Article Text

Statistics from Altmetric.com
As the human lifespan increases and healthcare quality improves, more people are reaching an advanced age only to present with cardiac disorders that are usually treated uneventfully in young patients. The balance between enhanced initial risks and reduced eventual benefits in the elderly has often led to difficult medical decisions, and at times painful ethical and economical considerations.
Although there may be, on an individual basis, a substantial discrepancy between chronological and physiological age, the ability of elderly patients to withstand a major physiological insult such as cardiac surgery is reduced because of associated comorbidities, limited functional reserve of vital organs, and diminished defence and adaptation capacities. In the 1970s, an increase in mortality after cardiac surgery was apparent in patients older than 70 years. With the development of less traumatic heart–lung machines, more effective myocardial protection strategies, and improved perioperative care, mortality in the more robust patients—that is, the septuagenarians—dropped to levels of younger age groups.1Nowadays, the range of benefit of cardiac surgery remains narrow in patients 80 years of age or older, the age group discussed here.
Epidemiology
In the early 1990s, 7.4 million people (3% of the population) in the USA were older than 80 years. With a current life expectancy of 6.9 years for octogenarian men and 8.7 years for women, the number of octogenarians is expected to exceed 10 million (4.3 % of the population) by the year 2000. In England, the number will be 2 million. It is estimated that 40% of octogenarians have serious symptomatic heart disease. The number of elderly patients undergoing open heart surgery is increasing in all institutions. Because women outlive men by 6.9 years the ratio of women to men undergoing surgery increases and comes close to 1:1 in the older groups.
Principles of cardiac surgery in octogenarians
Consider only symptomatic patients
Liberal indications for independent and motivated patients
Select the simplest operation and accept incomplete repair
General considerations
Frailty of the elderly
Elderly patients with valve disease present with associated comorbidities (table 1) as well as reduced defence and adaptation capabilities. The aging process and atherosclerosis have undermined the reserve of many organs that are bound for postoperative dysfunction, or have already induced altered function. Furthermore, atherosclerosis frequently involves the aorta. Any manipulation of the aorta (cannulation for arterial inflow during cardiopulmonary bypass, cross clamping, and placement of a de-airing vent) may fragment a plaque and induce embolisation. Intraoperative transoesophageal and/or epiaortic echocardiography, which should routinely complement palpation of the aorta in the elderly, has shown that 20% of patients older than 75 years have protruding, sometimes mobile, atheromatous plaques in the ascending aorta and aortic arch.2 The risk of embolisation can be reduced by avoiding cross clamping of the aorta and performing the operation (sometimes with endarterectomy or resection of the ascending aorta and aortic arch) during a period of deep hypothermic circulatory arrest. This formidable undertaking is, however, inappropriate in an old patient, and gentle manipulation of the aorta remains the sole practical preventive measure.
Prevalence of comorbidities in octogenarians with cardiac valve disease
Malperfusion of the brain is another complication of diffuse atherosclerosis that may occur during cardiopulmonary bypass. The lack of pulsatility of the bypass flow, uneven distribution of blood because of atherosclerosis, and impaired cerebral autoregulation may result in global or local underperfusion of the brain. Delayed awakening, agitation, and incomplete return of cognitive function are possible consequences of poor global brain perfusion. Together, diffuse and focal neurological deficits may affect 15–20% of elderly patients after heart surgery and are particularly devastating; they initiate a protracted postoperative course which often turns out to be fatal or leads to permanent institutionalisation.
Surgical risk:benefit ratio in the elderly
The true influence of age on early mortality after cardiac surgery is difficult to estimate, because of the high prevalence of other confounding factors. Although age appears in all scoring systems as an incremental risk factor for postoperative mortality, some studies found that it had no or only a marginal influence in relatively simple operations like isolated aortic valve replacement.3 Most scoring systems in open heart surgery have shown that mortality increases logarithmically with the progression of the risk score. Figure 1, which is derived from the French score,1represents the mortality of mitral and aortic valve surgery in relation to the risk score. Age over 80 years shifts the patient to the right, where the steep rise in mortality starts. Without the addition of another risk factor, the operative risk of an octogenarian seems acceptable for almost any cardiac operation. The addition of one single moderate risk factor (with a score of 2 in fig 1) doubles the mortality rate of the cardiac operation. The addition of two moderate or one serious risk factor (with a score of 5) more than triples the rate and should warn against surgery.
Mortality rates of aortic and mitral valve surgery according to the cumulated risk score. Critical situations include urgent operations (acute aortic dissection, postinfarction ventricular septal defect or papillary muscle avulsion) and necessity to operate within 48 hours after myocardial infarction. AVR, aortic valve replacement; MVR, mitral valve replacement; CABG, coronary artery bypass graft; LV, left ventricular.
The expected benefit of an intervention should not be viewed in terms of prolonging life, but of improving the quality of life; octogenarians seek surgery only to preserve their fading activity, threatened independence, or both. Therefore, only symptomatic and motivated patients should be considered for surgery, and the increase in wellbeing must be substantial to justify the operative risk. Obviously, conditions such as dementia or protracted depression that prevent an improvement in quality of life, and disorders such as advanced cancer or organ failure that reduce length of survival, make even low risk cardiac surgery inappropriate. Likewise, prophylactic operations or operations that yield a benefit only after a long survival, such as the “Maze” operation for chronic atrial fibrillation or the Ross procedure for aortic valve disease, should never be considered in the elderly. Not only does the addition of any comorbidity lead to a steep increase in the operative risk, it also reduces survival prospects in the elderly. In such a situation, the surgeon is well advised to opt for a technically and physiologically less demanding operation, even at the cost of an incomplete repair, with reduced mid-term benefit. Acceptance of a residual aortic stenosis in case of a small aortic annulus, mild mitral regurgitation (with or without repair) or revascularisation limited to the major coronary arteries are examples of incomplete yet appropriate management in the sick elderly. A fair and objective discussion regarding operative risk and subsequent improvement in quality of life will allow most elderly patients, their family and doctor to reach a decision regarding further treatment. The decision will, however, be difficult to reach in the case of acute cardiac failure, because the patient may no longer be able to assess critically his or her needs and wishes.
Comorbidities advising against valve surgery
Coronary artery disease and left ventricular ejection fraction < 30%
Creatinine concentration > 200 μmol/l
Chronic obstructive pulmonary disease with FEV1 < 800 ml
Neurological deficit restricting patient's independence, outside activity, or both
Debilitating psychiatric disorders (dementia, protracted depression)
Cancer reducing quality of life, survival, or both
FEV1, forced expiratory volume in 1 second
Preoperative investigations
A decision regarding the necessity for valve repair or replacement can be based on clinical and echocardiographic findings alone. Atherosclerosis is, however, so conspicuous in the elderly that coronary angiography is appropriate in almost every patient. The risk of this examination, although increased, is not overwhelming (procedural mortality and morbidity are around 0.5% and 5%, respectively) and the benefit of appropriate coronary revascularisation is undisputable. Likewise, to reduce the high rate of postoperative stroke, a Doppler ultrasound of the carotid artery bifurcation should be obtained in every patient. Carotid endarterectomy before or at the time of heart surgery should be considered for symptomatic or bilateral high grade stenosis. The presence of an asymptomatic carotid stenosis or occlusion should lead the surgeon to work with higher perfusion pressures, some will add some degree of systemic hypothermia, during the period of cardiopulmonary bypass.
Appropriateness of valve operations in octogenarians
Aortic valve replacement for severe stenosis +++
Mitral valve repair or replacement for severe insufficiency ++
Aortic valve replacement for moderate stenosis during CABG ++
Mitral valve repair for moderate insufficiency during CABG +
Percutaneous balloon valvoplasty of the mitral valve +
Mitral valve replacement for moderate insufficiency during CABG 0
Combined aortic and mitral valve replacement 0
Percutaneous balloon valvoplasty of the aortic valve 0
Composite graft or homograft replacement of the aortic root −
Ross procedure (pulmonary autograft) −− +++ highly recommended; ++ recommended; + acceptable; 0 not recommended; − should be avoided; −− has no indication.
Aortic valve disease
Aortic valve stenosis
Indication for surgery
Calcific aortic stenosis is the most common valve disorder encountered in octogenarians, and accounts for 60–70% of the valve surgery caseload.4 ,5 In a population based study, significant aortic stenosis was found in 2.9% of randomly selected people aged 75–86 years, half of whom had symptoms. This figure predicts a yearly potential need for 3500 aortic valve replacements in octogenarians in a country like England.
Replacement of a stenotic aortic valve (and myocardial revascularisation limited to major coronary trunks) in elderly patients should be considered when symptoms occur. Most surgeons, however, will also consider valve replacement for only moderate stenosis (with a transvalvar gradient between 20–30 mm Hg and a valve orifice surface between 1–1.2 cm2) in patients undergoing coronary revascularisation. This prophylactic replacement seems warranted on the grounds that the replacement only marginally increases the operative risk and progression of an aortic stenosis in an elderly person can be rapid, quickly negating the benefit of isolated bypass surgery.
Choice of prosthesis
Because the life expectancy of an octogenarian is shorter than the expected functional time of a biological prosthesis, most surgeons select a tissue valve for aortic valve replacement. Even if the thromboembolic risk of a mechanical valve in the aortic position can be controlled with a low anticoagulation dosage, the risk of bleeding remains a concern in the elderly patient. A few surgeons argue that the risk is extremely low and warrants implantation of mechanical prostheses in small aortic annuli. These prostheses have a smaller transvalvar gradient than bioprostheses and provide better haemodynamics and unloading of the left ventricle in annuli smaller than 21 mm in diameter.6 In this situation, however, most surgeons accept the higher residual gradient of a bioprosthesis, or choose to enlarge the aortic annulus with a patch to accommodate a larger biological valve, or implant a stentless biological valve. The stentless valves are devoid of a sewing ring and, therefore, offer the largest opening surface and smallest transvalvar gradient. They are, however, more difficult to implant (they require two separate suture lines) and require longer cross clamp and cardiopulmonary bypass times. Furthermore, the suturing of the commissures of the prosthetic valve may be dangerous on a calcified aortic root, as is often encountered in old patients.
Results of surgery
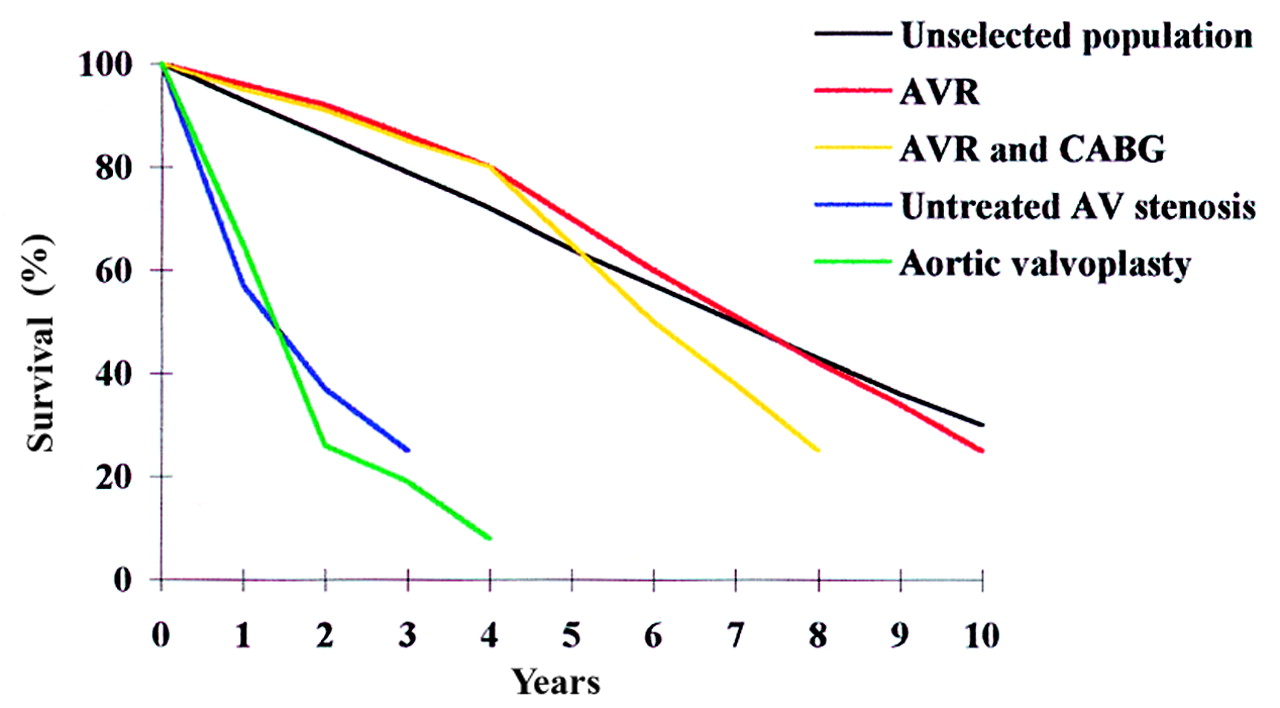
The majority of patients with aortic stenosis have a preserved left ventricular function and half have normal coronary arteries. Postoperative mortality rates of 5–10% (only slightly higher than the rates of 2–3% for younger populations) are regularly reported for isolated valve replacement in this age group.3-5 ,7Associated coronary artery disease requiring coronary grafting raises the mortality rate to 15–20%. Although these good operative results were achieved on a selected population of fit elderly patients, it must also be acknowledged that the great majority were operated on at an advanced stage of valve disease, and a significant proportion had congestive heart failure, a condition known to increase operative mortality.4 ,5 After successful surgery, survival is similar to a control population with rates of 95%, 80%, and 70% at one, three, and five years, respectively (fig 2).7 The great majority of patients (up to 90%) return to their homes and lead an independent life, and those not limited by other comorbidities are able to perform moderate to vigorous activity.8 These excellent results contrast with the grim natural history of symptomatic aortic stenosis. The survival rate of a matched population of patients who refused surgery (not of patients to whom surgery was not offered) was 57%, 37%, and 25% at one, two, and three years, respectively, and their quality of life was severely reduced.9
{kind=link}
Survival rates of octogenarians with aortic valve stenosis. AV, aortic valve; R, replacement; CABG: coronary artery bypass graft.
Percutaneous balloon angioplasty
Percutaneous balloon angioplasty has been proposed to relieve aortic stenosis in the elderly patient. Yet stenotic aortic valves in octogenarians exhibit rock hard calcification of the leaflets with no discernible commissures, and are the least suitable valves for dilatation. The results of balloon dilatation in this age group are disappointing with a significant rate of serious complications, including death, stroke, aortic rupture, and aortic insufficiency, and a high prevalence of residual or early recurrent severe stenosis.10 Persistence of stenosis accounts for the lack of improvement in survival rates. That the results of valve replacement after failed percutaneous valvoplasty are also good (according to the US registry, the operative and two year survival rates after failed valvoplasty were 88% and 71%, respectively11) suggest that the reluctance to operate on aortic stenosis in the elderly is often exaggerated and the counselling for treatment options too often slanted towards valvoplasty. Valvoplasty might be considered as an initial step to alleviate stenosis in patients presenting with acute decompensation and progressive renal, hepatic, and respiratory failure. Although it is unclear whether this bridging valvoplasty is more effective than urgent surgery, it has the advantage of postponing major surgery until the patient can give a considered decision about his or her destiny.
Aortic valve regurgitation
Aortic valve insufficiency is rare in this age group and represents only 3–5% of the valve surgery caseload.5Chronic forms are found in patients with longstanding hypertension, in patients with progressive dilatation of the ascending aorta, and in patients who previously received an aortic bioprosthesis that has degenerated. Medical treatment, centred on the administration of vasodilators, often succeeds in stabilising or slowing progression of regurgitation. While surgery is advised prophylactically in young patients for echocardiographic signs of early ventricular deterioration or for when the diameter of the ascending aorta exceeds 6 cm, it should be deferred in octogenarians to when symptoms occur. In case of dilatation of the ascending aorta, a reduction plasty of the aorta reinforced with a synthetic mesh combined with the aortic valve replacement is a valuable alternative to the more radical but also more dangerous composite graft replacement. Acute forms of aortic valve insufficiency occur with endocarditis and aortic dissection. Emergency replacement of the aortic root with a valve homograft (with reimplantation of the coronary arteries) is the procedure of choice in endocarditis not responding to medical treatment in young persons. The magnitude of the operation, however, is excessive for the ill prepared and septic elderly. Debridement of the annulus and replacement of the valve with a prosthesis can be a better alternative, even if the risk of persistent or recurrent endocarditis is higher. Aortic insufficiency in aortic dissection is caused by the loss of commissural support of the valve and can usually be corrected by appropriate resuspension of the commissures. Resection of the dissected aorta should be limited to the ascending aorta in octogenarians; deep hypothermic circulatory arrest for simultaneous aortic arch replacement should be avoided if the aortic arch does not threaten to rupture.
Aortic valve stenosis in octogenarians
Aortic valve replacement is well tolerated
Only severe associated comorbidities should contraindicate surgery
Calcification of the ascending aorta produces cerebral embolisation in 10% of patients
Tissue valves are best
Postoperative survival is similar to a control population
Survival without operation in symptomatic patients is extremely short
Indications for percutaneous balloon dilatation are limited
Mitral valve disease
Mitral valve regurgitation
Indication for surgery
Chronic mitral valve insufficiency is the second most common operated valve disorder in the elderly, and represents 30–35% of the valvular surgery caseload.4 ,5 Although chronic regurgitation causes damage to the left ventricle before symptoms occur, surgery in octogenarians should not be considered in asymptomatic patients. Chronic regurgitation is usually caused by myxomatous degeneration of the valve or by ischaemic dysfunction of the left ventricle.12 With time, the mitral annulus dilates and regurgitation worsens. Degenerative regurgitation is typically caused by prolapse of the leaflets and ischaemic regurgitation by restricted motion of the leaflets. The distinction is, however, at times difficult; mild degrees of myxomatous degeneration and coronary artery disease frequently coexist in this age group. The distinction is not relevant when the valve needs be repaired or replaced on because the same surgical techniques are used. It is, however, important in patients operated on primarily for coronary artery disease and presenting mild to moderate degrees of regurgitation. Regurgitation may regress with improved myocardial perfusion and contractility. In these patients, intraoperative transoesophageal echocardiography provides a convenient way to assess the valve. If regurgitation is mild after induction of anaesthesia, it should be left untouched and later handled with vasodilators if systemic afterload is increased. If it is moderate, some surgeons will opt for the same conservative management while others will choose to implant an annuloplastic ring. If it is severe, correction is required.
Repair or replacement of the mitral valve
Repair of mitral insufficiency caused by myxomatous degeneration can often be achieved by application of simple and reliable techniques. Resection of the part of the leaflets that prolapses (with readaptation of the leaflet) and remodelling the annulus with a ring are often successful. The ring reduces the increased anteroposterior diameter of the mitral valve and brings the two leaflets closer together and improves their coaptation. Replacement of the mitral valve can be performed with preservation of the subvalvar apparatus in cases of myxomatous degeneration, but frequently requires its sacrifice in ischaemic regurgitation (and in mitral stenosis). Preservation of the subvalvar apparatus prevents the unfavourable globular remodelling of the left ventricle. This remodelling and fixation of the posterobasal part of the ventricle to the valve acutely diminishes ventricular systolic function.
The choice of prosthesis in the mitral position is debatable. Many surgeons select a biological prosthesis, which allows avoidance of anticoagulation or maintenance of anticoagulation at a low level when atrial fibrillation and massive dilatation of the atria coexist. Implantation of these prostheses is, however, more difficult than implantation of mechanical ones. For this reason (and especially in case of atrial fibrillation) some surgeons opt for a mechanical prosthesis. Finally, the stented commissures of a bioprosthesis protrude into the left ventricular outflow tract after implantation, and may create a subaortic obstruction when the left ventricle is not dilated. In the case of a small left ventricle, as occurs in acute forms of mitral regurgitation and in pure mitral stenosis, implantation of a low profile mechanical valve is a safer alternative.
Repair or replacement of the mitral valve can be technically challenging when the annulus is heavily calcified. The calcifications often extend to the epicardium of the atrioventricular groove. Overzealous decalcification can result in a non-repairable atrioventricular disconnection or in a delayed rupture of the left ventricle, which typically occurs a few hours after vigorous ventricular contraction. Partial decalcification of the annulus may lead to paraprosthetic leaks caused by the poor adaptation of the prosthesis ring to the rugged annulus.
Results of surgery
Mitral valve repair for regurgitation usually yields excellent results and should be attempted in the majority of elderly patients, even if only a less than perfect repair can be achieved. In a series of 100 patients older than 65 years, operative mortality was 4% and survival rate at one year was 90% after mitral valve repair.12 The impact of valve repair on survival and quality of life in octogenarians is currently unknown because of the small number of patients reported. Replacement of the mitral valve is not so well tolerated. The mortality rate in octogenarians fluctuates between 10–20%, and subsequent survival rates are 80%, 64%, and 41% at one, three, and five years, respectively.13 ,14
Mitral valve regurgitation in octogenarians
Surgery only in symptomatic patients
Functional regurgitation in ischaemic cardiomyopathy often regresses with myocardial revascularisation
Repair is often obtained with simple manoeuvres and provides more superior results than replacement
Mild residual regurgitation after repair should be accepted
Severe annular calcification is an additional risk for valve replacement
Bioprostheses are more difficult to implant and their superiority over mechanical prostheses is marginal
Mitral valve stenosis
Mitral valve stenosis is rare in octogenarians (1% of the valve surgery caseload), but still prevalent in septuagenarians. Valvar morphology is often not favourable for repair because of extensive calcification, rigidity, and retraction of all the valve components. Again, surgery is best recommended to patients with disabling symptoms only. Percutaneous balloon commissurotomy has been proposed as an alternative to surgery in high risk patients. In experienced hands, the procedural mortality in patients older than 70 years was 5% and improved transvalvar haemodynamics (mitral valve opening area > 1.5 cm2 with mitral regurgitation ⩽ 2+) was achieved immediately in 50% of patients and persisted for three years in 30%.15 Surgery, however, with an increased mortality to 20%, was necessary in 50% of patients within three years. Although better than on the aortic valve, the haemodynamic improvement after mitral valvoplasty vanishes rapidly and can be considered only as a palliative, often temporary measure.