Learning and teaching in the clinical environment
BMJ 2003; 326 doi: https://doi.org/10.1136/bmj.326.7389.591 (Published 15 March 2003) Cite this as: BMJ 2003;326:591
- John Spencer
Clinical teaching—that is, teaching and learning focused on, and usually directly involving, patients and their problems—lies at the heart of medical education. At undergraduate level, medical schools strive to give students as much clinical exposure as possible; they are also increasingly giving students contact with patients earlier in the course. For postgraduates, “on the job” clinical teaching is the core of their professional development. How can a clinical teacher optimise the teaching and learning opportunities that arise in daily practice?

Clinical teaching in general practice
Strengths, problems, and challenges
Learning in the clinical environment has many strengths. It is focused on real problems in the context of professional practice. Learners are motivated by its relevance and through active participation. Professional thinking, behaviour, and attitudes are “modelled” by teachers. It is the only setting in which the skills of history taking, physical examination, clinical reasoning, decision making, empathy, and professionalism can be taught and learnt as an integrated whole. Despite these potential strengths, clinical teaching has been much criticised for its variability, lack of intellectual challenge, and haphazard nature. In other words, clinical teaching is an educationally sound approach, all too frequently undermined by problems of implementation.
Common problems with clinical teaching
Lack of clear objectives and expectations
Focus on factual recall rather than on development of problem solving skills and attitudes
Teaching pitched at the wrong level (usually too high)
Passive observation rather than active participation of learners
Inadequate supervision and provision of feedback
Little opportunity for reflection and discussion
“Teaching by humiliation”
Informed consent not sought from patients
Lack of respect for privacy and dignity of patients
Lack of congruence or continuity with the rest of the curriculum
Challenges of clinical teaching
Time pressures
Competing demands—clinical (especially when needs of patients and students conflict); administrative; research
Often opportunistic—makes planning more difficult
Increasing numbers of students
Fewer patients (shorter hospital stays; patients too ill or frail; more patients refusing consent)
Often under-resourced
Clinical environment not “teaching friendly” (for example, hospital ward)
Rewards and recognition for teachers poor
The importance of planning
Many principles of good teaching, however, can (and should) be incorporated into clinical teaching. One of the most important is the need for planning. Far from compromising spontaneity, planning provides structure and context for both teacher and students, as well as a framework for reflection and evaluation. Preparation is recognised by students as evidence of a good clinical teacher.

Questions to ask yourself when planning a clinical teaching session
How doctors teach
Almost all doctors are involved in clinical teaching at some point in their careers, and most undertake the job conscientiously and enthusiastically.
However, few receive any formal training in teaching skills, and in the past there has been an assumption that if a person simply knows a lot about their subject, they will be able to teach it. In reality, of course, although subject expertise is important, it is not sufficient. Effective clinical teachers use several distinct, if overlapping, forms of knowledge.

Various domains of knowledge contribute to the idiosyncratic teaching strategies (“teaching scripts”) that tutors use in clinical settings
How students learn
Understanding the learning process will help clinical teachers to be more effective. Several theories are relevant (see first article in the series, 25 January). All start with the premise that learning is an active process (and, by inference, that the teacher's role is to act as facilitator). Cognitive theories argue that learning involves processing information through interplay between existing knowledge and new knowledge. An important influencing factor is what the learner knows already. The quality of the resulting new knowledge depends not only on “activating” this prior knowledge but also on the degree of elaboration that takes place. The more elaborate the resulting knowledge, the more easily it will be retrieved, particularly when learning takes place in the context in which the knowledge will be used.
How to use cognitive learning theory in clinical teaching
Help students to identify what they already know
“Activate” prior knowledge through brainstorming and briefing
Help students elaborate their knowledge
Provide a bridge between existing and new information—for example, use of clinical examples, comparisons, analogies
Debrief the students afterwards
Promote discussion and reflection
Provide relevant but variable contexts for the learning
Experiential learning
Experiential learning theory holds that learning is often most effective when based on experience. Several models have been described, the common feature being a cyclical process linking concrete experience with abstract conceptualisation through reflection and planning. Reflection is standing back and thinking about experience (What did it mean? How does it relate to previous experience? How did I feel?). Planning involves anticipating the application of new theories and skills (What will I do next time?). The experiential learning cycle, which can be entered at any stage, provides a useful framework for planning teaching sessions.
Example of clinical teaching session based on experiential learning cycle
Setting—Six third year medical students doing introductory clinical skills course based in general practice
Topic—History taking and physical examination of patients with musculoskeletal problems (with specific focus on rheumatoid arthritis); three patients with good stories and signs recruited from the community
The session
Planning—Brainstorm for relevant symptoms and signs: this activates prior knowledge and orientates and provides framework and structure for the task
Experience—Students interview patients in pairs and do focused physical examination under supervision: this provides opportunities to implement and practise skills
Reflection—Case presentations and discussion: feedback and discussion provides opportunities for elaboration of knowledge
Theory—Didactic input from teacher (basic clinical information about rheumatoid arthritis): this links practice with theory
Planning— “What have I learned?” and “How will I approach such a patient next time?” Such questions prepare students for the next encounter and enable evaluation of the session

Experiential learning cycle: the role of the teacher is to help students to move round, and complete, the cycle
Questions
Questions may fulfil many purposes, such as to clarify understanding, to promote curiosity, and to emphasise key points. They can be classified as “closed,” “open,” and “clarifying” (or “probing”) questions.
Effective teaching depends crucially on the teacher's communication skills. Two important areas of communication for effective teaching are questioning and giving explanations. Both are underpinned by attentive listening (including sensitivity to learners' verbal and non-verbal cues). It is important to allow learners to articulate areas in which they are having difficulties or which they wish to know more about
Closed questions invoke relatively low order thinking, often simple recall. Indeed, a closed question may elicit no response at all (for example, because the learner is worried about being wrong), and the teacher may end up answering their own question.
In theory, open questions are more likely to promote deeper thinking, but if they are too broad they may be equally ineffective. The purpose of clarifying and probing questions is self evident.
How to use questions
Restrict use of closed questions to establishing facts or baseline knowledge (What? When? How many?)
Use open or clarifying/probing questions in all other circumstances (What are the options? What if?)
Allow adequate time for students to give a response—don't speak too soon
Follow a poor answer with another question
Resist the temptation to answer learners' questions—use counter questions instead
Statements make good questions—for example, “students sometimes find this difficult to understand” instead of “Do you understand?” (which may be intimidating)
Be non-confrontational—you don't need to be threatening to be challenging
Explanation
Teaching usually involves a lot of explanation, ranging from the (all too common) short lecture to “thinking aloud.” The latter is a powerful way of “modelling” professional thinking, giving the novice insight into experts' clinical reasoning and decision making (not easily articulated in a didactic way). There are close analogies between teacher-student and doctor-patient communication, and the principles for giving clear explanations apply. If in doubt, pitch things at a low level and work upwards. As the late Sydney Jacobson, a journalist, said, “Never underestimate the person's intelligence, but don't overestimate their knowledge.” Not only does a good teacher avoid answering questions, but he or she also questions answers.
Questions can be sequenced to draw out contributions or be built on to promote thinking at higher cognitive levels and to develop new understanding
How to give effective explanations
Check understanding before you start, as you proceed, and at the end—non-verbal cues may tell you all you need to know about someone's grasp of the topic
Give information in “bite size” chunks
Put things in a broader context when appropriate
Summarise periodically (“so far, we've covered …”) and at the end; asking learners to summarise is a powerful way of checking their understanding
Reiterate the take home messages; again, asking students will give you feedback on what has been learnt (but be prepared for some surprises)
Exploiting teaching opportunities
Most clinical teaching takes place in the context of busy practice, with time at a premium. Many studies have shown that a disproportionate amount of time in teaching sessions may be spent on regurgitation of facts, with relatively little on checking, probing, and developing understanding. Models for using time more effectively and efficiently and integrating teaching into day to day routines have been described. One such, the “one-minute preceptor,” comprises a series of steps, each of which involves an easily performed task, which when combined form an integrated teaching strategy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Teaching on the wards
Despite a long and worthy tradition, the hospital ward is not an ideal teaching venue. None the less, with preparation and forethought, learning opportunities can be maximised with minimal disruption to staff, patients, and their relatives.
Approaches include teaching on ward rounds (either dedicated teaching rounds or during “business” rounds); students seeing patients on their own (or in pairs—students can learn a lot from each other) then reporting back, with or without a follow up visit to the bedside for further discussion; and shadowing, when learning will inevitably be more opportunistic.
Key issues are careful selection of patients; ensuring ward staff know what's happening; briefing patients as well as students; using a side room (rather than the bedside) for discussions about patients; and ensuring that all relevant information (such as records and x ray films) is available.
Teaching in the clinic
Although teaching during consultations is organisationally appealing and minimally disruptive, it is limited in what it can achieve if students remain passive observers.
Teaching during consultations has been much criticised for not actively involving learners
With relatively little impact on the running of a clinic, students can participate more actively. For example, they can beasked to make specific observations, write down thoughts about differential diagnosis or further tests, or note any questions—for discussion between patients. A more active approach is “hot seating.” Here, the student leads the consultation, or part of it. His or her findings can be checked with the patient, and discussion and feedback can take place during or after the encounter. Students, although daunted, find this rewarding. A third model is when a student sees a patient alone in a separate room, and is then joined by the tutor. The student then presents their findings, and discussion follows. A limitation is that the teacher does not see the student in action. It also inevitably slows the clinic down, although not as much as might be expected. In an ideal world it would always be sensible to block out time in a clinic to accommodate teaching.
The patient's role
Sir William Osler's dictum that “it is a safe rule to have no teaching without a patient for a text, and the best teaching is that taught by the patient himself” is well known. The importance of learning from the patient has been repeatedly emphasised. For example, generations of students have been exhorted to “listen to the patient—he is telling you the diagnosis.” Traditionally, however, a patient's role has been essentially passive, the patient acting as interesting teaching material, often no more than a medium through which the teacher teaches. As well as being potentially disrespectful, this is a wasted opportunity. Not only can patients tell their stories and show physical signs, but they can also give deeper and broader insights into their problems. Finally, they can give feedback to both learners and teacher. Through their interactions with patients, clinical teachers—knowingly or unknowingly—have a powerful influence on learners as role models.
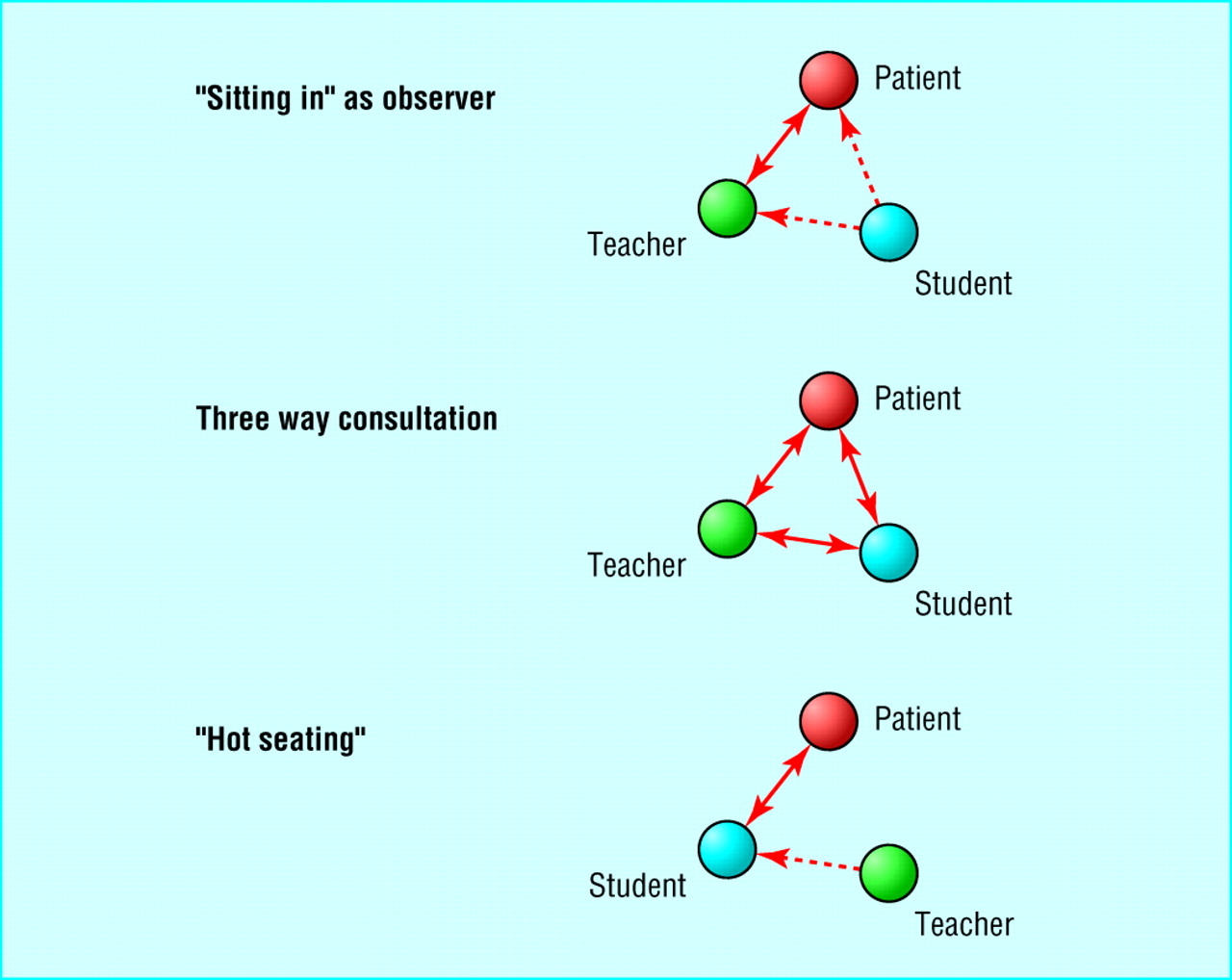
Seating arrangements for teaching in clinic or surgery
{kind=link}
Working effectively and ethically with patients
Think carefully about which parts of the teaching session require direct patient contact—is it necessary to have a discussion at the bedside?
Always obtain consent from patients before the students arrive
Ensure that students respect the confidentiality of all information relating to the patient, verbal or written
Brief the patient before the session—purpose of the teaching session, level of students' experience, how the patient is expected to participate
If appropriate, involve the patient in the teaching as much as possible
Ask the patient for feedback—about communication and clinical skills, attitudes, and bedside manner
Debrief the patient after the session—they may have questions, or sensitive issues may have been raised
Suggested reading
Acknowledgments
Drs Gabrielle Greveson and Gail Young gave helpful feedback on early drafts.
Footnotes
-
John Spencer is a general practitioner and professor of medical education in primary health care at the University of Newcastle upon Tyne.
The ABC of learning and teaching in medicine is edited by Peter Cantillon, senior lecturer in medical informatics and medical education, National University of Ireland, Galway, Republic of Ireland; Linda Hutchinson, director of education and workforce development and consultant paediatrician, University Hospital Lewisham; and Diana F Wood, deputy dean for education and consultant endocrinologist, Barts and the London, Queen Mary's School of Medicine and Dentistry, Queen Mary, University of London. The series will be published as a book in late spring.