Trends in doctor-manager relationships
BMJ 2003; 326 doi: https://doi.org/10.1136/bmj.326.7390.646 (Published 22 March 2003) Cite this as: BMJ 2003;326:646
- Huw T O Davies, professor of health care policy and management (hd{at}st-and.ac.uk)a,
- Stephen Harrison, professor of social policyb
- a Centre for Public Policy and Management, University of St Andrews, Fife KY16 9AL
- b Department of Applied Social Science, University of Manchester, Manchester M13 9PL
- Correspondence to: H T O Davies
Doctors are increasingly unhappy in a changing world.1 Although the reasons for this are broad and far reaching,2 some of this discontent results from the doctor-management interface.3 The rejection of the new NHS consultant contract in England and Wales seemed to crystallise this discontent, hinging as it did on issues of professional autonomy and a lack of trust.4 But such a crisis should not be seen in isolation. We can better understand the current predicament by, firstly, reviewing the history of the doctor-manager relationship in the United Kingdom over recent decades, and in particular seeing this relationship as shaped by the changing structural arrangements from within which health care is delivered. Secondly, such changes are in turn part of an international phenomenon, related in particular to perceived crises of healthcare funding and consequent attempts to improve efficiency.
This overview aims to summarise each of these elements. We draw on a recent review of international developments,5 pre-existing reviews charting changes in the doctor-manager relationship in the NHS 6–8, and a range of more recent empirical studies.9–14
Summary points
One reason for the high level of doctors' discontent lies in the doctor-manager relationship
Such discontent reflects international trends that have led to diminished autonomy and a reduced dominance of doctors in health care
In recent years the “scientific-bureaucratic” model of healthcare delivery has risen to prominence
This model emphasises external robust evidence over personal professional expertise, with patterns of care driven more by managerial processes than through professional motivation
Understanding these dynamics may enable a rethinking of the psychological contract between doctors and the organisations in which they provide services
Management and structural change in the NHS
For a quarter of a century after the foundation of the NHS, its main structures stayed largely intact. After 1974, however, reforms occurred increasingly often, culminating in almost perpetual upheaval in the past five years. Three key reorganisations were the introduction of general management in 1984, the opening up from 1991 of an internal market, and the repeated rounds of performance and accountability initiatives after the election of a “new Labour” government in 1997. The shifting patterns of doctor-manager relationships over these periods can then be examined in terms of two key issues—how the relative influence of doctors and managers has changed and what were and are the main determinants and focuses of managerial agendas.
Relative influence of doctors and managers
From the early days of the NHS, doctors rather than managers (then, tellingly, officially called administrators) had dominant and pervasive influence. The shape and distribution of services arose from an accumulation of individual clinical decisions, with managers supporting and administering these arrangements rather than seeking to challenge them.15 The introduction of general management in 1984 provided a focus for financial administration but left patterns of clinical care—and hence influence from doctors—largely untouched.6 However, the development of the internal market in the early 1990s, the subsequent increasingly strident set of demands about service delivery and accountability, and most recently the introduction of clinical governance have all enabled managers to drive through substantial restructuring of clinical services, sometimes in the face of outright physician dissent.16
Throughout this period there were many attempts to involve doctors more fully in management activities,9 including the statutory role of the medical director and the development of clinical directorates. Such participation by doctors in management has not been easily accomplished, with medical directors experiencing considerable workload challenges and stress17 and clinical directors displaying high levels of disenchantment.11 Thus, despite this rebalancing of power between doctors and managers, a sense often remains among both groups that the important power lies elsewhere, so that a degree of disempowerment is frequently felt on both sides.
Aspects of clinical autonomy7
Control over diagnosis and treatment—Decisions about which tests and examinations are appropriate; the drugs and procedures to be used; who to refer and where; and the nature of follow up care
Control over evaluations of care—Judgments about the appropriateness of either the care of individual patients or the overall patterns of care provided
Control over nature and volume of medical tasks—The extent to which doctors are left to determine their own priorities, workloads, and supporting activities, including the location and timing of these activities
Contractual independence—The extent to which doctors have unilateral rights to engage in extracurricular activities such as teaching, research, royal college or BMA business, commercial consultancy, or private practice

(Credit: SIMON FRASER/SPL)
Determinants and focus of managerial agendas
Administrators in the 1970s and early ‘80s tended to be reactive to emergent problems rather than proactive in developing corporate objectives. The key clients in terms of determining managerial activity were senior clinicians rather than service users.18 At the same time, political control was relatively loose, although this tightened in the 1980s as general management provided a focal point for political leverage. The emergence of (even relatively attenuated) competitive forces in the 1990s drove managers to be more proactive in developing strategic objectives and plans to meet these. 19 Thus managers increasingly had a corporate outlook, seeking to maintain and develop their own institutions' facilities. As the market was replaced by supposedly more cooperative forms of working—supplemented by central diktat, the national performance framework, star ratings, and a plethora of regulatory and inspection mechanisms—the focus of senior management changed such that they are now seen more as agents of government than as facilitators of professionally driven agendas.
Although these changes are hugely important, they should be seen as gradual shifts and accumulations over time rather than as stark discontinuities resulting from specific policy initiatives. Furthermore, although doctors resisted (sometimes vociferously) many of the underlying changes, they quickly assimilated the changes and their corollaries12 and seemed to have little desire to revert to prior arrangements.8 In this there may well be substantial age related effects—for example, junior doctors are keen to be more involved in management roles.20 Specialties may also differ, with some—such as radiology, pathology, and psychiatry—being more sympathetic to a managerial culture.13 The changes, however, have not been without consequence for professional practice.
International trends
Trends in developed, liberal democracies may be summarised in the following broad terms, though this conceals some important differences of detail.5 Firstly, there has been an increasing “systematisation” of medical knowledge. This has occurred partly through methods that allow the measurement of medical work for managerial purposes—for example, case-mix measures such as diagnosis related groups and similar. Such measures have been used in many countries, including the United States, the United Kingdom, Germany, Australia, and the Netherlands, as a possible basis for prospective remuneration for healthcare institutions. Systematisation of medical knowledge has also occurred worldwide through strategies that determine how doctors should deliver care, both at the level of the individual patient encounter (for example, clinical protocols and guidelines) and in terms of the processing of patients through the system (for example, prescribed “patient pathways”).
Secondly, increasing attention has been paid to the financial and other incentives offered to doctors. Incentives may be aimed directly at individual doctors—such as capitation payments, caps on fee-for-service income, and target payments for screening set proportions of a population. Incentives may also be aimed indirectly—related to workload for the hospitals and clinics in which doctors are increasingly located. Incentivising organisations in this way increases the need for medical work to be managed. Most countries are now paying greater attention to the incentives context for medical work, particularly through the arrangements of managed care.21
Thirdly, state regulation of medicine as a profession has been modified and supplemented in various ways. Some such modifications aim to reduce the supply of doctors—as in Germany, France, and Italy—whereas other reforms aim to reduce the medical near-monopoly of the institutions of state registration, as in the United Kingdom, Belgium, and Spain. Much regulatory activity is aimed more directly at modifying clinical practice22 and includes the creation of new inspectorates, the introduction of compulsory clinical audit, publication of league tables of hospital and clinic performance indicators, and tightened gate keeping arrangements between primary and secondary care or between ambulatory and hospital care. A wide range of countries have adopted such approaches, including the United Kingdom, the United States, Germany, and Belgium.
An overriding theme of the diverse changes over 30 years has been a substantial erosion of the professional medical dominance and autonomy.7 Although different aspects of medical autonomy at the micro level can be identified (box), all of these have to some extent been undermined, constrained, or curtailed as a consequence of the trends outlined above.
Changing modes of medical practice
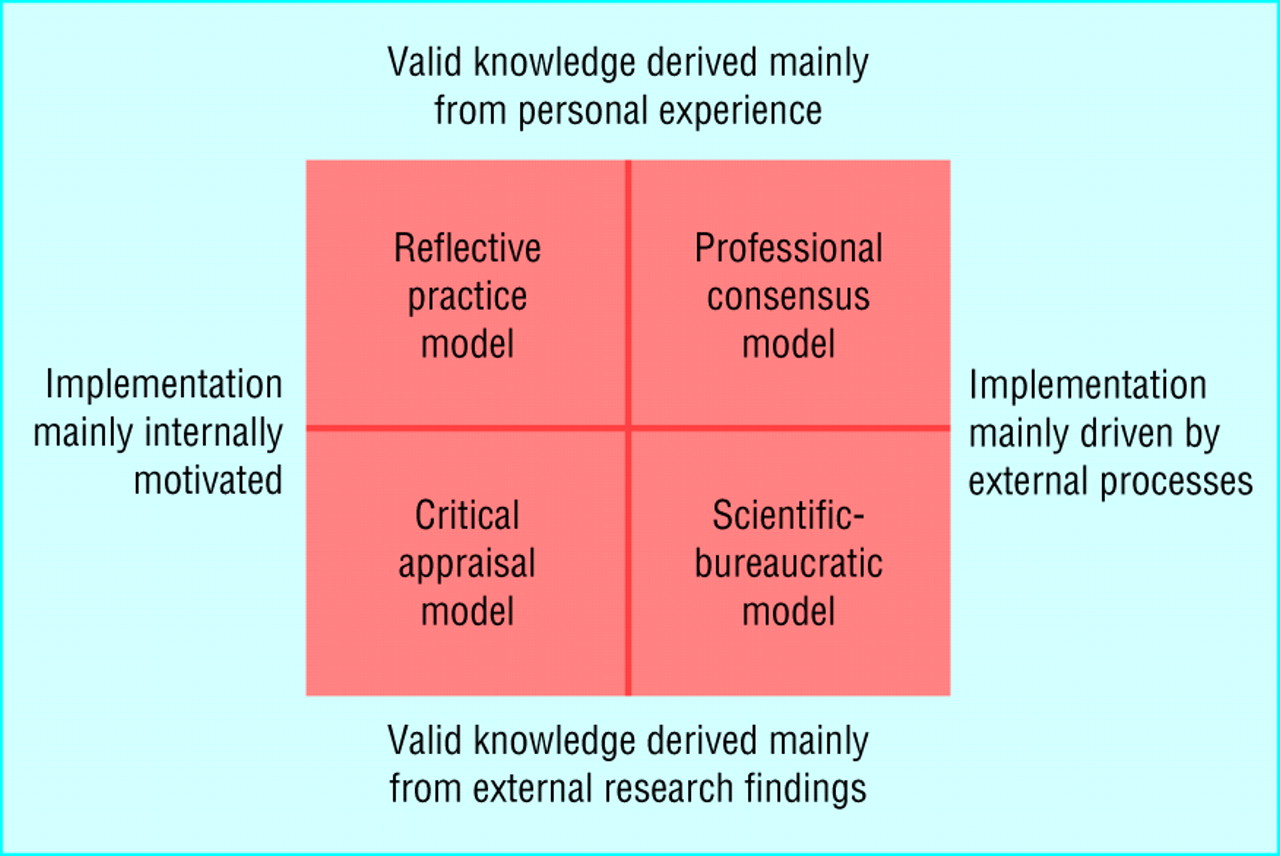
Medical practice can be characterised according to two different dimensions.23 Firstly, we can consider the extent to which valid knowledge is seen as tacit rather than explicit, derived from personal experience rather than systematic study. Secondly, we can identify whether the key drivers for implementation of that knowledge are individual and internal rather than external and collective. Combining these two dimensions gives rise to four models of medical practice—the reflective practice model, the professional consensus model, the critical appraisal model, and the scientific-bureaucratic model (figure). Although the descriptions of each represent “idealised types,” all of these are present in medical care to some extent, and the balance between them has changed substantially over time.

Models of medical practice (adapted from Harrison et al23)
{kind=link}
The reflective practice model represents a traditional view of medical care. Doctors provide care to patients on an individualised basis, adapting their practice in the light of ongoing experience and success. They work largely independently of organising structures and are less concerned with external formalised bodies of knowledge than with their own expanding clinical understanding and tacit knowledge.
The professional consensus model also emphasises accumulated clinical wisdom but consolidates this in the form of explicit guidance condensed from expert panels. Institutional arrangements may then be used to try to encourage a greater degree of compliance with these expert perceptions of “best practice.”
The critical appraisal model tackles some of the deficiencies of a knowledge base that is overly reliant on personal experience or expert view. Here, the emphasis is on externally generated, methodologically sound evidence, such as that derived from various clinical epidemiological studies. However, the implementation of such evidence is still left to doctors' individual discretion based on an integration of evidence with individual patient characteristics and preferences.
The scientific-bureaucratic model also emphasises robust, objective evidence but sees such evidence as being formalised into prescriptions for practice and models for service delivery. It brings this together with formal, externally driven strategies for implementation, thus reducing individual discretion about practice patterns.
Although each of these models remains in most healthcare systems, the scientific-bureaucratic model has risen in prominence in several countries over the past decade. 7 8 Modes of medical practice have been changing from individualised and sometimes idiosyncratic care underpinned by professional values to managed corporate delivery underpinned by more explicit bodies of knowledge. This change is the source of many of the current conflicts between doctors and managers.
A reliance on science applied through managerial processes may bring benefits—increased performance, improved efficiency, and greater uniformity. However, such benefits may come at a cost as a rigid formality may conflict with deeply held professional values such as autonomy, solidarity, flexibility, and a belief in tacit knowledge. A doctor's focus on individual patients is always likely to clash with the manager's need to take a more utilitarian view. More importantly, scientific-bureaucratic approaches to health care may induce a range of dysfunctions as well as being unable to cope with the complexity and context-dependent nature of health care.24 Such inadequacies and dysfunctions are likely to become more obvious as greater reliance is placed on a managerial approach.25
Conclusion
Substantial evidence now attests to the extent of doctors' unhappiness with the state of their relationships with managers and identifies some of the underlying dynamics.11 Although much of this evidence relates to the acute sector, similar tensions can be expected in primary care as primary care trusts begin to develop and the new general practitioner contract is implemented. We have shown that the current situation is both a culmination of longstanding trends in the NHS and part of a more general international phenomenon.
There are many reasons to tackle this discontent: disillusionment, lack of morale, loss of trust, misalignment, and miscommunication are hardly recipes for high quality patient care. If, as the government hopes, regulated markets and consumer choice are to be effective forces for improved quality and performance then this cannot happen without better alignment between doctors and the organisations in which they provide services.
The extent of cultural divergence between managers, doctors, and other professional groups suggests that such a realignment will be far from easy.26 Lay managers tend to favour a greater degree of rationalisation and transparency in work organisation than do clinicians,10 and managers with clinical backgrounds can find it difficult to combine their two divergent professional roles.19 None the less, despite the many good reasons that doctors may not wish to be involved in management, and the considerable tensions that arise when they are,14 further engagement is indeed needed.
Acknowledgments
Claire-Louise Hodges helped with searching and reviewing some of the literature underpinning this paper.
Footnotes
-
Funding The Nuffield Trust and the Commonwealth Fund of New York provided financial support.
-
Competing interests None declared.