Article Text

Abstract
Objective To avoid preventable consequences of perinatal hepatitis B infection, all infants should be given hepatitis B vaccine (HBV) within 24 hours of birth if birth weight is ≥2 kg and at 30 days of life or at discharge if <2 kg, to provide highest seroprotection rates while ensuring universal vaccination prior to discharge. We aimed to achieve timely HBV administration in >80% of eligible infants in both birthweight groups and decrease infants discharged home without receiving HBV to <1% over an 18-month period and sustain results for an additional 15 months.
Methods Data were collected from June 2016 to May 2020 in a level III neonatal intensive care unit. A multidisciplinary team identified barriers and interventions through Plan-Do-Study-Act cycles from September 2017 to February 2019: using pharmacists as champions, overcoming legal barriers, staff education and best practice alerts (BPAs) embedded in electronic health records. Statistical process control (SPC) p charts were used to evaluate the primary outcome measure, monthly percentage of infants receiving timely HBV administration stratified by birthweight categories (≥2 and <2 kg). For infants receiving HBV outside the time frame, absolute difference of timeliness was calculated.
Results Mean timely HBV administration improved from 45% to 95% (≥2 kg) and from 45% to 85% (<2 kg) with special cause variation in SPC charts. Infants discharged without receiving HBV decreased from 4.6% to 0.22%. Of those given HBV outside the recommended time frame, median absolute time between recommended and actual administration time decreased significantly: from 3.5 days (IQR 1.6, 8.6) to 0.3 day (IQR 0.1, 0.8) (p<0.001) in ≥2 kg group and from 6 days (IQR 1, 15) to 1 day (IQR 1, 6.5) (p=0.009) in <2 kg group.
Conclusions Using a multidisciplinary approach, we significantly improved and sustained timely HBV administration and nearly eliminated infants discharged home without receiving HBV. Pharmacists as champions and BPAs were critical to our success.
- paediatrics
- control charts
- run charts
- quality improvement
- PDSA
- hospital medicine
Data availability statement
Data are available upon reasonable request. Please contact the corresponding author to discuss the feasibility of obtaining access to a deidentified data set.
Statistics from Altmetric.com
Introduction
Hepatitis B vaccine (HBV) is 75%–95% effective in preventing perinatal hepatitis B (HB) transmission when given within the recommended time frame1 2 which is particularly important for those infants whose mothers were not appropriately identified prenatally, those at risk for household exposures and preterm infants who are more likely to receive blood transfusions and surgical procedures. The vaccine is life-saving, provides lifelong protection and is cost-effective.3 To avoid preventable consequences of perinatal HB infection, all infants should be given their birth dose HBV within the recommended time frame to provide universal routine prophylaxis. However, timely administration has been suboptimal in premature infants.
Premature infants are undervaccinated at time of discharge4 and often fail to catch up during childhood.5–7 Proper vaccination is essential to protect the vulnerable preterm population from vaccine-preventable diseases. When infants receive any vaccination prior discharge from the hospital, they are more likely to receive vaccinations in the future.8 Therefore, administering this birth dose HBV in the hospital is crucial to provide a safety net and in promoting successful future vaccinations.
For premature infants, most vaccines can be given using the same schedules as recommended for full-term infants regardless of gestational age or birth weight.9 However, administration timing of HBV for infants born to mothers negative for HB depends on infant’s birth weight because of lower immunological response among infants with birth weights <2 kg.10 The American Academy of Pediatrics (AAP) published revised guidelines to vaccinate infants <2 kg born to HB-negative mothers at 30 days of life or at time of discharge whichever came first to provide the highest seroprotection rates as well as ensuring every infant receives their birth dose prior to leaving the hospital. For infants whose maternal HB status is positive or unknown, HBV is administered within 12 hours regardless of birth weight along with HB immune globulin (HBIG) if mother’s status is confirmed positive or remains unavailable.11
We used an algorithm adapted from this AAP Policy Statement11 rescinding the prior permissive language allowing providers option to delay birth dose administration as our guideline: for infants born to HB-negative mothers, administer HBV within 24 hours of life if ≥2 kg; administer HBV at 30 days of life or at time of discharge whichever comes first if <2 kg. We found at baseline only 45% of infants in both birthweight categories met timely HBV administration and 4.6% were discharged without receiving their birth dose. The rounding neonatologist educated the team of residents, advanced practice providers (APPs), nurses and pharmacists of the revised guidelines on daily rounds but had minimal effect.
Our SMART (Specific, Measurable, Achievable, Relevant and Timely) aim was to increase the mean percentage of timely HBV administration within the recommended time frame from 45% to >80% of eligible infants in both birthweight groups and decrease infants discharged home without receiving HBV from 4.6% to <1% over an 18-month period, then sustain it for an additional 15 months.
Methods
Setting
Our neonatal intensive care unit (NICU) is a 25-bed level III nursery in an urban academic safety net hospital with over 3500 deliveries and approximately 400 NICU admissions annually. The majority of infants are inborn, more than 95% are discharged home from our unit and the majority (91%) are Medicaid insured. One-quarter of infants have birth weight <2 kg. The unit is staffed by four neonatologists, four APPs, three paediatric pharmacists and paediatric residents rotating monthly.
Inclusion and exclusion criteria
All infants admitted to our NICU were eligible. Exclusion criteria included death or transfer to another hospital prior to the time HBV was due, and those medically unstable (per recommended guidelines)12 determined by the infant’s provider. We also excluded infants whose parents declined vaccination. Infants who met inclusion criteria were stratified by birthweight categories (≥2 and <2 kg).
Interventions
Plan-Do-Study-Act cycle 1: formulating a multidisciplinary team (September 2017)
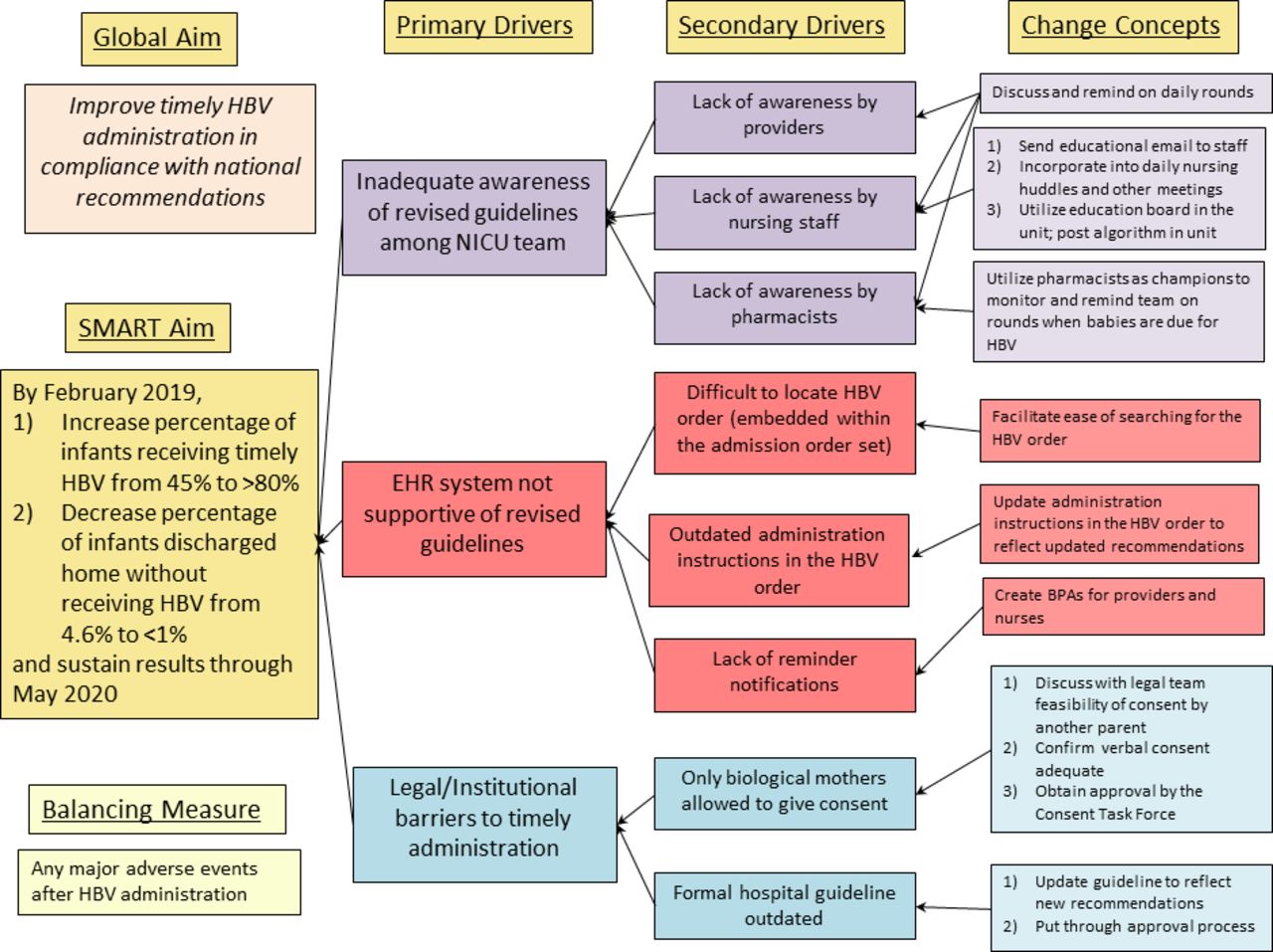
We formed a multidisciplinary team composed of paediatric pharmacists, NICU nurses, neonatologist, well-baby nursery physicians, well-baby and labour and delivery nurse educators and electronic health record (EHR) analyst. The team asked staff what barriers they were experiencing in administrating HBV in a timely manner. We then reviewed the current process and barriers, identified key processes where improvements were needed, and created a key driver diagram (figure 1) and identified three primary drivers: (1) inadequate awareness of revised guidelines among NICU team members, (2) EHR system not supportive of revised guidelines, and (3) legal and institutional barriers to timely administration.
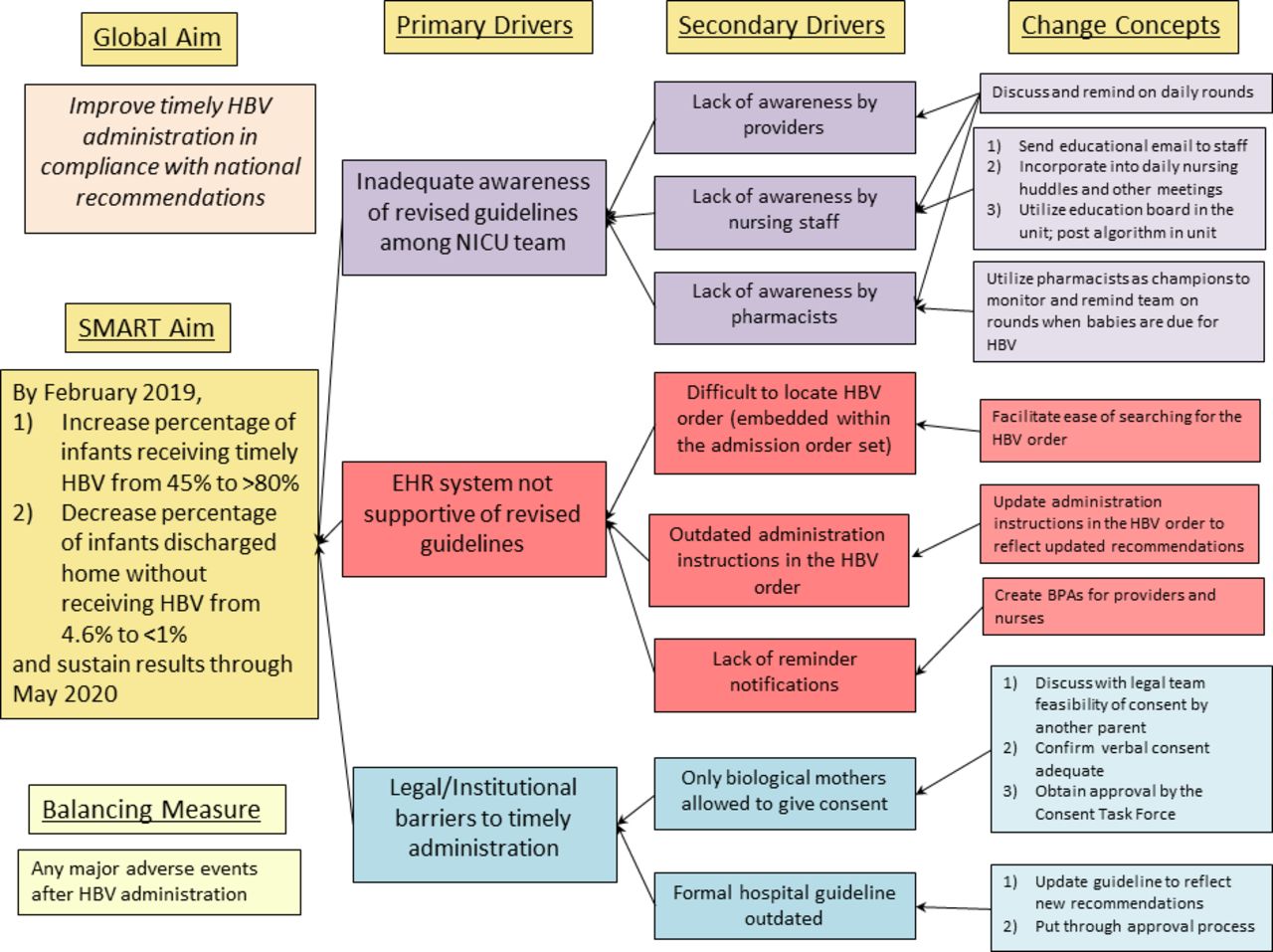
Key driver diagram showing aims, key drivers and change concepts. BPA, best practice alert; EHR, electronic health record; HBV, hepatitis B vaccine; NICU, neonatal intensive care unit; SMART, Specific, Measurable, Achievable, Relevant and Timely.
Plan-Do-Study-Act cycle 2: pharmacists as champions (November 2017)—targeting inadequate awareness of revised guidelines
The paediatric pharmacist rounding daily with the team would make suggestions regarding HBV administration recommendations according to guidelines. However, this was often inconsistent, lacking a systematic method and incorrect as they were following the outdated guidelines. Since paediatric pharmacists are a small, consistent team who participate in daily rounds and dispense the vaccine, they were designated as the champions.
The group tracked each NICU infant’s HBV eligibility/completeness status each morning by chart review, then communicated among their pharmacy peers. In March 2019, an electronic handoff note feature which became part of the permanent medical record was created. In July 2019, they then created a standardised ‘to-do’ checklist to better automate the process. This checklist was visible to all pharmacy members including when the unit census was printed and available for rounds. This also added the ability to check off the box when HBV was given. This method enabled the pharmacists to track easily which infant still needed HBV prior to daily rounds, remind the team on rounds when it was due and document HBV completion.
Plan-Do-Study-Act cycle 3: verbal and parental consent (May 2018)—targeting legal and institutional barriers to timely administration
Prior to interventions, the person consenting for the infant’s vaccination was limited to the biological mother. However, frequently she was not easily available which delayed consent. When she did consent, it was unclear if verbal consent was sufficient and whether a system for consistent documentation existed.
We clarified verbal consent was sufficient by the hospital legal team. The parent consenting would be given the Vaccine Information Sheet (VIS) and this was to be documented in the Medication Administration Record by the nurse. In situations where biological mothers were not available to consent, we received approval for the other parent to consent.
Plan-Do-Study-Act cycle 4: nurse education (May to August 2018)—targeting inadequate awareness of revised guidelines
The entire NICU team lacked knowledge of the updated guidelines leading to the delay of vaccination or no vaccine administration. To address this, nursing staff education was provided over several months. This consisted of emailing the updated guidelines and algorithm to all staff, informative briefings at daily nursing huddles, posting the algorithm at all nursing stations, using an educational bulletin board in the unit and reminders from neonatologists and pharmacists on daily rounds. We also discussed this change in monthly NICU team meetings and bimonthly nurse staff meetings.
Plan-Do-Study-Act cycle 5: HBV order searchable (July 2018)—targeting EHR system not supportive of revised guidelines
Because the HBV order was embedded within the admission order set in the EHR, all HBV orders were placed at time of NICU admission by the provider regardless of birth weight. If an infant was <2 kg, this order was discontinued. Later during the hospital admission, when the team needed to order HBV, locating the order was difficult and time consuming of providers and pharmacists’ time. In addition, the administration instructions listed with the order were outdated and incorrect.
The HBV order that was embedded within the admission order set was created into an individualised order which was easily searchable and accessible for the ordering provider at a later time. The administration instructions were also updated to reflect the new guidelines and included that verbal consent was needed by a parent prior administration.
Plan-Do-Study-Act cycle 6: formal hospital guideline (January 2019)—targeting legal and institutional barriers to timely administration
The official online HBV hospital guideline was outdated reflecting the old recommendations. To formalise this, it was updated to reflect revised recommendations, included the AAP algorithm11 and clarified that either parent was now able to provide consent. This guideline was approved by well-baby nursery and NICU team representatives. Although the approval process took longer than expected, updating the hospital guideline allowed providers to easily electronically access the new recommendations.
Plan-Do-Study-Act cycle 7: best practice alerts (February 2019)—targeting EHR system not supportive of revised guidelines
With substantial staff and resident turnover, we needed a systematic method to ensure sustainability. To overcome this, best practice alerts (BPAs) were developed in the EHR. After discussion among the multidisciplinary team, we had BPAs fire for ≥2 kg infants only to the nursing staff so infants who were transferred between NICU and well-baby nursery would not be missed. For infants <2 kg, BPAs fired for providers with a direct link to the HBV order allowing immediate ordering if not already done. This feature took longer than expected to launch within our EHR but was considered an essential tool for sustaining results.
Study of the interventions
Data were extracted from the EHR on all infants admitted to our NICU including birth weight, gestational age, inborn or outborn status, date and time of birth, and time of HBV administration and discharge. Data were abstracted retrospectively during the preintervention phase (June 2016 to August 2017), and prospectively during the intervention phase (September 2017 to February 2019) and the postintervention phase (March 2019 to May 2020). The charts of infants who did not receive timely HBV administration were reviewed by one author (MH) to determine the reason the vaccine was not administered on time.
Data for process and balancing measures including the pharmacists’ documentation of HBV eligibility/completeness tracking, documentation of VIS provision to the consenting parent, administration of HBIG, administration of intramuscular epinephrine and listing of HBV as allergy/contraindication were retrieved through chart reviews from July 2017 to May 2020 by three authors (MH, SS, GR). Nurse attendance at staff meetings was collected using attendance records and meeting minutes kept by the nurse manager. The EHR was queried for the number of times the BPA fired and the number of times an order was placed for HBV from the BPA between February 2019 and May 2020.
Measures
The primary outcome measure was mean timely HBV administration defined as administered within 24 hours of birth for infants with birth weight ≥2 kg, or administered on day of life 30±24 hours or within 24 hours of day of discharge (whichever came first) for infants with birth weight <2 kg. For infants who failed to receive HBV timely, the absolute difference in time between the actual administration and the appropriate window to receive HBV was calculated. Secondary outcome measure was the percentage of infants who never received their birth dose before discharging from NICU.
The process measures were (1) percentage of infants with pharmacists’ documentation of HBV eligibility/completeness tracking, (2) percentage of infants with documentation of VIS provision to ensure verbal consent obtainment, (3) percentage of nurse attendance at staff meetings during educational sessions, and (4) median number of times the BPA fired per infant per month and percentage of fired BPAs from which an order for HBV was entered. The balancing measure was any major adverse events after HBV administration.
Analysis
The mean percentage of infants in a month receiving timely HBV prior to discharge for ≥2 and <2 kg infants was plotted on statistical process control (SPC) p charts. Three sigma limits were used to set the upper and lower control limits. The SPC p charts were created using QI Charts version 2.0.22 (Scoville Associates, Texas). Standard SPC charting rules for determining special cause (ie, 8 or more consecutive points above or below the centreline, a single point outside the control limits, 6 consecutive points increasing or decreasing, 2 out of 3 consecutive points near a control limit or 15 consecutive points close to the centreline) were used as evidence of improvement.13 The number of times the BPA fired per month was divided by the number of infants admitted to the NICU during each month. Continuous variables, which included timeliness of HBV administration and the process measure of median number of times the BPA fired per infant per month, were presented as medians with IQRs as their distributions were not normal and analysed with the Kruskal-Wallis test and Mann-Whitney U test. Χ2 and Fisher’s exact tests were used to analyse categorical variables which included any adverse events after HBV administration. For other process and balancing measures, percentages with 95% CIs were reported. Statistical analyses were performed with SPSS V.22 (IBM SPSS).
Results
The number of infants ≥2 kg in each of the phases was as follows: 379 infants in the preintervention phase, 363 infants in the intervention phase and 349 infants in the postintervention phase. In the <2 kg group, there were 103, 136 and 137 infants in each phase, respectively. Gestational age, birth weight, percentage of inborn, total excluded infants or infants excluded due to death, transfer or medically unstable were similar across the three phases for both birthweight categories (table 1). Parental deferral in the ≥2 kg group was higher in the intervention phase (5.8%) and postintervention phase (4.9%) as compared with the preintervention phase (2.1%) (p=0.009 and p=0.04, respectively). Parental deferral across the phases was not different in infants <2 kg (table 1).
Demographics of patient population and excluded infants
Outcome measures
Mean timely HBV administration (SPC charts)
For ≥2 kg infants, the mean monthly percentage of infants receiving timely HBV increased from a baseline mean of 45% to 76%, then to 95% after intervention implementations (figure 2). Similarly, for <2 kg infants, the mean monthly percentage of infants receiving timely HBV increased from a baseline mean of 45% to 71%, and to 85% after interventions (figure 3). After Plan-Do-Study-Act (PDSA) 1 and 2, and again after PDSA 3–5, there were runs of eight consecutive points above the centreline for both the ≥2 and <2 kg infants. Updated mean and controls limits were plotted in the SPC charts after special cause was detected. Improvements in both groups have been sustained for nearly 2 years.
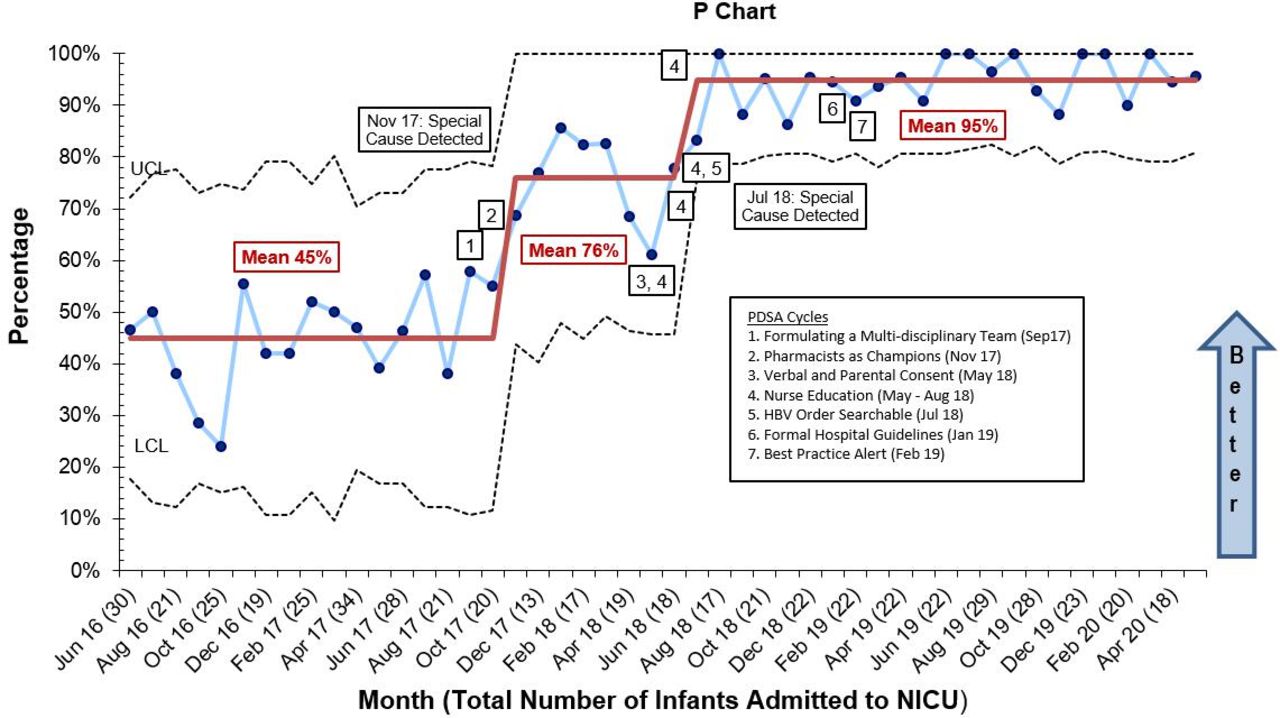
Percentage of eligible newborns ≥2 kg receiving timely hepatitis B vaccine (HBV) prior to discharge from the neonatal intensive care unit (NICU) by month. LCL, lower control limit; PDSA, Plan-Do-Study-Act; UCL, upper control limit.

{kind=link}
{kind=link}
{kind=link}
Percentage of eligible newborns <2 kg receiving timely hepatitis B vaccine (HBV) prior to discharge from the neonatal intensive care unit (NICU) by month. LCL, lower control limit; PDSA, Plan-Do-Study-Act; UCL, upper control limit.
For infants ≥2 kg who received HBV vaccine late (>24 hours after birth), the median number of days between inappropriate time of HBV administration and what would have been the appropriate time for vaccination decreased significantly during the intervention phase (0.8 days, IQR 0.3, 2.5) and postintervention phase (0.3 days, IQR 0.1, 0.8) compared with preintervention phase (3.5 days, IQR 1.6, 8.6) (p<0.001).
For infants <2 kg at birth who received HBV vaccine either early (before 29 days of life or >1 day prior discharge) or late (after 31 days of life), the absolute median number of days between inappropriate time of HBV administration and what would have been the appropriate time for vaccination did not change significantly (p=0.78) between preintervention phase (6 days, IQR 1, 15) and intervention phase (8 days, IQR 1, 22) but did decrease significantly to 1 day (IQR 1, 6.5) in the postintervention phase as compared with the preintervention and intervention phases (p=0.009).
Of infants born to mothers of HB-positive or unknown status, one of three infants did not receive timely HBV administration (ie, within 12 hours of life) during preintervention phase. However, all infants in intervention phase (6/6) and postintervention phase (3/3) received HBV within 12 hours of life as recommended per AAP guidelines in these cases to prevent perinatal transmission.
Decreasing percentage of infants discharged home without receiving HBV
Of the eligible infants, the proportion of infants discharged home without receiving HBV decreased significantly. In the preintervention phase, 3.4% (95% CI 2% to 6%) in the ≥2 kg group and 8.7% (95% CI 5% to 16%) in the <2 kg group never received HBV prior to leaving the NICU. During the intervention and postintervention phases, no infant ≥2 kg (639 eligible infants, p<0.001) and only 0.91% infants <2 kg (2/218 eligible infants, p<0.001) did not receive HBV prior to discharge. Both of these infants received HBV at their initial follow-up visit after discharge.
Process measures
Tracking HBV eligibility/completeness by pharmacists (PDSA cycle 2)
From March through June 2019 when implementing the trackable handoff note feature, documentation was present in 68% of infants (76/111, 95% CI 59% to 77%). From July 2019 through May 2020 after implementing a standardised electronic checklist, 81% of infants (269/334, 95% CI 76% to 85%) had HBV eligibility/completeness tracked in the checklist, 7% of infants (24/334, 95% CI 5% to 11%) still showed the previous process (in July and August 2019) and 12% of infants (41/334, 95% CI 9% to 16%) had no documentation.
Ensuring verbal consent obtainment (PDSA cycle 3)
Baseline data (July to August 2017) showed 100% of infants (n=49, 95% CI 93% to 100%) had documentation of VIS provision. Of 890 infants who received HBV during the intervention and postintervention phases, 100% of infants (95% CI 99.6% to 100%) had documentation of VIS provision to the consenting parent in the EHR.
Nurse attendance at staff meetings (PDSA cycle 4)
We provided several forms of nursing staff education including during monthly NICU team meetings and bimonthly nurse staff meetings. Individual nurse attendance at one or both of these meetings was 60% (27/45, 95% CI 44% to 74%).
Number of times the BPA fired per infant per month and percentage of fired BPAs from which an order for HBV was entered (PDSA cycle 7)
The BPA fired a median number of 2.2 times (IQR 1.1, 6.9) per infant per month from February 2019 to May 2020. The percentage of fired BPAs which resulted in an HBV order being entered into the EHR was 13.6% (95% CI 11.1% to 16.5%).
Balancing measure
Adverse events secondary to HBV administration
There were no adverse events documented after HBV administration in the intervention and postintervention phases including anaphylaxis or allergic reactions (0/890, 0%, 95% CI 0% to 0.4%) requiring administration of intramuscular epinephrine.
Discussion
By using several PDSA cycles, we were able to achieve our SMART aim and improve mean timely HBV administration from 45% to over 80% in both birthweight categories and decrease rate of infants discharged home without receiving HBV from 4.6% to only 0.22% (2/893) over an 18-month period and sustain these improvements for 15 months. Key lessons learnt included the importance of taking a multidisciplinary approach, identifying and using pharmacists as champions, overcoming legal barriers, repetitive staff education and utilisation of EHR functions. Most importantly, pharmacists and utilisation of BPAs were key to our success as we continue to attain >80% mean timely HBV administration in both groups nearly 2 years after intervention completion.
We observed the first significant improvement in timely HBV administration with the support of our pharmacists. Pharmacists have proven to be very effective when involved in QI projects to decrease medication errors and reduce staff time.14 15 Instead of using a NICU clinical assistant to track HBV eligibility in an external database as done by Stetson et al,16 our pharmacists were able to adapt a simple and readily available standardised electronic checklist embedded in the EHR, which was easily accessible for monitoring on daily rounds, added ability to track HBV completion and remained part of the medical records. This allowed consistent reminders and achieving timely vaccination. The pharmacists were critical to our success.
Although we have a small group of core providers, our staff pool is larger and different paediatric residents rotate through every month. As shown in figures 2 and 3, our improvements waned 7 months into the initiative possibly reflecting decreased awareness in the unit, portraying the difficulty in sustaining improvement by solely relying on providers. Though staff attendance at staff meetings did not reach 100%, after continuing education and reminders to our staff over the next 4 months, having administration guidelines readily available in the unit and implementing hard-wired solutions such as BPAs, we were able to sustain improved results.
Most importantly with these interventions, we nearly eliminated infants discharged home without receiving their birth dose HBV. The two infants who did not receive HBV before discharge both received it at their first outpatient follow-up visit. One infant’s mother was critically ill and no other parent was available to provide consent prior to the infant’s discharge. This alerted us to a possible need for expanding legal consent options for rare circumstances.
Utilisation of BPAs was important in sustaining the effects. BPAs have proven to be a very effective and useful tool in improving quality of care,17 decreasing unnecessary costs18 and improving vaccination completeness in adults19 and infants.20 Ernst20 noted the need for on-the-spot vaccine ordering from the BPA to further increase vaccination rates. In our study, we included a link allowing providers to directly place the HBV order from the BPA which only occurred 13% of fired BPAs, but our mean timely percentage of HBV administration was already quite high (95% in ≥2 kg and 85% in <2 kg groups) when BPAs were implemented. As we continue to achieve high percentages of mean timely HBV administration 2 years after intervention completion, we believe the BPAs were critical for sustainability. We must be cognisant though not to overuse this function since this may lead to alarm fatigue from users.21 22 Others have seen a gradual decrease in response over prolonged exposure to BPAs23 so ongoing assessment of compliance will be critical in sustaining our improvements.
Our study had several limitations. First, this study reflects a single centre’s experience. Our success may have been related to the smaller size of our NICU and group of staff. Whether similar methods are generalisable to larger, higher acuity units is unclear although Stetson et al and Ernst16 20 have improved overall vaccination rates in level IV NICUs. In addition, we believe our sustainability was related to the capability of our EHR with BPAs; if this functionality is not available to a NICU, our interventions will not be applicable.
The relatively small monthly sample size in the <2 kg group resulted in variability in our results for this group as seen in the widely spread upper and lower control limits of the SPC charts. Small sample sizes result in unstable estimates for the outcome variable and limit its reliability.
One can argue the lack of clinical relevance of timely HBV administration as long as infants are immunised before discharge from NICU. Though rare, there are reported cases where mothers are not appropriately identified as HB positive prenatally.24 Although there were only a small number of infants born to mothers of HB-positive or unknown status in our study, by improving timely HBV administration, we are able to provide protection to these infants while investigating mother’s status. In addition, for the <2 kg group, by administering HBV as close to 30 days of life this allows infants to be eligible to receive subsequent combination vaccines starting at 2 months of age having the minimum 4 weeks of interval needed in between the first and second HBV doses. This allows for a single injection rather than several individual injections minimising pain and prevents further delay of other needed vaccinations that should be given promptly at 2 months of chronological age.
Another limitation was that we excluded infants whose parents declined the vaccine. The rate of parental deferral was higher in the intervention and postintervention phases compared with preintervention phase in ≥2 kg group. However, the proportion of affected infants is small and unlikely to have impacted our results. It is unclear whether these infants whose parents deferred HBV will continue to defer or delay vaccines later in their childhood. Lauderdale et al 25 found that when infants received their HBV birth dose, administration rates for all other future infant vaccines were improved, highlighting the importance of improving NICU HBV administration. It will be interesting to see whether infants who did not receive their birth dose HBV continue to be incomplete in other vaccinations.
Conclusions
This study used basic quality improvement methodologies to identify several barriers and implement change interventions in a structured manner to improve timely HBV administration and vaccinate almost all infants prior to discharge. Engaging the pharmacists and use of automated EHR functions such as BPAs may aid in achieving and sustaining improvements in compliance with timely vaccination, reducing risk of acquisition of preventable serious infection in neonates.
Data availability statement
Data are available upon reasonable request. Please contact the corresponding author to discuss the feasibility of obtaining access to a deidentified data set.
Ethics statements
Patient consent for publication
Ethics approval
The hospital Quality Improvement Review Committee determined that this project was not human subjects research and did not require Institutional Review Board review.
References
Footnotes
Contributors MH conceptualised and designed the study and data collection method, collected data, carried out the initial analyses and interpretation, drafted the initial manuscript and reviewed and revised the manuscript. TRG interpreted the data and reviewed and revised the manuscript for important intellectual content. SS conceptualised and designed the study, collected data and reviewed and revised the manuscript. TS conceptualised and designed the study and reviewed and revised the manuscript. GR collected data, analysed and interpreted the data and reviewed and revised the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.