Article Text

Statistics from Altmetric.com
Introduction
Hospital-based intensive care is known to be a significant driver of healthcare costs. In the USA, intensive care unit (ICU) care accounted for 13% of all hospital costs in 2005.1 One aspect of ICU care that has been found to be both a driver of cost and a measure of quality is ICU readmissions.1 As a result, readmission to the ICU within a single hospitalisation is now viewed by payers as a potential preventable complication, and payers are beginning to propose denial of charges associated with these episodes of care given the impact on length of stay (LOS) and hospital charges.2 Examples from the literature include data from an adult medicine multicentre database enquiry that demonstrated that patients who were readmitted to an ICU have a 2.5-fold increase in hospital LOS compared with patients who were not readmitted.3 Furthermore, Magruder et al 4 demonstrated a 128% increase in hospital charges associated with an ICU readmission, and this trend was present despite risk adjustment for patient severity of illness.4
Over recent decades there has been a significant reduction in the congenital heart disease mortality rate.3 As a result, increasing emphasis has been placed on reducing morbidity and identifying markers of care delivery such as hospital LOS and incidence of hospital readmission.5 The paediatric cardiac population is at particular risk for in-hospital deterioration and subsequent readmission to the cardiac intensive care unit (CICU).6 However, while studies have described that in-hospital readmission to the paediatric CICU is associated with mortality,5 6 there is little data on efforts aimed at preventing these readmissions. It is notable that benchmark data do not exist for this metric; however, our internal single-centre data demonstrated that 2.8% of our patients who were transferred from the CICU to the cardiac step-down unit were readmitted to the CICU within 48 hours.
Through observation of our own internal CICU to cardiac step-down unit processes, we identified that standard transfer of care and monitoring practices were not differentiated based on patient-specific risk. We hypothesised that undifferentiated monitoring of all patients regardless of risk allowed subtle clinical changes to go unrecognised until the needs became more urgent, resulting in more invasive and complex interventions such as readmission to the CICU. Our aim was to develop, test and measure compliance with standardised transfer of care processes for higher risk paediatric cardiology patients. We hypothesised that compliance with standardised care processes based on risk or condition would reduce in-hospital readmissions to the CICU within 48 hours of transfer.
Methods
Improvement team
In November 2014, we established a multidisciplinary improvement team between the CICU and the cardiac step-down unit, which would eventually become known as the Transfer Workgroup. The team comprised key stakeholders including nursing leadership, bedside nurses (registered nurse (RN)), nurse practitioners (advanced practice registered nurse (APRN)), quality outcomes managers and physicians (MD). The team was formed to address the transition of patients between the CICU and the cardiac step-down unit. Initial steps were focused on review of the processes involving patient transition between both cardiac units, as well as review of potential gaps in practice and identification of areas for improvement. From this analysis, the group identified the historical <48-hour CICU in-hospital readmission rate, which was viewed as potentially modifiable.
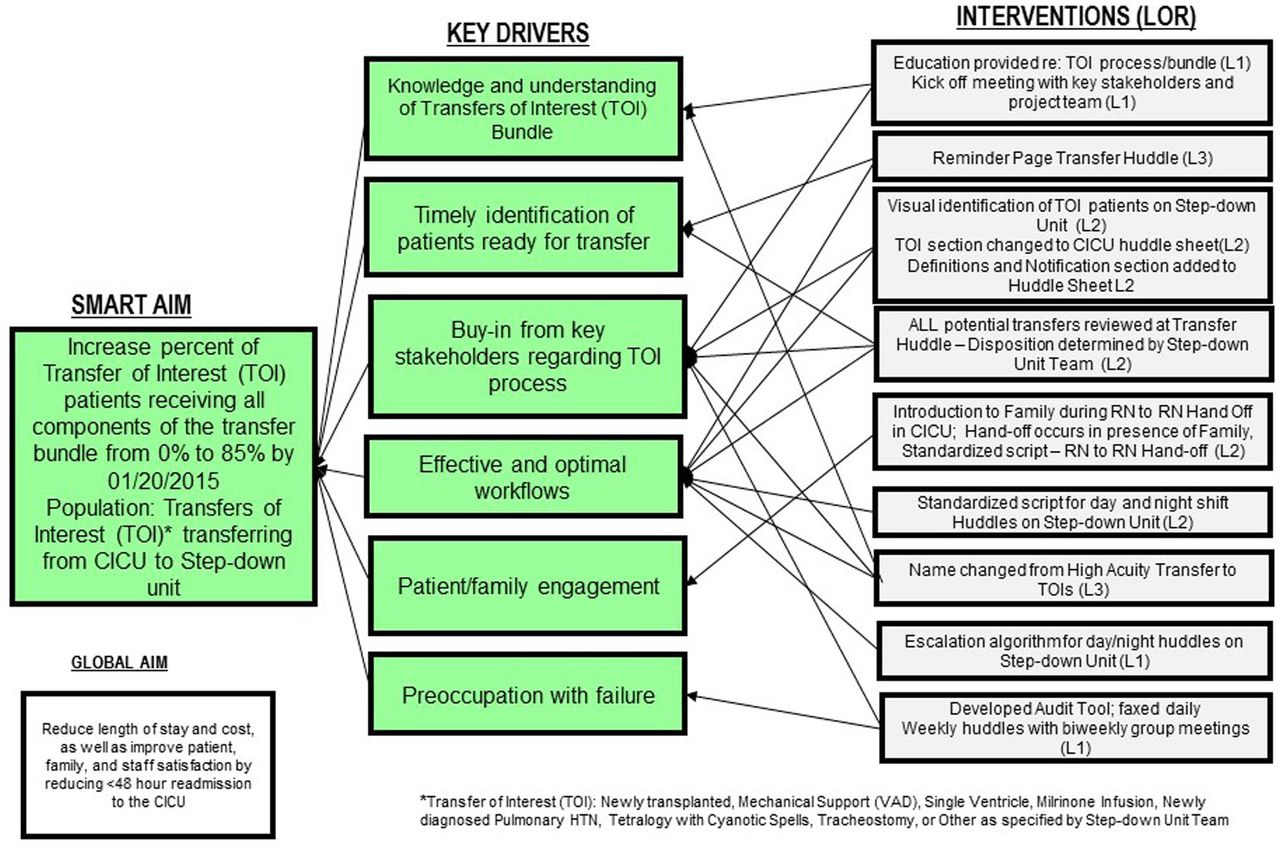
Using the Model for Improvement, the team defined global and smart aims, and developed a key driver diagram to guide our improvement work (figure 1).7 For each driver, the team defined potential interventions and subsequently tested each by using Plan-Do-Study-Act (PDSA) cycles to enable improvement strategies to be tested and refined.7 8 Effective interventions were adopted and unsuccessful tests were adapted or abandoned. At the conclusion of the testing phase, a new process map was established representing the new system of care (figure 2).

Key driver diagram. CICU, cardiac intensive care unit.

Transfer process prior to project initiation. CICU, cardiac intensive care unit; RN, registered nurse; TOI, Transfers of Interest.
Setting
The CICU and cardiac step-down units are both components of the Heart Institute (HI) at our organisation. The CICU is a 25-bed unit with an average daily census of 16.3 for 2015. The CICU personnel includes 8 physicians, 119 nurses and 10 nurse practitioners. The cardiac step-down unit is a 17-bed unit with an average daily census of 14.5 for 2015. The cardiac step-down personnel includes 12 physicians, 48 nurses and 10 nurse practitioners. There are a total of 14 categorical cardiology fellows in the HI. The total number of transfers from the CICU to the cardiac step-down unit in 2014 and 2015 was 493 and 564, respectively.
Previous to this improvement project, all transfers out of the CICU to the cardiac step-down unit were managed according to the same set of processes. The patients listed to be transferred were communicated at the time of transfer rounds in the CICU (11:00 daily). The primary ICU provider responsible for the patient’s care provided the sign-out in the CICU with the following persons expected in the audience: CICU attending and charge RN, as well as cardiac step-down attending, fellow, APRN/paediatric resident and charge RN. Once sign-out was complete, no formal methodology existed for the remainder of the care that day (both pretransfer and post-transfer). Bedside RN communication between units was by a non-standardised phone call. There was no formal inclusion of the cardiac step-down overnight care team.
Our organisation has a mature quality improvement infrastructure within our Center for Health Systems Excellence. Hospital faculty and staff are trained in improvement science via multiple course offerings. Quality improvement consultants and data analysts provide assistance for many improvement projects.9
Improvement
Sources of failure in the CICU to the cardiac step-down transfer process, which were postulated to contribute to the <48-hour CICU readmission, were as follows:
Lack of a standardised approach to assessment, identification or special care considerations for complex or vulnerable patients at the time of transfer, variable application of patient criteria for when to transfer patients
Incomplete communication (MD/APRN providers with bedside RN, CICU RN to cardiac step-down RN and cardiac step-down day shift to night shift RN) regarding significant events or concerns during clinical course
Lack of standard cardiac step-down vital sign and fluid balance tabulation frequency
Lack of standard RN:patient assignment ratio
Variable approach to escalation of changes to the patient’s clinical condition.
We reviewed all <48-hour CICU readmissions between January and June 2014 to identify patterns or themes in patients with unplanned readmission to the CICU within 48 hours of transfer. As a result of this assessment, key conditions and therapies appeared more prevalent in this population and were used to establish a key driver diagram to address the <48-hour CICU readmission rate. The Transfer Workgroup identified this unique population and coined the patient identifier ‘Transfers of Interest (TOI)’ (table 1).
Patient condition categories that generated a label of ‘Transfers of Interest’ (TOI)
The key drivers identified included (1) knowledge and understanding of TOI bundle, (2) timely identification of patients ready for transfer, (3) buy-in from key stakeholders regarding TOI process, (4) effective and optimal workflows, (5) patient/family engagement and (6) preoccupation with failure (figure 1).
Interventions
Interventions were tested through PDSA cycles and categorised as level of reliability 1 or 2 as evident in the key driver diagram. Reliability level refers to the capability of a process, procedure or health service to perform its intended function in the required time under existing conditions. Level 1 in this context refers to processes classified by 80%–90% reliability (1–2 failures out of 10 opportunities). Level 2 processes are approximately 95% reliable (<5 failures out of 100 opportunities), and Level 3 processes are approximately 99% reliable (<5 failures out of 1000 opportunities). The result of these interventions was the creation of the TOI patient care bundle (box 1).
TOI bundle components
Early identification of TOI patients prior to transfer (24 hours)
Deliberate RN:patient ratio assignment (first 24 hours after transfer) and no greater than 2:1
Cardiac intensive care unit RN to cardiac step-down RN face-to-face handoff
Day shift bedside huddle on cardiac step-down unit including cardiology attending and fellow, APRN/paediatric resident, charge RN and bedside RN (performed at bedside)
Every 2-hour vital signs and every 4-hour intake and output assessment the first 24 hours after transfer
Night shift bedside huddle on cardiac step-down unit including cardiology fellow, APRN/paediatric resident, charge RN and bedside RN (performed at bedside)
APRN, advanced practice registered nurse; RN, registered nurse; TOI, Transfers of Interest.
Several failures were noted early and their reduction was critical to the ultimate progress of this quality improvement effort. Most prominent was the initial language used to label the category of patients to be transferred. As the project took shape, these patients were initially termed ‘high acuity patients’. During this early period, there were consistent failures regarding the early identification of the patient population. In addition, there was frequent concern on the part of the cardiac step-down RN staff that these patients were too ill for their unit. This RN hesitancy led to highly variable adoption of early testing. After identification of these repeat failures, the Transfer Workgroup relabelled the patients as TOI without changing the inclusion criteria. This change in perception led to immediate gains, and there was a near instant improvement in the capacity to conduct testing and interventions. We believe the terminology shift from ‘high acuity’ to TOI was more readily adopted because it did not rely on the CICU labelling patients as higher acuity, which was viewed negatively by the step-down staff. Rather, TOI status was determined by the step-down unit, which fostered buy-in and accountability for compliance with the TOI bundle.
Study of improvement, measures and analysis
In order to measure improvement, the study included both outcome and process measures. A baseline period of January 2014 to September 2014 was preselected prior to the commencement of improvement work. The primary process measure was compliance with all of the six TOI bundle components, referred to as an all-or-nothing measure. Compliance with each individual component was also measured. All bundle components were tracked on run charts with a goal of 100% adherence with the entire TOI bundle in at least 85% of all patient transfers. The outcome measure, readmission to CICU within 48 hours, was measured by a days between readmissions control chart (T-chart), which is particularly useful for measuring rare events.10 Statistical process control methods were used to monitor changes in care processes. Weekly data were reviewed for the all-or-nothing measure, as well as each bundle component, to enable early detection of failures and evaluation of the interventions that were being tested. Run charts and control charts were created and annotated to track interventions tested throughout the project. Standard industry criteria were used to determine whether observed changes in measures were chance random variation (common cause variation) or due to a specific assignable cause (special cause variation).10 11 Care was taken to assess balancing measures such as patient condition on in-hospital CICU readmission, LOS (overall, as well as CICU-specific and cardiac step-down-specific) and all-cause 30-day hospital readmission, none of which were adversely affected as a result of this improvement effort.
Sustainability
In an effort to sustain the progress of the TOI project, the team employed three strategies: adoption of specific TOI components thought to be most beneficial for all CICU to cardiac step-down transfers regardless of patient condition (day shift bedside huddle and RN-to-RN handoff), a preoccupation with failures, and an invitation to patients and family members to join the day and night shift huddles. Control charts were shared routinely at Transfer Workgroup meetings and monthly RN staff meetings. Progress was shared twice yearly at inpatient quality improvement presentations. Results were communicated for monthly analysis by leadership. Members of the Transfer Workgroup evaluated all failures in real time. Nurses and providers were contacted shortly after the encounter, and learnings were shared and implemented when indicated.
Human subjects protection and ethical issues
The present initiative fell within the Institutional Review Board’s guidance for quality improvement projects that did not constitute human subjects research. The study of the interventions for this quality improvement effort did not compromise patient privacy as all persons involved were previously present in the care of these patients.
Results
During the entire study period (January 2014–December 2015), 1118 patients were transferred from the CICU to the cardiac step-down unit (average of 47 per month). During that time, there were a total of 24 separate <48-hour readmissions to the CICU (rate of 2.2 per 100 transfers). For the purpose of this study, the baseline period was January 2014–September 2014, and during this baseline period there were 400 patient transfers from the CICU to the step-down unit and 11 separate <48-hour readmissions (rate of 2.8 per 100 transfers). The improvement period after the TOI intervention was October 2014–December 2015, and during this phase there were 718 transfers from the CICU to the step-down unit and 13 separate <48 readmissions (rate of 1.8 per 100 transfers). From the baseline period to the improvement period, the days between <48-hour readmissions increased from a median of 18 days to 37 days (figure 3). During the improvement period, there were four separate special cause events as defined by control chart rules whereby any single point outside of the control limits is considered special cause.10 11
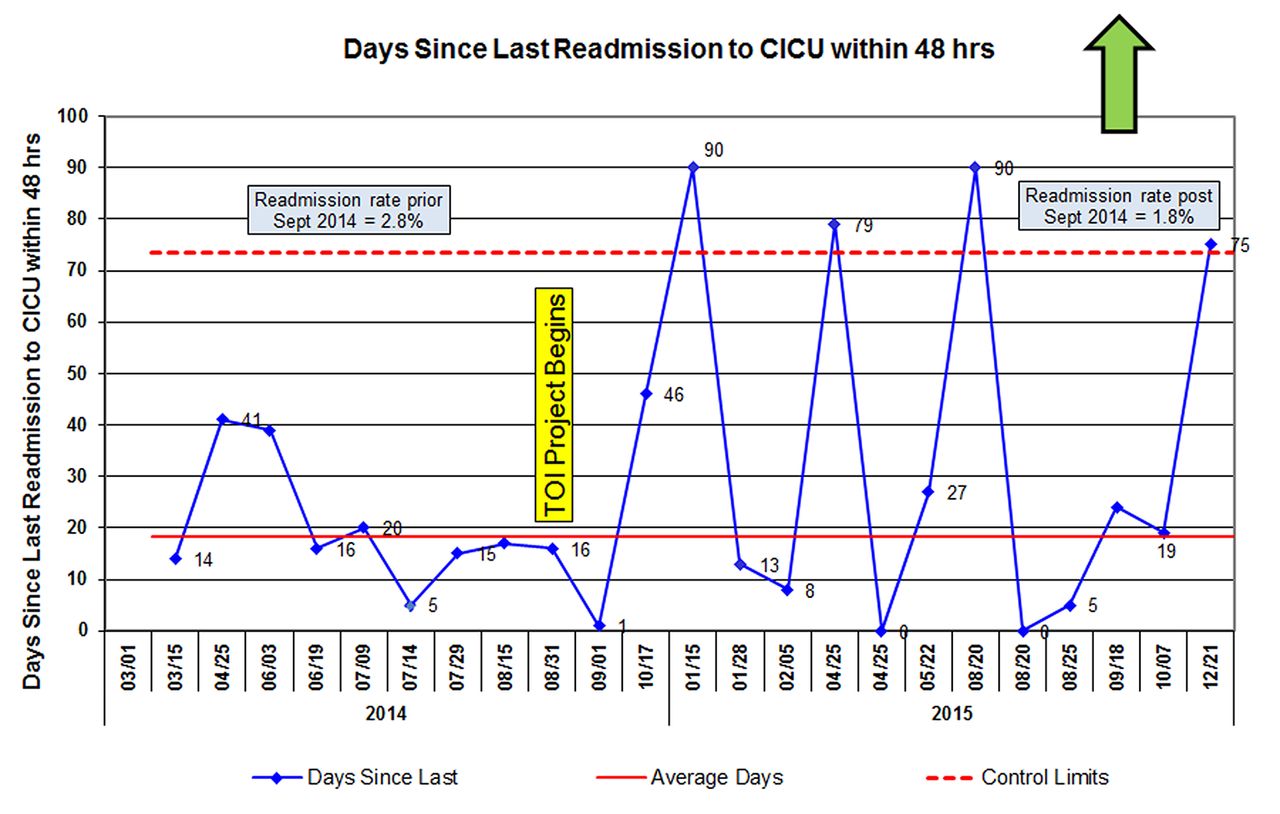
Days since last readmission to CICU within 48 hours. CICU, cardiac intensive care unit; TOI, Transfers of Interest.
Throughout the improvement period, there were 102 patients who were identified as a TOI. From October 2014 through December 2015, an average of 94% of transferred patients (median 100%) received the complete bundle, exceeding the project goal of 85% (figure 4). While we measured our compliance with the entire bundle as an all-or-nothing measure, we also measured the failures of each component of the bundle and monitored those in a Pareto chart (not shown — most common failures were ‘Early Identification’ and ‘RN staffing’). Balancing measures, collected to verify that the TOI intervention had not negatively impacted other patient safety metrics, demonstrated an unchanged rate of rapid response events (2.0 per 1000 patient days), an overall decreased all-cause 30-day hospital readmission rate (16.3% to 13.4%)%) during the study period, and a decrease in average length of hospital stay by 2.2 days for surgical cardiac patients, with no change in LOS for medical cardiac patients.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Transfer bundle compliance.
Discussion
Using the Model for Improvement, our study demonstrated a reduction in <48-hour readmissions to the CICU after the development and testing of a new care process practice bundle. Our study demonstrated that the bundle was sustainable in a busy tertiary paediatric cardiology setting, and that it led to a significant decrease in the frequency of these clinically important events without interfering with other quality outcome metrics, such as LOS or rapid clinical decompensation.
It is recognised that in-hospital readmission to the ICU has been associated with increased LOS, increased cost and increased mortality. Previous studies have focused primarily on identifying factors or conditions associated with increased risk of readmission to the ICU, the effect on mortality or to identify all-cause hospital readmissions.1 4 6 12 13 Despite the negative effects of in-hospital ICU readmission, reports of system modifications to prevent these events are limited. Our efforts were instead focused on interventions surrounding the transfer of care for higher risk cardiac patients transferring from the CICU to the cardiac step-down unit in a direct attempt to decrease the rate of CICU readmission. While our process does not allow for identification of which particular bundle elements (or combination of elements) are responsible for the increase in time between CICU readmission from 18 to 37 days, there was nonetheless a shift in our rate of <48-hour readmission. Based on our findings, the creation and use of a standardised transfer-of-care process based on patient condition may play an important role in reducing in-hospital CICU readmissions. It should also be noted that while there were four separate data points outside of the control limits indicating a change from baseline performance, it is unclear whether these gains will be sustained over time and will require ongoing monitoring to fully appreciate the significance of the improvement.
We elected to create an intervention after our series of PDSAs that relied on an all-or-none bundle compliance process measure. While this method is vulnerable to the effects of poor adherence to individual components of the bundle, we were able to achieve a high rate of compliance. As a result of this approach, we gained valuable insight into the complexities of the individual process measures in terms of the interdependence. Specifically, two components of the TOI bundle included RN-to-RN in-person handoff and enhanced RN staffing for identified patients for the first 24 hours following transfer, and the ability to reliably comply with these individual components of the bundle was entirely dependent on a third bundle element, the early identification of the TOI patients. As a result, we believe that the all-or-none approach to the overall bundle compliance was critical to the success of the intervention.
Leveraging previously well-established or highly valued processes to introduce tests of change likely buttressed the success of our intervention. In addition, it proved beneficial, when trying to gauge effectiveness of a test, to gain buy-in from key process stakeholders. For example, communication regarding early prediction of TOI patients occurred during existing forums, including daily huddles, and was led in combination by the charge nurses of each respective unit. Huddles were a routine activity for the CICU and step-down unit and felt to be the ideal setting to discuss these upcoming transfers. Additionally, engagement of key stakeholders, specifically direct care staff, in the design and testing of interventions enhanced the perception of the value of the change. Direct care staff and families verbalised the importance of RN-to-RN in-person handoff at the bedside, and compliance with this bundle element was readily achieved despite the significant change from previous workflow. Similarly, the new day and night huddles at patient’s bedside after arrival to the step-down unit were also felt to be of substantial value to the healthcare team and were readily adopted as a consequence. These day shift huddles have since been spread to all patient transfers in a slightly modified form in terms of individual participants. Frequent updates regarding performance and progress to date served to keep team members engaged and motivated in the improvement effort. Lastly, the importance of a multidisciplinary team effort should not be underestimated. This was a team effort and not a discipline-specific problem to solve, and we believe this contributed greatly to the success of this project.
A limitation of the transfer of care bundle approach is that we were not able to identify which of the six elements of the bundle was most predictive of preventing <48-hour in-hospital readmissions to the CICU. Additionally, it should also be noted that improvement efforts focused on <48-hour in-hospital readmissions exclusively, and we did not measure all in-hospital readmissions to the CICU following transfer. As a result, we are not able to determine if the interventions employed were effective at reducing all in-hospital readmissions to the CICU. In addition, after the initiation of the TOI bundle, we did still have 13 separate <48-hour readmissions, which indicates that while our rate improved, it did not eliminate these events. As a result, we have initiated, as part of the routine activity of the Transfer Workgroup, a process to examine each <48-hour in-hospital CICU readmission for its preventability. Our aim at this time is to examine if there are certain characteristics that occur with some regularity that may be modifiable. Lastly, this was a single-unit improvement study and may not yield the same results in other setting.
Despite these limitations, over the course of this improvement period, the average LOS for our cardiac surgical population decreased by 2.2 days, suggesting that the improvement was not the consequence of holding patients in the CICU for a longer period of time prior to transfer. In addition, the number of medical response team activations did not increase. This is an important finding given that our organisational philosophy is to activate early to provide early intervention, rescue and stabilisation for clinical decompensation. During this improvement period, the overall <30-day readmission rate to the hospital decreased as well. While we recognise this may not correlate directly with our particular improvement project, it is important to note that we did not see an increase in readmission rate for complications missed during the index hospitalisation.
Future efforts include enhanced prediction of patients at risk, identifying preventability of all <48-hour in-hospital readmissions, the creation of transfer readiness criteria and the spread of bundle components to other patient populations and hospital systems.
Conclusion
Reducing the rate of <48-hour in-hospital readmission to the CICU is possible within a tertiary care setting. We believe we were able to accomplish this by (1) better prediction of those patients most at risk for readmission and (2) providing targeted interventions to effectively mitigate risk factors. Reducing LOS and cost, while improving patient experience, remain key priorities for our institution, and we believe that the TOI bundle is an effective tool in this mission.
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.