Article Text

Statistics from Altmetric.com
Improvements in health services require a range of technical skills, but like all complex organisational tasks they also rely on the personal skills and attitudes of the staff carrying out the changes. That much is axiomatic.1 2 3 Less certain, but surely potentially helpful to front-line staff undertaking improvement initiatives, is ascertaining just what might be the right sets of skills needed for different kinds of improvement tasks in varying circumstances.4 5 6
Useful insights into the ways in which a range of organisational circumstances demand such skills were exposed when the Heath Foundation, an independent charity working to improve healthcare quality in the UK, funded our project to help local ‘improvement groups’ learn how to bring about specifically agreed developments, while simultaneously observing how the improvements worked out. By formatively evaluating the processes involved, the intention was to help the Health Foundation promulgate improvement skills more effectively in future. The methods that we used are briefly summarised in box and have been published fully elsewhere along with the details of the sites, participants, processes and outcomes.7 In brief, two National Health Service (NHS) sites were chosen for being exceptionally well primed, due to their apparent excellence in continual quality improvement, to benefit from extra funding, facilitation and expertise aimed at helping them make better use of ‘improvement science’.8 The expectation was that the focus would be on technical skills (such as rapid improvement cycles, process mapping, tailored outcome measures and data analysis), which would be made available as needed through the Health Foundation’s extensive network of improvement experts.
Methods
Once we had carried out our orientation interviews and got to know the two organisations, the authors (four senior academics specialising in qualitative health services research and service development) helped each site to identify a clearly delineated improvement task in each of two suitable clinical areas (table 1). We then, using snowball sampling, interviewed the relevant staff involved (n=9–13 per improvement group, each group consisting mainly of senior health professionals with significant additional managerial roles) to elicit their views about their service, the proposed improvements, the intended tasks and the likely skills involved. Having separately thematically analysed each set of interviews we presented the findings back to each improvement group and used consensus methods to help them identify and prioritise the improvement skills they felt they lacked. We then arranged interactive learning events designed to help them acquire and apply those skills. This process was repeated as necessary throughout our project, which involved us in participant observation of 9 learning events, 10 group meetings and 35 further interviews—all designed to help develop and formatively evaluate the learning and the progress of the improvements. Between 3 and 9 months after our involvement ended, we conducted 33 follow-up interviews to ascertain subsequent progress and the participants’ reflections on the skills and learning involved.
The sites’ improvement projects
The two organisations had starkly contrasting approaches to quality improvement (table 2). The Dansworth senior managers, who had for many years inculcated what they called a ‘quality improvement culture’, had established strongly supported improvement structures and a core of local clinical enthusiasts well versed in methods of improvement science, who were spreading their philosophy. In contrast, the Furnhills executive drove change mainly through contracts; it was their nationally renowned prowess as healthcare commissioners that underpinned their considerable service improvements. While ostensibly signed up to clinical engagement and ownership, Furnhills’ (impressive) improvements were due more to top-down target-led performance management.
Examples of the contrasting approaches to quality improvement
These contrasting cultures had an overarching influence that resulted in a very wide range of organisational ‘microclimates’ across the four groups, which allowed us to explore the exceptionally disparate local cultures and processes shaping the execution of their improvement work. Our thematic analysis suggested, as have others,9 10 a number of organisational factors that impacted strongly on the projects. We identify here seven key factors, the handling of which we found demanded more than just technical skills of quality improvement. As the following examples illustrate, it was complex organisational and personal skills, as well as the ability to learn collectively, that mainly shaped the improvement groups’ success or failure.
External environment: A nationally imposed NHS restructuring meant that Furncop’s work became entangled with job insecurities and turf battles over the leadership of the improvements to chronic obstructive pulmonary disease (COPD) care, which repeatedly threatened to undermine the project. Overcoming those problems in Furnhills required formidable political, negotiation and stress management skills, not to mention extraordinary resilience. In contrast, untouched by that national upheaval, Dansworth remained organisationally stable but was experiencing strong external pressures to improve dementia care, leading to a welter of local initiatives that overwhelmed Dandem’s original improvement task. Time management and prioritising, as well as understanding vested interests and power bases, became essential, as did the necessity of communicating across sectors that were unused to planning services together.
Internal environment: The initial manager of the Furncop project was a strong advocate of Furnhills’ top-down approach to quality improvement. But her nursing team found that being directive was counterproductive when trying to persuade primary-care general practitioners (GP) to reach the stated targets for COPD care; so against their manager’s wishes the nursing team often used a more collaborative improvement approach. The consequent tensions between manager and team all but negated their deep sense of team loyalty and dedication to the improvement mission. When the manager left, a locally prominent GP took over; she championed the respiratory nurses’ collaborative approach, but she and the now cohesive team found themselves struggling against Furnhills’ hierarchical insistence on target-led performance-management methods. Finding a way through that continuing tension was crucial to the project’s eventual progress. The Danelder group had no such problems; they and their Dansworth senior managers were wedded to collaborative methods. However, they found themselves paralysed by the bruising that a recent internal restructuring had inflicted on the ward staff. Understanding those psychodynamics allowed the leader of the hospital team to use the improvement project skilfully to heal the wounds and re-establish cohesion. Even so, it then took considerable skill and facilitation to establish the cross-organisational connections and mutual learning necessary to smooth the discharge of elderly patients into the community. They succeeded by bringing together a disparate multisectoral workforce, something that the Dandem project, working in a different part of the same organisation, had difficulty in achieving. So unlike Danelder, the Dandem work made minimal progress towards its agreed improvements.
Internal structures and processes: Dandem’s improvement learning events never got beyond a preliminary exchange of knowledge and proposals about the services in the different sectors, whereas the staff executing the Danelder project rapidly forged a team approach that enabled them to access and implement the necessary improvement techniques together. Why the difference? The Dandem project leader, being somewhat new and on the fringes of Dansworth’s core organisation, had not been exposed to the prevalent improvement culture and was unable to exploit the available structures and processes. In contrast, the Danelder project leader and many of the participants were steeped in Dansworth’s long-standing improvement culture and had the improvement resources at their fingertips.
Local politics: The Furndem group seemed reluctant to tackle the key concerns about the unacceptably high waiting list for their hospital-based memory clinic because they worried that the commissioners were wanting them to compromise the exceptional quality of care that patients received once at the front of the queue. Moreover, they blamed GPs for the backlog, and so for almost the whole duration of the project they rejected the GPs’ perceptions of their service’s limitations. The protracted politics of establishing a constructive dialogue proved the key to the sudden service transformation that finally occurred. The Furncop work was similarly caught in local tensions between primary and secondary care, as well as the politics of an executive trying to stamp its new-found authority on all teams managing long-term conditions, including COPD. A final example was a manager who failed to properly engage a key party who consequently, when later handed responsibility for completing the agreed improvement task, felt no ownership of it and sidelined it.
Leadership: The original leader of Furncop was backed by her senior managers but neither the GPs nor her own team of nurses were willing to follow the improvement methods she advocated. Her eventual successor, a prominent GP, although fully supported by her fellow GPs and the nursing team, found herself having to resist being undermined by the senior performance managers. Thus, difficulties in the leaders’ roles—whether managing upwards or downwards—impeded the project under both regimes. Leadership played a major part also in another of the projects where the director’s reluctance about the project was completely reversed when a charismatic GP enthusiast eventually took a leadership role and the improvements suddenly forged ahead. Project leadership likewise had contrasting impacts in Dansworth. The Danelder project, which more than achieved its goals, owed much of its success to being led by a well-trained quality improvement (QI) champion, empowered to focus on the task and respected by her team. The leader of the unsuccessful Dandem project was, in contrast, swamped by other tasks, distant from the improvement culture, not empowered to lead the necessary multisectoral change, and still (patchily) building respect.
Relationships: The relative status of Furncop’s respiratory nurses and their target GPs meant that the nurses required consummate assertiveness, negotiation and persuasion skills to alter the GPs’ behaviour. Similarly, Danelder emphasised the need for assertiveness skills to help hitherto disempowered junior staff to contribute to decisions about discharging patients. In Furndem, lack of trust—and consequent stand-off—between the healthcare commissioners, the memory clinic group and the GPs blocked the project for nearly a year until a productive dialogue was finally enabled. Finally, all four projects benefitted from groups of staff coming together, sharing information and learning to hear each other’s concerns and to plan together where they had previously not made time for—or had actively avoided—such joint working.
Educational style: Furnhills’ top-down management style was mirrored by their approach to training in QI; it relied on a central committee, large high-profile set-piece events and didactic training sessions. None of these had any positive impact on either of the Furnhills’ projects. In contrast, the success of the Danelder team was crucially underpinned by Dansworth’s focus on nurturing capable enthusiasts who engaged in widespread exchange of practical knowledge and experience with their peers, and on developing quality through on-the-job coaching, mentoring and masterclasses, all of which laid the foundation for quickly and easily implementing the necessary techniques.
Our analysis of the entire qualitative data set suggested that all the projects, in the face of the organisational challenges they faced, needed to deploy three sets of skills. The improvement groups’ abilities to use the first set, the technical skills of improvement science, always depended on the other two sets—their ‘soft’ skills and their learning skills. The above examples, in which all the improvement tasks were engulfed by most if not all of the seven organisational factors that we identified, show how the participants needed to employ the full range of fundamental personal and organisational ‘soft’ skills. Besides the communication, assertiveness, negotiation, time management, prioritising, stress management, leadership, ‘people-reading’ and team skills mentioned above, ‘soft’ skills also included organising and administrative skills grounded in a good deal of local knowledge about people, places and how the informal systems work. Where those skills were absent, the improvements stalled. Where they were appropriately applied, as in the Danelder project or the final stage of Furndem, the improvements were achieved. The successful exploitation of those skills relied also on the third skill set, the learning skills that dictated the groups’ abilities to openly share their practical, contextual, tacit knowledge, for example, through reflecting on their experiences through story swapping and observation, and being willing and able to learn collectively with and from a range of colleagues so as to share and absorb each other’s experiential knowledge about the local system (table 3).
Examples of changes in learning skills in the facilitated improvement teams
This shift in learning styles was an aim of the facilitation provided by our team, and in the final evaluation interviews was frequently highlighted as having been a major beneficial change. But it was something that the Furndem, Furncop and Dandem participants found very difficult at first. Nevertheless, with suitable facilitation it ended up at the heart of any eventual progress they made. Collective learning was also crucial to the success of the Danelder project. Their achievement relied strongly on their ability to learn from open critical reflection, and to be willing, in short, to behave from the start as a community of practice, and to spread that ethos more widely.11 12
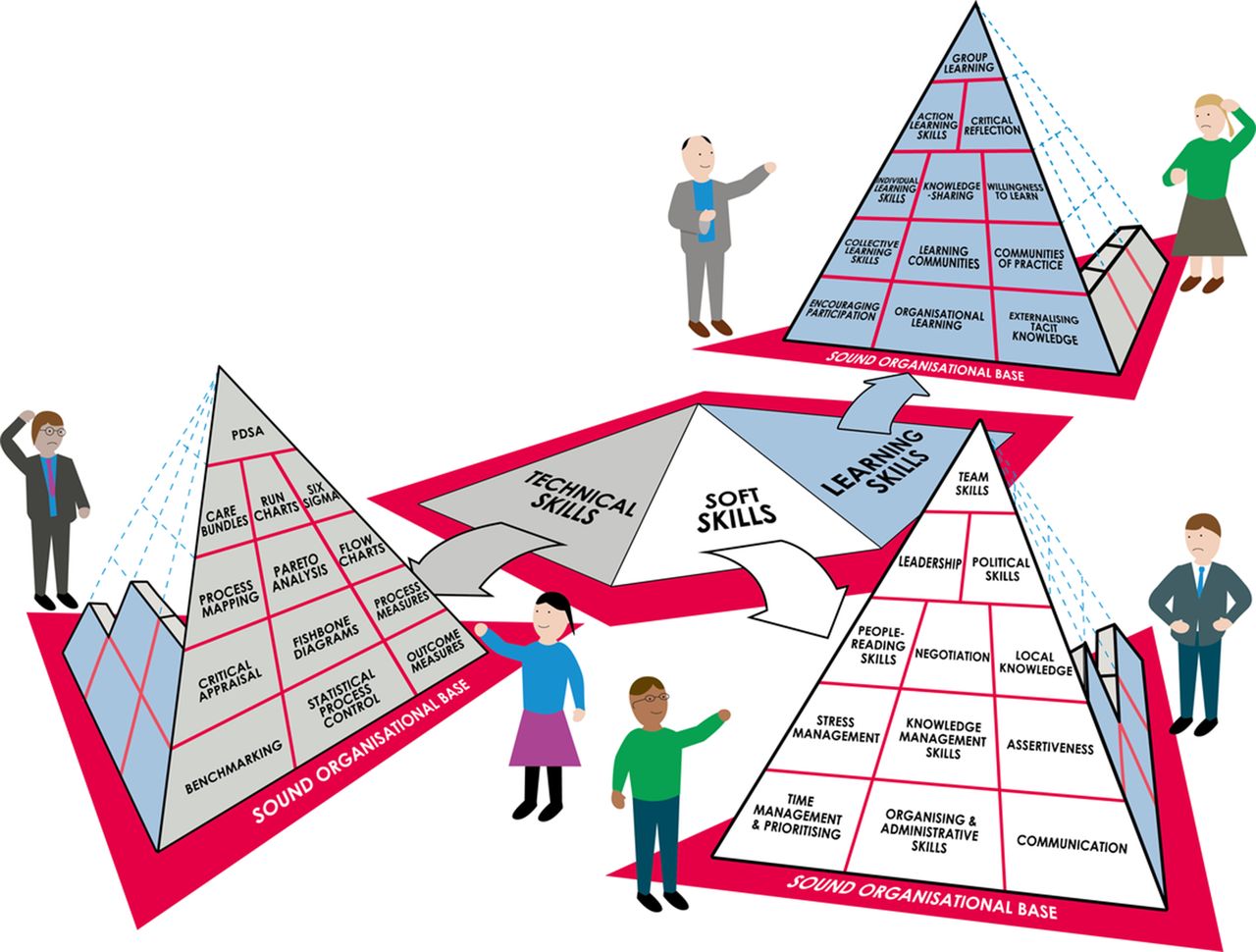
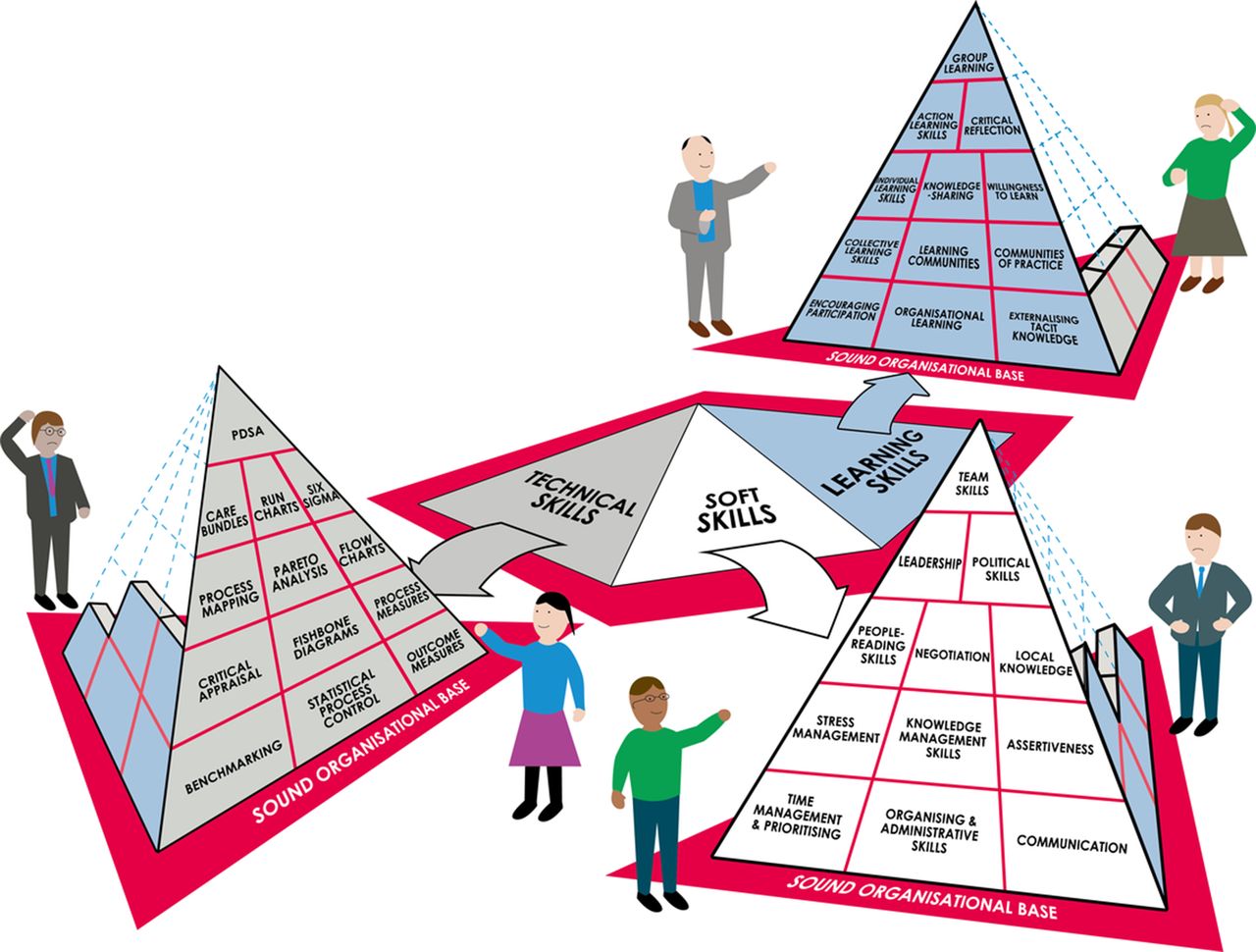
Our overall conclusion, therefore, was that none of the four groups could rely merely on acquiring and deploying technical QI skills; they could only make the intended improvements to the extent allowed by their ‘soft’ skills and collective-learning skills. Successful improvement work is like a three-sided pyramid (figure 1) built on an organisational base that has the strength, stability and characteristics to grow and support all of its sides—the technical, ‘soft’ and learning skill sets. Unless all three sides are appropriately balanced against each other, the pyramid’s height, and hence the degree of quality improvement, will be limited to the smallest side; or more likely—especially if its base is unsound—it will collapse.
{kind=link}
The improvement pyramid. Source: Claire Barry (Burning Bright Ltd) (reproduced from Gabbay et al 7), courtesy of The Health Foundation.
It was evident that the need for soft skills and learning skills varied according to the immediate cultural environments of the improvement groups, but our study was not designed to delineate the precise skills required by different team members at different stages of the work, which is now being explored in a further study. The key point is that each set of circumstances demanded from each group a distinct range of skills, some of which were deficient. Even in these highly successful healthcare organisations, the four groups faced diverse organisational challenges that would have overwhelmed their projects had the outside facilitators not actively helped them develop and apply the right balance of skills. But facilitators are rarely available to such teams; nor do they impart a long-term, rounded approach to the development of organisational improvement capability. A better approach might surely be to routinely anticipate the likely local organisational challenges to specific QI initiatives and to select and train the improvement teams so that all three sides of the pyramid are robust enough to ensure success.
Footnotes
Handling editor Mary Dixon-Woods
Contributors The project was initiated and led by JG and AlM. All four authors made substantial contributions to the design of the work and the acquisition, analysis and interpretation of data. JG drafted the paper, but all four had a hand in revising it critically for important intellectual content and gave final approval of the version submitted. All agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.