Indigestion and non-steroidal anti-inflammatory drugs
BMJ 2001; 323 doi: https://doi.org/10.1136/bmj.323.7323.1236 (Published 24 November 2001) Cite this as: BMJ 2001;323:1236
- J M Seager,
- C J Hawkey
Non-steroidal anti-inflammatory drugs (NSAIDs) are usually thought to pose a dilemma for doctors wishing to prescribe them. Their anti-inflammatory and analgesic properties have led to their widespread use for rheumatoid and (much more commonly) other conditions often regarded as more trivial. However they are ulcerogenic to the stomach and duodenum and lead to a threefold to 10-fold increase in ulcer complications, hospitalisation, and death from ulcer disease.1

Three ulcers (one bleeding) in the gastric antrum caused by NSAIDs. Such ulcer complications are estimated to cause up to 16 500 deaths each year in the United States and 2000 deaths a year in Britain
{kind=link}
In fact, the dilemma is more complex than whether potentially life threatening drugs should be used to manage conditions that are uncomfortable but not in themselves life threatening. There is growing evidence that NSAIDs have other incidental benefits. The only study to investigate overall life expectancy with drug use found non-significant trends towards enhanced rather than reduced life expectancy. Aspirin has benefits in preventing cardiovascular disease and probably cancer that seem to far outweigh the hazards of gastrointestinal ulceration. Limited evidence suggests that these benefits may be shared by other NSAIDs.
NSAID use
About 24 million prescriptions a year are written for NSAIDs in the United Kingdom. Half of these are given to patients over the age of 60. At any one time about 15% of elderly people are taking an NSAID. Average prescribing rates are calculated to be 426 scripts per 1000 population per year.
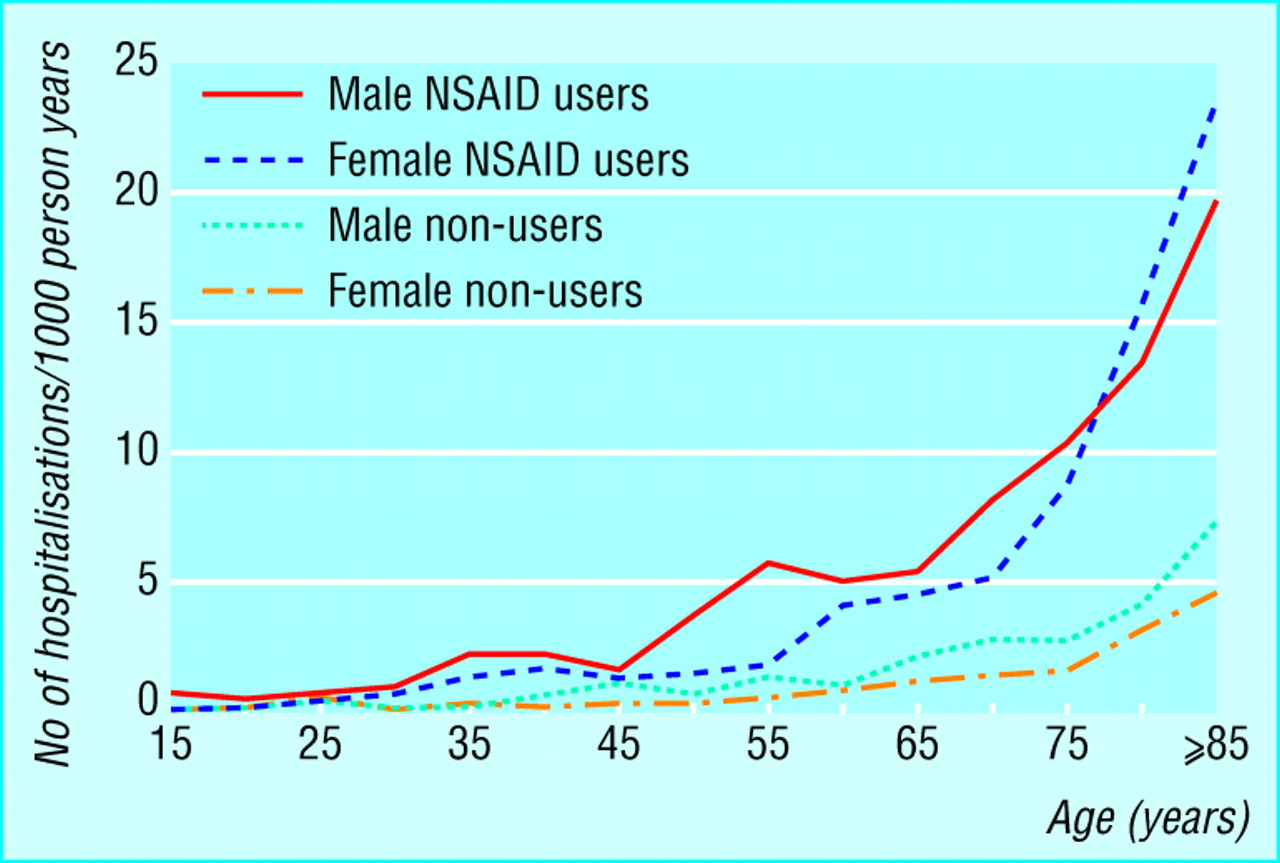
Hospitalisations due to complications associated with NSAID use are a problem in elderly patients
{kind=link}
Less than 10% of NSAIDs used in the community seem to be for rheumatoid arthritis, and less than half for any form of arthritis. They are widely used for acute soft tissue injury and more chronically for undiagnosed pains in the back and elsewhere. Chronic use is more common in elderly than younger patients, and prophylactic use of aspirin, mostly in relatively low doses, for cardiovascular events is increasing, amounting to 9.5% of a relatively elderly population.
Gastrointestinal toxicity of NSAIDs
NSAIDs are important in causing both (non-ulcer) dyspepsia and ulcers (often silent and presenting with a complication). The unreliability of dyspepsia as a pointer to ulceration underlies many of the problems of managing patients taking NSAIDs.

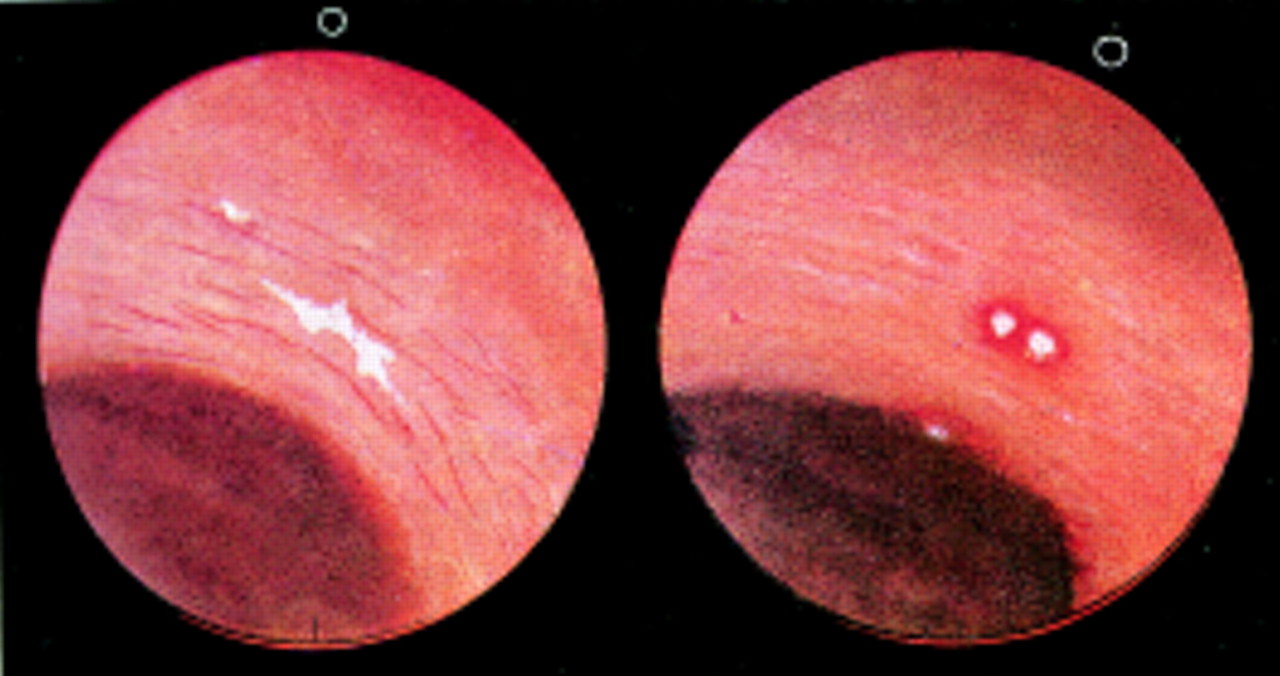
In 1938 Douthwaite and Lintott provided the first endoscopic evidence that aspirin caused gastric mucosal damage. Images show gastric antrum before (left) and after (right) administration of aspirin (reproduced from Douthwaite AH, Lintott JAM. Lancet 1938;ii:1222-5)
{kind=link}
Within 90 minutes of taking 300 mg or 600 mg of aspirin, nearly everyone develops acute injury consisting of intramucosal petechiae and erosions. Non-aspirin NSAIDs cause less florid acute injury, but endoscopic studies show that about 20% of those taking non-aspirin NSAIDs or aspirin at anti-inflammatory doses chronically have a gastric or duodenal ulcer. Many patients who start NSAIDs will not be able to continue because of drug associated dyspepsia.
Ulcers probably form and heal spontaneously in most NSAID users and usually cause little harm. However, about once in every 50–100 patient years, ulcer bleeding or perforation develops that requires hospitalisation.2 As a consequence, probably at least 1200 patients die each year in the United Kingdom.1
Who is at particular risk?
Risk factors for gastroduodenal ulcer complications are now fairly well defined. Most patients with NSAID associated ulcer complications are elderly. This is because elderly people have a higher background prevalence of ulcer problems, are more likely to receive NSAIDs, and are probably more sensitive to them. A history of ulcers (whether or not associated with NSAIDs) is a further risk factor.
Risk factors for gastrointestinal complications occurring with NSAIDs
Patient related factors
Age >60 years
History of ulcer disease
Drug related factors
Use of relatively toxic NSAID
High dose of NSAID (or two NSAIDs used concurrently)
Concurrent use of anticoagulant
Concurrent use of corticosteroid
Uncertain or possible risk factors
Duration of NSAID treatment
Female
Underlying rheumatic disease
Cardiovascular disease
Helicobacter pylori infection
Smoking
Alcohol consumption
A meta-analysis of recent studies shows that ibuprofen (≥1200 mg/day) is associated with a lower level of risk than other NSAIDs, whereas others such as azapropazone and piroxicam are associated with a higher risk.3 These differences probably relate at least in part to effective dose, since doses of ibuprofen greater than 1200 mg carry risks similar to those with other NSAIDs.3 Among NSAIDs in general, risks rise steadily with dose.3
As would be expected, the risk of ulcer bleeding is much higher if patients taking NSAIDs also receive warfarin. Interestingly, use of corticosteroids has been shown fairly consistently to magnify the risk of ulcer complications, to the extent that ulcers associated with NSAIDs and steroid may account for the probably incorrect belief that corticosteroids were themselves ulcerogenic.
Managing patients taking NSAIDs
Management of patients who need to take NSAIDs should be based more on assessment of risk than on clinical, laboratory, or endoscopic investigation. NSAID use should be avoided in patients with two or three of the risk factors for ulcer complications, or if this is not possible they should receive prophylactic treatment.
Comparative toxicity of NSAIDs for gastrointestinal complications*
Although development of dyspepsia soon after starting an NSAID may preclude its use and can sometimes lead to discovery of a previously silent ulcer, NSAID associated dyspepsia is generally a poor guide to the presence of an ulcer. Development of anaemia or new onset dyspepsia can identify NSAID associated ulcers, but upper gastrointestinal investigation is often negative and reliance on these signs will miss most ulcers, which most commonly present with complications on a relatively silent background.
Available drugs to treat ulcers
Preclinical studies in animals and humans suggest that two components contribute to development of NSAID associated ulcers. Firstly, inhibition of prostaglandin synthesis, by impairing mucosal defences, leads to erosive breach of the epithelial barrier. Secondly, acid peptic attack deepens this into frank ulceration, and pH is also an important determinant of passive NSAID absorption and trapping in the mucosa. Preventive treatment aimed at either mucosal defence or acid attack is available.

Inhibition of cyclo-oxygenase enzymes by NSAIDs relieves inflammation and pain but also removes mucosal protection of gastric epithelium
{kind=link}
Misoprostol is a stable analogue of prostaglandin E1. Several studies show that it prevents acute gastric injury by a wide variety of agents including NSAIDs. In doses of 400–800 μg daily misoprostol prevents gastric (and probably duodenal) ulcers. A large study has shown it to reduce the incidence of hospitalisation for NSAID associated gastrointestinal complications.2 Unfortunately, as a prostaglandin, it causes diarrhoea, abdominal cramps, and reflux at the doses necessary to protect against NSAID associated ulcers.
Acid suppressing drugs—Normal doses of H2 antagonists have relatively little affect on acute aspirin and NSAID associated injury in animals and in humans. High doses of H2 antagonists and normal doses of proton pump inhibitors are protective, and long term studies have shown them to prevent both gastric and duodenal ulcers. There have been no randomised studies of the effect of acid suppression on NSAID associated complications, although indirect evidence from epidemiology is encouraging.

Algorithm for managing gastrointestinal side effects of NSAIDs
{kind=link}
Choice of treatment
Patients with NSAID associated ulcers
If patients present with ulcers NSAIDs should be stopped if possible since they retard healing. For patients who need to continue taking NSAIDs, large comparative studies have shown that omeprazole 20 mg daily results in faster healing of gastric and duodenal ulcers than ranitidine 150 mg twice daily4 or misoprostol 200 μg four times daily and is better tolerated than misoprostol.
Subsequent prevention of relapse
Studies have shown that, once healing is achieved, NSAID associated ulcer relapse can be retarded by use of omeprazole, misoprostol, or high dose famotidine.4 These comparative studies—based on preventing the development of ulcers, multiple erosions, or moderate to severe dyspepsia—have shown overall higher efficacy for omeprazole 20 mg daily than misoprostol 200 μg twice daily or ranitidine 150 mg twice daily.4 In these studies omeprazole protected against ulcers, both gastric and particularly duodenal, and erosions. Misoprostol was associated with the same rate of duodenal ulcer formation as placebo but was particularly effective in preventing multiple erosions. In these studies the site of the initial lesion was a strong predictor of the site of subsequent relapse.
NSAID users without ulcers
Many studies have shown that misoprostol can inhibit ulcer development in such patients, as can famotidine 40 mg twice daily and omeprazole. These drugs have not been compared for relative effectiveness in this group of patients.
Side effects of NSAIDs
Dyspepsia
Oesophagitis
Oesophageal strictures
Gastric and duodenal petechiae, erosions, ulceration, bleeding, and perforation
Type C gastritis
Small and large bowel ulceration, bleeding, and perforation
Exacerbation of colitis
Practical prescribing
Patients presenting with gastric or duodenal ulcers who need to continue taking NSAIDs should be treated with omeprazole 20 mg daily or another proton pump inhibitor until the ulcer heals. Although omeprazole is the only proton pump inhibitor to have been studied in large scale trials, its benefits are probably a class effect. Patients with multiple erosions instead may be better served by misoprostol.
Overall, subsequent maintenance treatment is likely to be more effective and better tolerated with a proton pump inhibitor than misoprostol. Recognition that the site and nature of the original lesion is a strong predictor of the site and nature of relapse can aid management.

Chemical (type C) gastritis showing oedema and mild chronic inflammation of lamina propria and vertical smooth muscle fibres and slight foveolar hyperplasia. Contrast with H pylori induced gastritis, which has a marked neutrophil infiltrate in the lamina propria and deeper gastric glands
{kind=link}
For patients who present with duodenal ulcers a proton pump inhibitor is an appropriate maintenance treatment. For patients with multiple erosions misoprostol is appropriate if tolerated. On current data there is little to choose between proton pump inhibitors and misoprostol with regard to efficacy in preventing gastric ulcers, but proton pump inhibitors are better tolerated.
Role of Helicobacter pylori eradication
This is an extremely controversial topic. One study, of patients starting NSAIDs (naproxen) for the first time without a history of dyspepsia or ulceration, showed that eradication of H pylori substantially reduced the rate of gastric ulcer formation at two months. In another study, of patients who had previously had ulcers or moderate to severe dyspepsia, H pylori eradication did not influence outcome at six months. Finally, although omeprazole is effective prophylaxis in patients without H pylori infection, it is more effective in those who remain infected.4

Rofecoxib and celecoxib, selective COX-2 inhibitors, can relieve pain and inflammation without risking gastric ulceration
{kind=link}
Most doctors, feeling uncomfortable about persistent H pylori infection, eradicate it in NSAID users. In our view this is irrational if these patients are at sufficiently high risk to be candidates for co-treatment with acid suppressing drugs.
The future
A new generation of less toxic NSAIDs is probably imminent. Specific inhibitors of the inducible cyclo-oxygenase-2 enzyme (COX-2), which probably leave protective gastric prostaglandins uninhibited, are now available. Meloxicam, another recent NSAID, is well tolerated. Whether this is because it is a partially selective COX-2 inhibitor or because tested doses are low is uncertain. Other developments include NSAIDs that donate cytoprotective nitric oxide to the gastric mucosa.5
Conclusions
Currently, there is a wide range of views about what is an appropriate level of NSAID prescribing and no simple, all embracing resolution. In patients with risk factors for gastrointestinal complications the side effects of NSAIDs may outweigh all benefits. For such patients, omeprazole and misoprostol can provide effective protection, and the choice is between patients' generally poor tolerance of misoprostol and the higher costs of omeprazole. Finally, a growing concern is the correct management of low dose aspirin used for cardiovascular protection, and no patient studies have specifically investigated this.
NSAID protection strategies
Use lowest possible doses of NSAIDs
Use safer NSAIDs Low toxicity NSAIDs COX-2 inhibitors
Use NSAID prophylaxis Proton pump inhibitors Misoprostil
Footnotes
-
J M Seager is research pharmacist and C J Hawkey is professor of gastroenterology in the division of gastroenterology, University Hospital, Nottingham.
The ABC of upper gastrointestinal tract is edited by Robert Logan, senior lecturer in the division of gastroenterology, University Hospital, Nottingham; Adam Harris, consultant physician and gastroenterologist, Kent and Sussex Hospital, Tunbridge Wells; J J Misiewicz, honorary consultant physician and joint director of the department of gastroenterology and nutrition, Central Middlesex Hospital, London; and J H Baron, honorary professorial lecturer at Mount Sinai School of Medicine, New York, USA, and former consultant gastroenterologist, St Mary's Hospital, London.