Article Text

Statistics from Altmetric.com
“A student of management and organisation theory could only be stunned by how little the efforts to improve quality [in health care] have learnt from current thinking in management and from the experience of other industries.” Christian Koeck BMJ 1998;317:1267–8.
Introduction
Health policy in much of the developed world is concerned with assessing and improving the quality of health care. The USA, in particular, has identified specific concerns over quality issues12 and a recent report from the Institute of Medicine pointed to the considerable toll of medical errors.3 In the UK a series of scandals has propelled quality issues to centre stage45 and made quality improvement a key policy area.6
But how are quality improvements to be wrought in such a complex system as health care? A recent issue of Quality in Health Care was devoted to considerations of organisational change in health care, calling it “the key to quality improvement”.7 In discussing how such change can be managed, the authors of one of the articles asserted that cultural change needs to be wrought alongside structural reorganisation and systems reform to bring about “a culture in which excellence can flourish”.8 A review of policy changes in the UK over the past two decades shows that these appeals for cultural change are not new but have appeared in various guises (box 1). However, talk of “culture” and “culture change” beg some difficult questions about the nature of the underlying substrate to which change programmes are applied. What is “organisational culture” anyway? It is to this issue that this paper is addressed.
Many previous policy reforms in the National Health Service (NHS) have invoked the notion of cultural change. In the early 1980s the reforms inspired by Sir Roy Griffiths led to the development of general management in hospitals and the greater involvement of clinicians in budgeting through resource management initiatives.9 Many of the themes of these reforms were extended by the market reforms of the early 1990s which separated out the functions of purchasers and providers.10 Central to these changes were attempts to increase management and accountability in the NHS, and to develop more of a “business culture”. Resistance and resilience to these changes was more evident than wholesale transformation.1138
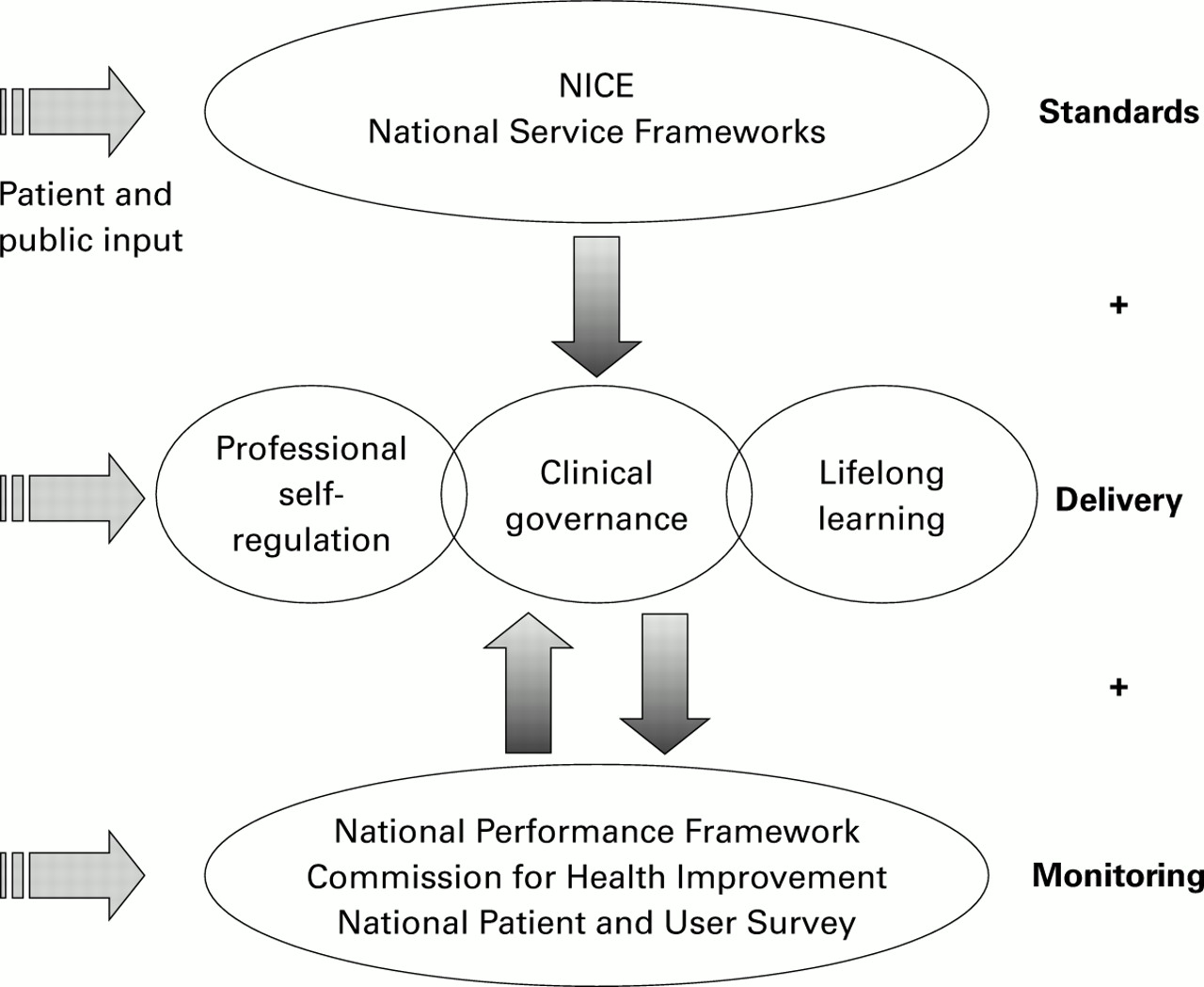
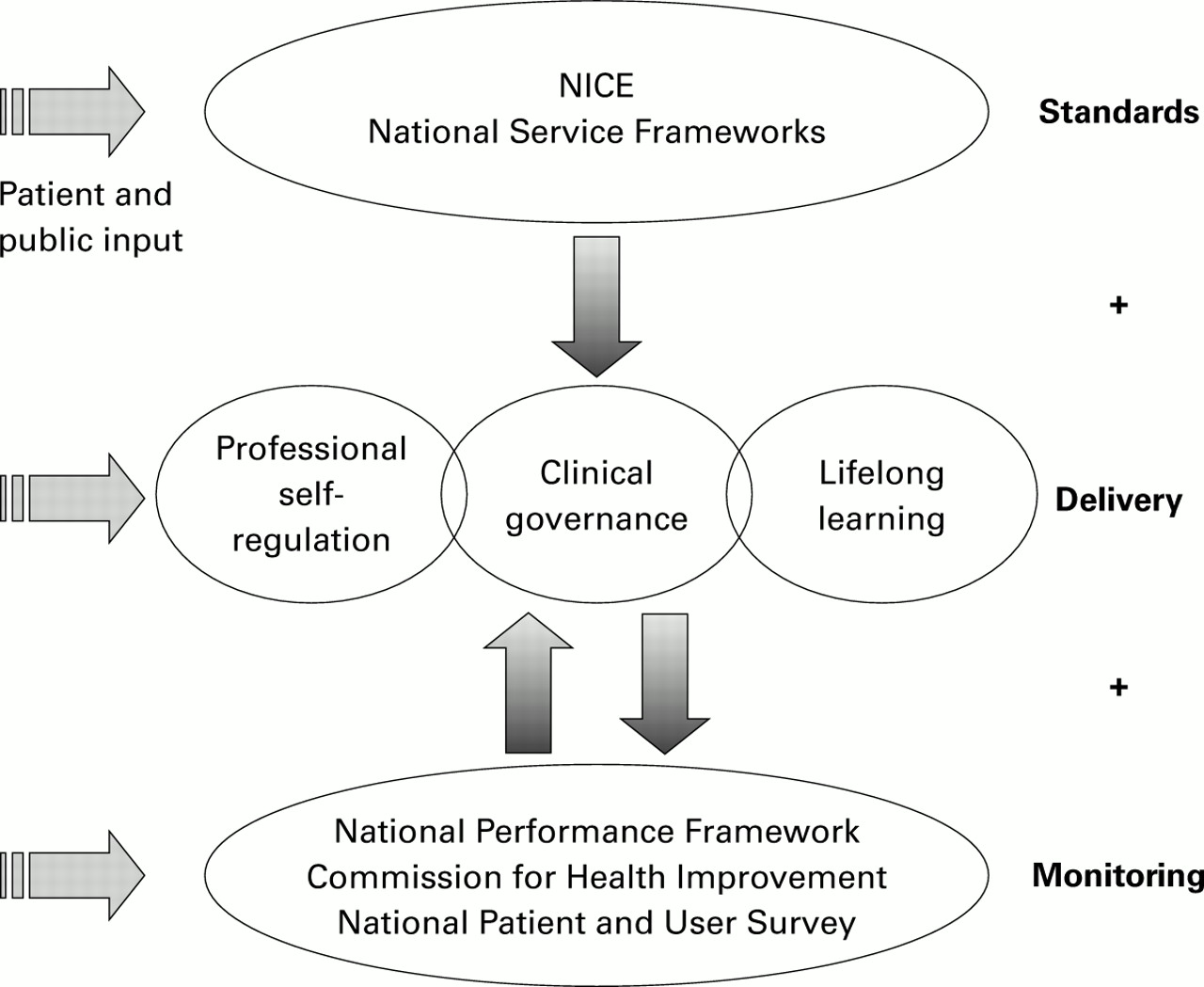
Since the election in 1997 the Labour Government has succeeded in making quality the central reform issue in the NHS. The new quality strategy as set out in the White Paper12 and supporting policy documents613 represents an ambitious attempt to develop an over-arching framework for health care quality. These documents articulate a detailed set of interlocking strategies, tactics, and supporting initiatives aimed at three factors:
defining appropriate quality standards;
delivering health care congruent with these standards;
monitoring to ensure that uniformly high quality of care is achieved (fig 1).
It is in the second of these, the delivery of health care, that a consideration of organisational culture has most to offer.
In articulating the strategy needed to reinvigorate health care delivery, official documents stress the interlinking of three different strands: clinical governance, lifelong learning, and professional self-regulation (fig 1). Underpinning and binding each of these is the notion of cultural transformation as a primary driver to delivering improved quality of care. “…achieving meaningful and sustainable quality improvements in the NHS requires a fundamental shift in culture, to focus effort where it is needed and to enable and empower those who work in the NHS to improve quality locally …” and “Clinical governance needs to be underpinned by a culture that values lifelong learning and recognises the key part it plays in improving quality” (paragraphs 5.6 and 3.28).6
Although often referred to, it is unclear whether talk of “cultural transformation” is merely a convenient metaphor or is, instead, shorthand for a more tangible raft of specific changes. If the latter, then it would seem essential to have some clear idea about the meaning of organisational culture, the extent to which this culture can be managed within health care, and the nature of the organisational cultures which underpin quality improvement activity in health care. This paper draws on a wide social science literature to open this debate. It explains some of the current conceptualisations of organisational culture and explores the implications of these for health systems (such as the NHS) or healthcare providers (such as hospitals and primary care networks) that are seeking organisational transformation.
Organisational culture
Notions of “culture” have deep roots in the anthropological literature going back many decades.14 The application of these ideas to organisations rather than indigenous peoples began in the United States in the immediate post war period1516 but came to popular attention in the 1980s. During this period a number of best selling management books proved influential in instilling the notion that “organisational culture” was a crucial variable in the management of organisational performance.17–19 Over the last decade interest in organisational culture has grown apace and it has received extensive study across many industry settings including some work on healthcare organisations.20–24
THE CONTESTED NATURE OF ORGANISATIONAL CULTURE
Although the notion of organisational culture is now frequently invoked in the organisations and management literature, it remains an elusive concept, fraught with competing interpretations and eluding a consensual definition (one review cites 15 different descriptions25). Despite such diverse views, two broad schools of thought can be distinguished.26 Firstly, there is the family of approaches that regard culture as something that an organisation is (here culture serves as a metaphor for describing an organisation rather than being seen as something readily identifiable or separable from the organisation itself). Indeed, post-modern perspectives on organisational culture dispute the very notion of organisations and their cultures as concrete entities (box 2). In contrast, there is the group of approaches that conceive of culture as something that an organisation has: aspects or variables of the organisation that can be isolated, described, and manipulated.
Post-modern perspectives are best understood in contrast with modernism. At the core of a modernist approach is a view that organisational phenomena (including cultures, structures, and performance) are concrete entities which can be systematically described and explained.27Such modernist accounts have proved immensely influential, not least because they offer managers and policy makers the seductive view that better understanding of this empirical reality will bring improved organisational control and performance. The latest NHS reforms conform to this modernist conception of organisational life, and much of our paper colludes with this view.
Over recent years, however, the modernist position on organisation studies has been subjected to a sustained critique from a range of loosely coupled approaches that have been termed post-modern.28 Although it is difficult to offer a precise definition of the term post-modernism (indeed the post-modern value of diversity precludes this), a number of broad themes can be identified:
Post-modernism sees the social world as constructed by our shared language, and asserts that we can only “know” this world through the particular form of discourse our language creates.
Organisations are not seen as concrete entities, to be revealed through the process of objective and scientific research, but are seen as being socially and discursively constructed. As reflections of a form of discourse—that is, linguistic artefacts—they are unstable and fragile.
The task of a post-modern analysis therefore is to deconstruct current processes of sense making29 to expose the unstable and superficial nature of social structures and practices, and to reveal the hidden contradictions, tensions, and “unreason” inherent in human experience.
One strand of post-modern analysis is concerned with how what is legitimised as knowledge is governed and constrained by vested interests. Different groups struggle and compete to impose their definitions. Knowledge is what the powerful say is knowledge, and those who define what knowledge is, are considered powerful. Therefore, post-modernism aims at understanding how groups engage in struggles to offer an authentic and legitimised view of the world.30 Post-modern perspectives thus encourage a diversity of voices and the celebration of difference.3132
A post-modern perspective on organisational culture would not focus on cultures as a means of control. It would instead encourage dialogue on the nature and course of change among stakeholders, particularly those who traditionally have been disenfranchised or marginalised from such discussions. The emphasis of such a dialogue would be on challenging existing authorised accounts and balances of power, rather than on the refinement of mechanisms of control.
This distinction is crucial for, if culture is something that an organisation has, then it may be possible to create, change, and manage culture in the pursuit of wider organisational objectives. However, if organisations simply are cultural entities, then their study may help us to understand the processes of social construction at work but offers less in terms of shaping change or assisting with management control. It is clear that much of the prescriptive advice aimed at organisations from the management literature assumes that cultures are an attribute of organisations that are open to manipulation. Indeed, the current NHS reforms in the UK also embody this view (see box 1). Given the critiques of such an approach in the literature, we would not like to go too far down this road: our working assumption in this paper is that an organisation's culture is an emergent property of that organisation's constituent parts—that is, the culture may emerge somewhat unpredictably from the organisation's constituents (making it not necessarily controllable), but nonetheless characteristics of that culture may be described and assessed in terms of their functionality vis à vis the organisation's goals.
CULTURAL ATTRIBUTES AS ORGANISATIONAL VARIABLES
There is substantial agreement among those who conceive of culture as an organisational variable: organisational culture emerges from that which is shared between colleagues in an organisation, including shared beliefs, attitudes, values, and norms of behaviour. Thus, organisational culture is reflected by a common way of making sense of the organisation that allows people to see situations and events in similar and distinctive ways.263334 It is “the way things are done around here”, as well the way things are understood, judged, and valued.
In attempting to untangle the various elements of organisational culture, several levels can be identified.3536 At the most basic level are the underlying assumptions that represent the unconscious and “taken for granted” beliefs that structure the thinking and behaviour of an individual. These assumptions then give rise to organisational values that operate at a more conscious level and represent the standards and goals to which individuals attribute intrinsic worth.37 Then, more visible still are those artefacts that represent the concrete manifestations of culture. These might include, for example, the ceremonies, traditions and the incentive structures peculiar to an organisation. Some examples in health care of these different cultural levels are given in box 3.
Examples of different levels of culture within the NHS
Assumptions are the basic “taken for granted” views of the world and how one can understand and intervene in it—that is, ontology and epistemology. For example, medical research has traditionally been predicated on the use of rational scientific methods as the basis of generating and accumulating knowledge (controlled trials rather than qualitative and interpretative methods). Thus, assumptions about measurability, aggregation, and transferability of knowledge are deeply ingrained in medical care.
Values constitute the basic foundations for making judgements and distinguishing “right” from “wrong” behaviour. In the medical profession conduct has traditionally been based on the Hippocratic principle of placing the needs of individual patients above broader economic and corporate objectives; this, in turn, has led to clinical freedom being a highly prized cultural “value”.
Artefacts include the physical and behavioural manifestations of culture. In the medical profession these may include such diverse issues as dress codes (the doctors' ubiquitous white coat and tie), standard ways of running services (the physician's beds, the surgeon's list, juniors attached to seniors), or methods of performance assessment (the dominance of confidential peer review, the reliance on professional self-regulation).
In terms of health care, such differentiation of cultural levels is both important and helpful. Whereas the more visible artefactual elements of culture may be readily manipulated, deep-seated beliefs and values may prove more resistant to external influence. Indeed, there is some evidence from the NHS to suggest that previous attempts at cultural transformation may have succeeded only at a superficial level. For example, the Griffiths' reforms of the 1980s tried to overlay an overt management culture onto an organisation with an otherwise extant public service orientation.9 These reforms succeeded in changing some of the surface manifestations of medical culture—for example, the development of budgets and contracts—but they were less successful in penetrating the deeply entrenched values and beliefs (and power bases) that underpin clinical practice. Thus, clinician autonomy remained largely unchanged.38 Similarly, there is evidence to suggest that the internal market reforms, despite their apparent revolutionary nature, had little impact on the culture of the medical professions, at least initially.11
Given the contested nature of organisational culture, it should not be surprising that no consensus exists as to the range and definition of the organisational variables that fall within its purview. Nonetheless, some of the aspects of organisational culture on which there is at least some measure of agreement are described in box 4. It is not hard to see that these aspects are central to much of the debate about the future directions of health services, public or private.
Attitudes to innovation and risk taking: whether the organisation encourages and rewards new ways of doing things, or instead values and maintains traditional approaches.
Degree of central direction: the extent to which objectives and performance expectations are set centrally rather than being devolved.
Patterns of communication: the degree to which communication, instruction and reporting are restricted to formal hierarchies of authority (compared with informal channels).
Outcome or process orientation: the extent to which control and reward mechanisms are focused on tasks compared with the end product/service.
Internal or external focus: the extent to which attention is directed at external stakeholders, especially customers and the wider community, compared with an emphasis on internal organisational issues.
Uniformity or diversity: the attitudes and expectations within the organisation that either value consistency or encourage diversity.
People orientation: this dimension encapsulates the attitudes towards, support for, and valuations of, the organisation's human resources.
Team orientation: does the organisation encourage and reward individualism, or are internal structures designed to foster and value close teamwork?
Aggressiveness/competitiveness: this dimension captures the prominent attitudes in the organisation towards other external players in the same arena. To what extent are organisational attitudes focused on dominating rather than coexisting, cooperating, or even learning from other similar organisations?
Attitudes to change: to what extent is the organisation focused on internal stability rather than dynamic concerns (such as increasing size, scope or competitiveness)?
CULTURAL DIVERSITY
The culture found within an organisation may be far from uniform or coherent.2641 Indeed, looking for commonality may be less rewarding than an examination of differences (see box 5). Although some cultural attributes may be seen across an organisation, others may be prominent only in some sections of that organisation. Thus different cultures may emerge, for example, within different occupational or professional groups. These groups may even seek to differentiate themselves from one another by their cultural artefacts or values. Such subcultures may be associated with different levels of power and influence within the organisation, whose dynamics may alter over time—witness, for example, the dominance of the medical culture in the NHS and the relatively recent rise of the management culture.22384243
Integrated: Integrated cultures occur when there is wide consensus on the basic beliefs and appropriateness of behaviours within the organisation. Although often assumed, such integration may exist only in broad aggregate or may be more wishful thinking than practically realised.
Differentiated: Differentiated cultures occur when multiple groups within an organisation possess diverse and often incompatible views and norms. The development of subcultures, misunderstandings, and conflicts is then to be expected. The NHS has long existed as a collection of loosely coupled differentiated cultures (medical, nursing, professions allied to medicine, administrative and, more recently, managerial groups).
Fragmented: At the most extreme, differentiated cultures may diverge and fragment to such an extent that cross-organisational consensus and norms are absent. Even within specific groups, differences may be more marked than commonality, and agreements that are seen may be only fleeting and tied to specific issues. Thus, the organisation is characterised by shifting alliances and allegiances, considerable uncertainty and ambiguity, and unpredictability.
This typology is not intended to suggest that organisations have cultures that are either integrated, differentiated, or fragmented. Instead, each of these views may be applied to the same organisation to reveal, rather than hide, an overall lack of coherence.
Rivalry and competition between groups may appear as a key feature of the overall organisational culture (health care is notoriously tribal in this respect).2043 Different subcultures may be more or less malleable (susceptible to managed change of their artefacts, values, or beliefs) or may even be avowedly resistant to change (perhaps developing the status of “counter cultures”). Indeed, it is apparent that some organisations function more or less successfully with discordant subcultures, with each subculture being no more than “loosely coupled” to other subcultures or subsystems.2043 Nonetheless, different subgroups may still share certain key cultural attributes while conflicting on others; for example, while doctors and managers may differ culturally they both “inhabit a shared culture of medical autonomy”.44 It remains an open question as to whether it is even desirable that an organisation should seek an integrated set of cultural attributes.
Finally, organisations receive many cultural influences from outside the organisation and these influences may be at odds with the internal culture. Thus, the medical culture within a hospital will be influenced not just by aspects of that organisation but also, most prominently, by the current prevailing culture of the medical profession (nationally and even internationally), as well as by greater secular trends. Dealing with dissonance between the organisational culture and the prevailing professional culture will be difficult.
CULTURE AND PERFORMANCE
For all the interest in defining and assessing organisational cultures, the crucial generic question of whether and how organisational culture impacts on organisational success or performance remains empirically poorly explored. A simple causal relationship between cultural characteristics and success has not yet been demonstrated—unsurprisingly, any relationship is highly contingent on definitions of success and a wide range of other internal and external factors.4546 Such evidence as exists is equivocal at best.4748 Nonetheless, organisational culture appears to be a crucial factor in understanding the ability of any organisation to perform and compete,1718 and some work in health care confirms this.2324 Indeed, many organisations—public and private—place great store by shaping their cultures as a means of improving organisational fitness.19 It is clear from policy documents that the current UK government also takes the activist view that managing the culture is one route towards improving health care:
“We are looking at major cultural change for everyone. There is a need to develop organisations to support a change in culture and to deliver change” (paragraph 5.21).6
Cultural formation and transformation
Although certain cultural traits may endure within an organisation, culture is more dynamic and shifting than static. It is dynamic in that there may be rapid swings in organisational norms—for example, in response to organisational crises—and shifting in that longer term and more consistent drifts may occur—for example, the gradual acceptance of the management culture in the NHS. Newcomers to an organisation may bring with them prior expectations about the culture when they join, but culture is also transmitted to new arrivals by established staff, sometimes explicitly but more often implicitly. The organisational culture is shaped and articulated not just by individuals but also by new and old organisational features. The organisational structures, routines, command and control expectations, and operational norms all have influence.26 Large gaps may develop between overt statements about cultural variables (such as the values outlined in hospital mission statements) and the implicit communication of the same—for example, in the ways in which services are managed and delivered.
Organisational culture can also be influenced by factors outside of the organisation.26 The strong professional ethic and sense of professional identity seen in the health professions attest to the importance of supra-organisational norms. Public opinion, media reporting, and regulatory frameworks also exert influence.4 All these observations have implications for those attempting to manage a cultural shift.
MANAGING CULTURE
Given that an attempt is to be made at a cultural transformation within healthcare providers (as it surely is within the NHS with the advent of clinical governance849), what are the issues that need to be considered? Firstly, wholesale and simultaneous change on all the many different aspects of organisational culture is unfeasible and probably not even desirable. For example, several valuable cultural traits already exist in the NHS on which any new quality strategy can build, most notably a commitment to equity and belief in the founding principles—that is, a universal comprehensive service available to all without regard to ability to pay. More recent helpful values that are beginning to emerge include, for example, the centrality of patient care, a belief in evidence, and a growing willingness to examine quality issues, although these values may be conceptualised rather differently by different professional groups. Thus, any strategy for cultural change should be selective, aiming for a balance between continuity and renewal, identifying those cultural aspects to keep and reinforce, and those which need to be reworked.
Secondly, the nature of the cultural destination for the NHS and other healthcare organisations is currently far from clearly specified. Shortell et al50 identified what they termed “characteristics of the new moral fabric” which may help to define some of the future directions (box 6). In addition, a close reading of official policy documents and accompanying commentaries allows elucidation of other possible aspects of the desired cultural change (see box 7). However, what these shifts mean for day to day practice has yet to be properly analysed, assessed, and communicated. Much work remains to be done on defining a vision for a “transformed NHS” in terms of its cultural assumptions, values, and artefacts.
Characteristics of the old and new “moral fabric” for physicians. Adapted from Shortell et al.50
Changing cultural visions in the NHS.
Thirdly, cultural change cannot easily be wrought from the top down by simple exhortation. Successful strategies need to take into account the needs, fears, and motivations of staff at all levels.51 Furthermore, any attempt to influence key cultural dimensions (such as those described in box 4) needs to be part of a much wider assemblage of mutually reinforcing improvement activities.34 The organisational culture cannot be tackled in isolation from such issues as the organisational structure, financial arrangements, lines of control and accountability, strategy formulation, or human resource management initiatives. In particular, in the UK the much vaunted “clinical governance project” is central to cultural transformation. So this and supporting initiatives (in particular, the National Institute for Clinical Excellence, the Commission for Health Improvement, National Service Frameworks, and the National Performance Framework) need to be integrated with a clear and consistent set of cultural values.852 For example, application of the substantial set of measures outlined in the National Performance Framework and the growing public release of clinical performance data may inhibit the inculcation of welcome cultural traits such as innovation and openness.53
Finally, coherence within the organisation is necessary but may not be sufficient to bring about substantial change. The influence of outside professional bodies (such as the Royal Colleges in the UK), specialist societies, patient interest groups, and the media may cut across and sometimes work against efforts at internal reform. Identifying areas of consensus and consistency in the values espoused by these organisations and attempting limited cultural shifts in these areas may therefore be advantageous.
MANAGING CULTURAL DIVERSITY
One crucial relationship in making a reality of cultural transformation within clinical governance is that between health service managers and the medical profession. Yet these two groups are rooted in very different professional cultures (box 8). Thus, one challenge is to devise strategies on cultural transformation that successfully achieve a degree of “cultural fit” between these two key groups. Some general lessons for health care may be drawn from the literature on strategic alliances where various models have been developed to understand how “cultural fit” arises between strategic partners.
Managerial and medical cultures: points of divergence.
Child and Faulkner37 developed a useful typology to classify the various approaches to managing cultural diversity. In essence, two fundamental policy choices in the management of cultural diversity were identified. The first is whether one partner's culture should dominate, as opposed to striving for a balance of contributions from the contributory cultures. The second choice addresses whether to attempt an integration of the partners' cultures (with the aim of deriving synergy from them) versus a preference for segregating the cultures within the organisation (with the aim of avoiding possible conflict and reducing the effort devoted towards cultural management). These policy choices give rise to four possible bases for accommodating cultural diversity: synergy, domination, segregation, or breakdown (see box 9). The first three offer a basis for establishing cultural fit, whilst the fourth results in inaction or organisational damage. At different times each of these outcomes has been seen in UK health care (box 9), although whether these were as the result of deliberate policy choices is doubtful. More considered attempts at cultural transformation will need to address explicitly the importance of managing cultural diversity in order to achieve cultural fit.
Synergy represents a policy of cultural integration on the basis of melding both partners' cultures and aims to achieve the best possible fit between the two. In this approach the best elements of each culture are combined with the aim of making the whole greater than the sum of its parts—for example, the combination of management and clinical roles by clinical directors in the NHS.
Domination recognises that melding may prove impossible and accepts the right of dominance of a given group's culture—for example, clinicians have largely assumed this within the NHS.
Segregation is based on seeking an acceptable balance between cultures by virtue of maintaining separation rather than seeking integration. Many interprofessional alliances within the NHS may be seen to be of this type—for example, accommodation between the nursing profession and doctors.
Breakdown occurs when one partner seeks domination, integration, or mutually acceptable segregation but fails to secure the acquiescence of the other parties—for example, the Griffiths' reforms initially largely failed to usurp the dominance of the medical profession.
Concluding remarks
Recent commentators have asserted that improving the quality of health care will involve wholesale systemic change, not just tinkering around the edges.754 In the UK the Government's quality strategy seems to recognise just this, emphasising the importance of cultural transformation, and in the USA the Institute of Medicine's ongoing investigations reveal a preoccupation with system change. However, if such an approach is to bear fruit, a number of assumptions that are currently implicit in the approach must be verified as having some substance. Firstly, there must be such a thing as “organisational culture”; secondly, the nature of this culture must have some bearing on clinical performance and health care quality; thirdly, it should be possible to identify particular cultural attributes that are facilitative of performance (or at least, we should be able to pinpoint those that are damaging); and, finally, there must be some hope that interventions and management strategies can have a predictable impact on cultural attributes as a precursor to bringing about performance improvements. At the very least, this paper demonstrates that these assumptions are far from trivial or self-evident. Indeed, empirical data are largely absent and conceptual thinking illuminates contention rather than consensus. This, in turn, suggests that a more sober assessment of the task of cultural transformation in health care is warranted.
While some argue that culture cannot be shaped as such but that patterns simply emerge over time, others believe that culture can indeed be adapted by conscious effort to beneficial effect.455556 Taking this view—as the UK government clearly does—a number of important issues emerge from the preceding discussions:
there is a rich literature from other industries (and, indeed, some from health care) with much to teach organisations seeking transformation. It would be a mistake to neglect this resource, but empirical work within the distinctive cultures of the healthcare industry is urgently needed to particularise the findings to local circumstances;
the scale and scope of the task facing healthcare providers is substantial. The changes required are not just structural and procedural but more fundamentally encompass attitudinal change and the installation of new values. The task is one of engaging hearts and minds which will require actions and words linked with an unusual level of coherence and consistency;
wholesale change of organisational cultures will be problematic and probably inappropriate. This begs the questions of what should be retained and how specific cultural attributes can be selected and targeted;
managing the cultural diversity exhibited in health care to achieve fit and synergy between diverse groups will be a challenge. The recognition that much of the conflict centres around issues of power and legitimacy may be an important precursor to achieving that fit;
conspicuously, we have not sought to identify which cultural attributes most contribute to high quality, effective, and efficient health care, nor have we attempted to articulate the strategies that may be helpful in bringing these about. Although some guidance here is available,5758 these tasks remain substantial;
attempts to enact a cultural transformation within health care can expect to meet with resistance (passive or active), both from reluctant organisations and resistant organisational subgroups;
any strategy to change the culture within health care will need to heed the constraints imposed by external influences on cultural values, especially those arising from the various healthcare professions. Thus, national quality strategies will also need to influence more than just the activities of healthcare delivery organisations59;
attempts at cultural transformation may induce deleterious and unwelcome changes as well as the sought for cultural shifts.6061 Avoiding these dysfunctional consequences (or even assessing whether they have been induced) may be difficult.
A certain amount of cultural fluidity in organisations is to be expected, and this may be exacerbated when organisations struggle to cope with a turbulent environment. Nonetheless, recognising that cultures do change need not imply that cultures can be changed in a predictable manner by policy or managerial interventions. Indeed, observation in other industries suggests that one of two circumstances must pertain if fundamental change is to be achieved: either the organisation must be facing imminent crises leading to possible extinction6263 or there must be considerable organisational slack available.6465 Whereas the upheavals wrought by managed care in the USA may provide such conditions, it seems doubtful that either of these circumstances currently prevails in the UK.
This paper has attempted to sharpen thinking on the nature of organisational cultures in health care as a means of underpinning debates on whether and how such cultures should or, indeed, can be transformed. It is our view that strategies aimed at revolutionising the quality of health services through cultural transformation need to be more articulate on the cultural destinations sought, and the mechanisms that will carry organisations towards these destinations.
{kind=link}
The UK health care quality strategy. 6
The Commonwealth Fund
Harkness Fellowships in Health Care Policy
The Commonwealth Fund of New York is pleased to announce the Harkness Fellowships in Health Care Policy and to invite applicants for the 2001–2002 fellowship cycle.
The Harkness Fellowships in Health Care Policy provide a unique opportunity for promising health policy researchers and practitioners (e.g. physicians, health services managers and government officials) who are early in their career to spend 4–12 months in the United States conducting a policy-oriented research project and working with leading US health policy experts.
Fellows must demonstrate a strong interest in health policy issues and propose a well designed research study that falls within the scope of the Fund's national program areas:
improving health care services
bettering the health of minorities
advancing the well being of elderly people
developing the capacities of children and young people
Studies that include comparisons between the United States and the applicant's home country are encouraged. The Fund will provide extensive support to successful fellows to help them develop and shape their research proposals to fit the US context. Through its extensive network of contacts, the Fund will help identify and place fellows with a mentor who is an expert in the policy area to be studied. Fellows will also be required to identify a home country mentor who will act as a liaison with the US mentor and supervise any cross-national comparisons that are to be conducted as part of the study.
The deadline for receipt of applications is 2 October 2000. In order to apply, applicants must be citizens of the United Kingdom, Australia, or New Zealand and submit a formal application. Up to 10 Harkness Fellows in Health Care Policy will be selected annually.
Each fellowship will provide up to $75 000 (US) in support, which includes round trip airfare to the United States, a monthly stipend, support towards any portion of the study conducted in the home country, project-related travel and other research expenses, tuition for related academic courses, and health insurance. In addition, a family supplement is available to fellows accompanied by a spouse and/or children.
To obtain a brochure and application materials, please contact Robin Osborn, Director, International Program in Health Policy, The Commonwealth Fund, One East 75th Street, New York, NY 10021, United States (telephone 212/606-3809, fax 212/606-3875, email ro{at}cmwf.org) or see The Commonwealth Fund's world wide web home page (http://www.cmwf.org).
Acknowledgments
Huw Davies was on sabbatical in the United States as a Harkness Fellow in Health Care Policy during the preparation of this paper. Funding for the Fellowship was provided by The Commonwealth Fund, a New York City based private independent foundation. Russell Mannion was funded under a research programme supported by the Department of Health. However, the views presented here are those of the authors and not necessarily those of either of the funding bodies, or their directors, officers or staff.
Conflicts of interest: None.