.45 Assuming that screening was considered correct in some relevant community, the resulting overdiagnosis could be predatory, misdirected or tragic. The more those promoting screening set out to make money or enhance their own reputations, and the more likely harms were known, then the more predatory the overdiagnosis becomes. If the advocates of screening were primarily motivated by helping patients, but they should have predicted non-benefit, they produced misdirected overdiagnosis. Now imagine a CT technician advised that the new standard practice in her profession is to screen people for lung cancer. She believes this will save people's lives. If she could not be reasonably expected to know that screening would do more harm than benefit, the overdiagnosis is tragic. If—and this is more likely—the technician was not self-interested but should have predicted that screening could harm rather than benefit because this is a common feature of new tests, the overdiagnosis is misdirected.
Consider one more example: bladder cancer. Urologists decided some time ago that being diagnosed with the lowest grade of bladder cancer caused harm and did not cause enough benefit to outweigh the harm. Pathological changes were observable, but calling them ‘cancer’ led to unnecessary, harmful investigations and treatments.46 By recognising this problem and changing the diagnostic label, urologists changed the official professional understanding of ‘correct’ clinical practice for this condition. However, imagine that some urologists disagree and continue to argue that that these patients should be diagnosed with cancer. Before the reclassification, a urologist whose goal was to help her patients, but harmed them by diagnosing them with the lowest grade of bladder cancer, would have produced tragic overdiagnosis. After the change, a urologist who persisted in applying the old standard with the goal of helping patients, and in so doing perpetuates the unfavourable balance between benefits and harms, would produce misdirected overdiagnosis. If a group of urologists formed a new society to promulgate continued diagnosis of low-grade bladder cancer to protect their own incomes, despite understanding the likelihood of non-benefit or harm, they would be engaging in predatory overdiagnosis. If, eventually, the consensus became overwhelming, such that clinicians applying the old standard were individual outliers, their diagnoses would simply be incorrect rather than overdiagnosis.
Misdirected overdiagnosis is the most difficult to evaluate normatively: it seems likely to be unjustifiable but not unconscionable. It seems reasonable to recognise the moral worth of seeking to benefit others, and to focus remedies on improving and enforcing professional standards for reasonable practice, rather than condemning or sanctioning individual actors.
How clear are these distinctions?
In general, we believe these distinctions are useful for normative reasoning about overdiagnosis. Occasionally, the types will exist in a pure form. For example, predatory overdiagnosis might be proven if the internal documents of a drug manufacturer are discovered, and these spell out a plan to invent a new condition, for a profit motive, in spite of known harms. But this will be rare: it is more useful to consider predatory, misdirected and tragic overdiagnosis to be ideal types. Determining the goals of an actor can be difficult, and actors frequently have multiple goals. Judgements of avoidability are also complex and depend on the relevant professional standard. Thus, professionals in different disciplines or subdisciplines may allocate a well-intentioned action differently to misdirected (avoidable) or tragic (unavoidable) overdiagnosis. And the standard will not always be clear, especially for diagnosis, which tends to be less well understood, researched and regulated than treatment. This complexity and opacity suggests that overdiagnosing actions may often be predatory, misdirected or tragic by degree, rather than absolutely.
If predatory, misdirected and tragic overdiagnosis produce the same consequences, aren't they morally equivalent?
A possible objection to our argument may come from an act utilitarian position. As noted, implicitly utilitarian reasoning is common in the overdiagnosis literature (the more harm done, the more morally unjustified the overdiagnosis). If this was correct, then tragic, misdirected and predatory overdiagnosis would all be equally bad, providing they produced the same quantity of harm.
However, most approaches to public health ethics are more layered. Like us, they begin from consequences and augment with other moral concerns, such as respect for liberty or autonomy, procedural and distributive justice, proportionality, necessity and reciprocity.47 Our overall approach—adding moral considerations to a consequentialist foundation—thus has considerable precedent in the literature. We have added those features that appear most morally relevant to us; the resulting approach is sensitive to degrees of moral culpability and thus appropriateness of sanctions. However, we expect that there will be other frameworks developed and some contest of ideas before any consensus can be reached on which moral concerns are most relevant.
Fundamental problems facing the normative evaluation of overdiagnosis
We conclude with four unresolved ethical questions arising from the current landscape of overdiagnosis and the need to address it.
Procedural justice in identifying benefits, harms and professional standards
Throughout, we have emphasised the potential conflicts in determining reasonable actions, and relevant benefits or harms. Many epidemiologists and economists are currently working to quantify the benefits, harms and costs of potentially overdiagnosing interventions. To do this, they need to make assumptions about the standard for reasonable actions as these separate ‘correct’ from ‘incorrect’ care, and so separate overdiagnosis from error. They also need to define the benefits, harms and costs that they will measure and model. But these assumptions are often implicit. The overdiagnosis movement may benefit from a more procedurally just approach to addressing these fundamental problems. For example, community juries or the principles of accountability for reasonableness could be used to determine what benefits, harms and costs should matter and why.48 ,49 In addition to being goods in themselves, such processes would provide fairer means for negotiating differences between professional standards and communities.
Who is morally responsible for overdiagnosis, including the opportunity costs?
The literature is not clear on who should reasonably be held responsible for fixing the problem of overdiagnosis. It is variously implied that policymakers, clinicians, lawmakers, manufacturers and/or citizens should act. There are many open questions in this area. Is it reasonable, for example, to expect citizens to engage with detailed information and make their own decisions if experts cannot reach agreement on what is reasonable? Or if predatory overdiagnosis is identified, who should respond to contain it? We have shown that overdiagnosis is multifactorial, and it seems likely that different actors may be responsible for different components. For example, regulators or the courts may be responsible for sanctioning the worst cases of predatory overdiagnosis, while individual clinicians may only be responsible for avoiding misdirected overdiagnosis by examining their clinical goals and adhering to a justifiable professional standard. Our analysis emphasises that overdiagnosis is an artefact of systems of healthcare. This suggests we should be wary of overindividualising moral responsibility for the problem. In fact, some of the core elements of our system—such as defining and maintaining the integrity of professional standards—require collective effort for their achievement and are corporate goods in themselves.
Individuals will carry some moral responsibility for some forms of overdiagnosis, perhaps most strongly predatory overdiagnosis. However, collective actors such as states or professional bodies may reasonably be held responsible for providing the structures needed to minimise the chance of future overdiagnosis. So, for example, if professional standards are in conflict, and some suggest harms are large and avoidable, there may be a shared obligation to reach fair agreement on which standard is correct. If the conclusion is that large avoidable harms are occurring, there may be a collective obligation to strongly guide individual clinicians (who rely on the standard) away from testing, rather than maintaining a laissez-faire practice environment with substantial potential for individual clinical discretion. If predatory actors continue to promote alternative pro-testing standards, and funding arrangements make testing easy, collective actors such as colleges, expert bodies and the research community may be obliged to actively promulgate their agreed standard, criticise problematic standards, remove funding for testing and/or sanction predatory actors.
Recognising overdiagnosis as a matter for distributive justice
Overdiagnosis is a matter for distributive justice in two competing ways. First, a pressing moral problem with overdiagnosing interventions is their structural effects on the healthcare system. Overdiagnosis often arises from the application of expensive new testing or treatment technologies. This diverts resources away from basic health services and public health interventions, and may threaten the sustainability of universal healthcare where it exists.32 This is likely to effect the least-well-off, who are least able to pay for services, most strongly. This is a matter for justice and a loss of a corporate good, and can only be addressed at a systems level.
Conversely—and paradoxically—limiting diagnostic categories may redefine individuals as non-diseased, or even malingering, which may remove the health and social care that follows official medical labels. A diagnosis can provide access not just to medical care but also to social, welfare and other services. For example, being diagnosed with a mental illness may be a pathway not only to drug treatment, but also to psychological treatment, social supports or a disability pension. A diagnosis of attention-deficit hyperactivity disorder may facilitate not only drug treatment, but also extra help in the classroom, or parenting support. While medicalising ‘normal’ life experiences can be very reasonably critiqued and may do harm in itself,5 ,26 there can also be beneficial social effects of receiving a medical label.
Thus, efforts to reduce overdiagnosis may have negative social consequences for the people who rely on the social power of that diagnosis. This is not morally neutral, particularly when public services are under threat. It may also especially disadvantage the least-well-off who may lose access to services without the power of a diagnostic label. This is the paradox: overdiagnosis may misallocate needed funds away from universal healthcare, which will disadvantage the least-well-off; but curbing overdiagnosis may also remove services from the least-well-off.
There is no easy answer, and as previously noted, different groups may be differently responsible for this problem. Researchers, for example, should take care to include all potential benefits and harms, and their distribution, in estimating the effects of interventions to limit overdiagnosis. Policymakers, colleges and other groups with responsibility for practice change should be especially attentive to effects in already-disadvantaged communities. This includes not just the effects of change (eg, the possibility that social services may be lost if a medical diagnosis is removed) but also the effects of remaining with the status quo (eg, the harm that may be done if people continue to be overdiagnosed). It should be noted that the possibility of unintended harms should not prevent action: rather, action should be taken in such a way as to monitor and minimise new harms. Returning to our earlier discussion of identifying benefits and harms, it is likely that potential harms or loss of benefits will only be fully understood if affected communities are included in decision-making.
Responding to the experience of those who may have been overdiagnosed
The final unresolved moral challenge of overdiagnosis is in relation to the harms that may be done by the way overdiagnosis is communicated. Intervention to limit overdiagnosis is generally motivated by a desire to limit harms done to populations by overdiagnosing interventions. However, this has implications with regard to the counterfactual problem. Recall the two women, both diagnosed and treated with breast cancer, one of whom has been overdiagnosed. With low awareness of overdiagnosis, both women are likely to think themselves saved by screening and the onerous treatment they subsequently undertook. As awareness of overdiagnosis is raised, both women are likely to question whether or not they have been overdiagnosed. They may, as a result, experience distress or existential doubts and lose trust in the institution of medicine. This is not a reason to avoid communicating about overdiagnosis, but it does suggest a need for care and the provision of appropriate supports to those affected.
Conclusion
The questions we have addressed (How should overdiagnosis be defined? What are the ethical implications of overdiagnosis?) need to be resolved to provide direction and clarity in this relatively new field. Our analysis on these two questions is summarised in figure 1 (definition) and table 2 (ethical evaluation).
An ethical evaluation of overdiagnosis
{kind=link}
Defining overdiagnosis.
Our most important conclusion is that overdiagnosis is a shared problem. Informing individual citizens and patients, and supporting them to make decisions about their healthcare in accordance with their own values, is morally important. But, as we have argued, overdiagnosis can only be observed at a population level, it arises from changes in the routine operation of health systems, it is judged in relation to standards set within professions, its recognition depends on agreement regarding which benefits and harms matter and how they should be measured, and most of the solutions to it require the cooperation or action of collective agents such as professional colleges, regulators or even courts. Individuals, whether clinicians, patients or citizens, cannot be expected to prevent overdiagnosis alone: this will only occur when health systems attend to both benefits and harms, and regularly reorient to prioritise beneficial over harmful healthcare. Other authors are working on definitions and frameworks, and there is likely to be some contest over these in coming years. We believe that our approach draws out important features of overdiagnosis as a definitional and moral problem, and provides useful groundwork. We look forward to participating in the ongoing conversation as it progresses.
References
Footnotes
↵i Overdiagnosis is distinct from the other ‘over’ concepts in several ways. This includes that overdiagnosis can only occur when a diagnosis is made, in contrast to the broader concepts such as medicalisation and overuse. We have suggested elsewhere that a term like ‘too much medicine’ should be used as a broad umbrella term instead of overdiagnosis to prevent confusion.8
↵ii Personalised and precision medicine aim to achieve something close to the correspondence standard. If genomic tests were ever perfectly predictive of phenotypic disease expression in individuals, it is possible that they could become a means for avoiding overdiagnosis and overtreatment. However, so far this seems rarely to be the case. This may lead either to overconfidence in the new technologies (which could drive overdiagnosis because genetic markers of uncertain significance become grounds for overzealous interventions) or underconfidence in the new technologies (which could nonetheless drive ‘just in case’ overtreatment, but in the context of considerable uncertainty and anxiety). For a more detailed discussion, see ref. 18.
↵iii One unusual exception is when a person is diagnosed with early-stage cancer due to screening, refuses treatment, and does not advance to late-stage disease. Note, though, that there is no way of knowing at the time of diagnosis that the person is overdiagnosed: this can be known only retrospectively, after the passage of time and the non-emergence of symptoms.
↵iv Such distortions of health systems have been recognised by others under different guises: examples include Julian Tudor Hart's inverse care law33 and Brody and Light's inverse benefit law.34
↵v This is so even in the generation of the evidence on which researchers draw to calculate the balance of benefits to harms. Greenhalgh and colleagues describe the Diabetes Control and Complications Trial, in which investigators concluded that ‘intensive’ diabetes control was justified because it led to a reduction in microvascular complications. This was despite them cataloguing the ‘comas, seizures, and fatal motor accidents’ due to severe hypoglycaemia that resulted from intensive control. The people with type I diabetes experiencing these hypoglycaemic episodes may have taken a different view, as discussed in ref. 39.
Twitter Follow Stacy Carter at @stacymcarter
Contributors SMC led the analysis and writing. All four authors contributed to the development of the argument, through a collaborative, iterative process.
Funding National Health and Medical Research Council (1023197) and (1032963).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Commentary
- Commentary
- Commentary
- Response
Other content recommended for you
- Casting the net too wide on overdiagnosis: benefits, burdens and non-harmful disease
- Defining and evaluating overdiagnosis
- A definition and ethical evaluation of overdiagnosis: response to commentaries
- Overdiagnosis across medical disciplines: a scoping review
- Overdiagnosis in primary care: framing the problem and finding solutions
- The challenge of overdiagnosis begins with its definition
- Survey of public definitions of the term ‘overdiagnosis’ in the UK
- Effects of awareness of breast cancer overdiagnosis among women with screen-detected or incidentally found breast cancer: a qualitative interview study
- Benefits and harms of breast cancer screening revisited: a large, retrospective cross-sectional study quantifying treatment intensity in women with screen-detected versus non-screen-detected cancer in Australia and New Zealand
- Quantifying and monitoring overdiagnosis in cancer screening: a systematic review of methods