Article Text

Abstract
Background Antibiotics are extensively prescribed in intensive care units (ICUs), yet little is known about how antibiotic-related decisions are made in this setting. We explored how beliefs, perceptions and contextual factors influenced ICU clinicians’ antibiotic prescribing.
Methods We conducted 4 focus groups and 34 semistructured interviews with clinicians involved in antibiotic prescribing in four English ICUs. Focus groups explored factors influencing prescribing, whereas interviews examined decision-making processes using two clinical vignettes. Data were analysed using thematic analysis, applying the Necessity Concerns Framework.
Results Clinicians’ antibiotic decisions were influenced by their judgement of the necessity for prescribing/not prescribing, relative to their concerns about potential adverse consequences. Antibiotic necessity perceptions were strongly influenced by beliefs that antibiotics would protect patients from deterioration and themselves from the ethical and legal consequences of undertreatment. Clinicians also reported concerns about prescribing antibiotics. These generally centred on antimicrobial resistance; however, protecting the individual patient was prioritised over these societal concerns. Few participants identified antibiotic toxicity concerns as a key influencer. Clinical uncertainty often complicated balancing antibiotic necessity against concerns. Decisions to start or continue antibiotics often represented ‘erring on the side of caution’ as a protective response in uncertainty. This approach was reinforced by previous experiences of negative consequences (‘being burnt’) which motivated prescribing ‘just in case’ of an infection. Prescribing decisions were also context-dependent, exemplified by a lower perceived threshold to prescribe antibiotics out-of-hours, input from external team members and local prescribing norms.
Conclusion Efforts to improve antibiotic stewardship should consider clinicians’ desire to protect with a prescription. Rapid molecular microbiology, with appropriate communication, may diminish clinicians’ fears of not prescribing or of using narrower-spectrum antibiotics.
- antibiotic management
- critical care
- decision making
- qualitative research
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Intensive care units (ICUs) are unique environments where clinicians often make antibiotic decisions under diagnostic uncertainty and with high-stakes consequences. During decision-making, intensivists must balance heightened priorities of patients’ needs with antimicrobial stewardship (AMS) initiatives; how ICU doctors navigate these trade-offs remains poorly understood.
Critical care patients frequently exhibit ‘traditional’ signs of infection (eg, fever) even when no infection is present; consequently differentiating infection from non-infectious conditions is challenging.1 Furthermore, infections may be viral rather than bacterial, with only the latter requiring antibiotics. Undertreating bacterial infections or delaying antibiotics in ICU may increase the risk of mortality2; conversely, unnecessary therapy increases the risk of antibiotic-related side effects, including adverse drug reactions and infection with Clostridium (Clostridiodes) difficile,3 and promoting antimicrobial resistance (AMR).4
The development of AMR is of particular concern in ICU. Many patients have multiple comorbidities, histories of frequent hospital admissions, long hospital and ICU stays, multiple prior antibiotic courses, and complex physiologies; these factors can lead to underdosing and overdosing and are ideal circumstances for antibiotic toxicity and AMR development. These risks are compounded by invasive device usage, high broad-spectrum antibiotic exposure and ICU treatment intensity.5 Consequently, intensivists have seen an increasing prevalence of resistance and treatments failing due to AMR.6
Accordingly, antibiotic decisions have high levels of consultant intensivist and microbiologist involvement, and ICU-specific AMS programmes have been developed.7 8 Yet up to 70% of ICU patients receive antimicrobial therapy,9 despite up to half having no confirmed infection.2
Outside the ICU, studies have identified the importance of clinicians’ beliefs about their prescribing’s consequences,10 AMR perceptions,11 and social and professional influences.12 However, these studies have variously excluded intensivists,13 combined ICU and non-ICU wards,14 15 only included non-ICU wards,16 17 or did not specify which wards were included.18
The Necessity Concerns Framework (NCF) may help to understand antibiotic decision-making. Extensively used to understand patients’ medication adherence, NCF posits that decisions to start and continue with treatments are influenced by how individuals judge the necessity for treatment relative to their concerns about the actual or potential adverse consequences of taking it.19
Like Hulscher and colleagues,12 we applied a social and behavioural approach investigating clinicians’ perspectives of antibiotic decision-making (‘clinician perceptions’) and the social and environmental aspects surrounding these perceptions (‘contextual factors’). We explore these factors’ influence on ICU antibiotic decision-making, interpreting our findings using NCF.
Methods
This research is part of the INHALE programme (ISRCTN16483855) investigating molecular diagnostic utility for pneumonias in ICU.20 A randomised controlled trial is being conducted whereby patients with suspected pneumonias are randomised to receive either standard care or decision-making support from a point-of-care molecular diagnostic test. A behavioural evaluation examines antibiotic decision-making and clinicians’ willingness to adopt molecular tests. Before the trial, we strove to understand how ICU antibiotic decisions were made.
This study is reported following the Standards for Reporting Qualitative Research guidelines.21 It used focus groups and vignette-based interviews (VBIs) and followed a contextualist approach positing that the external context affects individuals’ interpretation of their experiences.22 All participants provided informed consent.
Study design
Focus groups explored contextual factors perceived to influence antibiotic decisions. Through these discussions, clinicians shared and compared their prescribing attitudes and experiences, allowing exploration of a range of perspectives (see online supplemental table S1 for topic guide).23
Supplemental material
Interviews investigated antibiotic decision-making processes. These used clinical vignettes depicting hypothetical but realistic scenarios at key decision points (see online supplemental table S2 for vignettes and interview guides). Individuals applied their expertise and experience to determine a course of action based on provided information, followed by a wide-ranging and detailed discussion around raised issues. Cognitive processes elicited during VBIs simulate real-world decision-making,24 and researchers can compare participants’ responses and systematically reconstruct decision-making processes.
Sample and setting
This research occurred in the ICUs of four English hospitals (see table 1 for the characteristics). We chose these sites due to their differences in patient populations and in general prevalence of resistant bacteria. Convenience sampling was used; clinicians participated whenever they could spare time from clinical duties. Focus groups were prescheduled, whereas VBIs were opportunistic. NB, YJ and DB recruited participants through local promotion; NB and YJ have clinical pharmacy backgrounds and DB is an ICU consultant at a participating site.
Participating hospital and intensive care unit characteristics
In UK ICUs, consultants (‘attending’ level permanent staff with usually over 10 years of experience) make most antibiotic decisions, aided by visiting clinical microbiologists, typically consultant level. ICUs are ‘closed units’—consultant intensivists have ultimate decision-making power for patients. Members from teams like microbiology and surgery can give recommendations but cannot change aspects of the patient’s management without consultant intensivist permission. ICU middle-grade (5–7 years of experience) and early-grade (up to 4 years of experience) trainees occasionally make antibiotic decisions, usually in urgent out-of-hours settings. Pharmacists aid with dosing and monitoring antibiotics, including choice and treatment durations.
All staff involved in ICU antibiotic prescribing could participate in focus groups; recognising that decision-making involves the team, non-prescribers were included. VBI participants were individuals who would actively prescribe on ICU (ie, consultant intensivists and trainees).
Data collection
NB and YJ conducted all focus groups and VBIs. Focus groups were semistructured and began with ‘What factors do you think influence your decisions around antimicrobial prescribing on your ICU?’ The moderators used predetermined follow-up prompts about contextual factors influencing prescribing. One focus group was conducted at each site; three were face-to-face and one was a teleconference. Four focus groups were deemed sufficient as previous research found that all prevalent themes could be identified in three.25 Focus groups lasted between 25 and 45 min and were undertaken between August and September 2018.
Semistructured interviews explored decision-making processes using two vignettes. Vignette 1 related to whether to start a patient on antibiotics, whereas vignette 2 depicted a patient currently on antibiotics where clinicians could choose to continue, change or stop antibiotics. Both patients had lower respiratory tract infections; these are common to ICU and are associated with diagnostic uncertainty. These scenarios had no ‘correct’ answers; rather, their purpose was to encourage reflection on decision-making processes. Five non-participating consultant intensivists pilot-tested the vignettes to ensure they were realistic and included sufficient information.
Paediatric clinicians were given analogous vignettes depicting children; otherwise, the same interview guides were used for all participants. VBIs were conducted face-to-face in each ICU, lasted between 7 and 40 min, and occurred between August and December 2018. Interviews and coding were iterative, with interviews conducted until data saturation (three consecutive interviews resulting in redundant information).26
Data analysis
All focus groups and interviews were audio-recorded, anonymised, professionally transcribed and entered into NVivo V.12. AMP (research psychologist), NB and YJ verified transcript accuracy. Data were first analysed using inductive thematic analysis, with themes constructed at a semantic level summarising content explicitly discussed by multiple clinicians.27
Data were open-coded, with codes refined and themes formed with input from the multidisciplinary team (see online supplemental table S3 for disciplines). We then adopted a deductive approach interpreting the generated themes using NCF.28 For instance, themes related to clinicians’ beliefs of antibiotic importance were classified as necessity perceptions. As focus group participants discussed their perceptions and VBI participants mentioned contextual factors, we treated both data sources as equally important and triangulated our findings between them.29
AMP conducted analyses, aided by NB, following Braun and Clarke’s30 approach: data familiarisation, generating codes, searching for themes, reviewing and defining themes, and writing the report.
Results
Audio recording duration was approximately 2.6 hours for focus groups and 9 hours for VBIs. Focus group participants largely agreed with each other; there were few if any points of tension. Table 2 shows participants’ characteristics.
Characteristics of study participants
Our overarching finding was that clinicians favoured starting or continuing antibiotics in uncertainty. Prescribing antibiotics was often perceived as necessary to protect patients and clinicians from deleterious immediate consequences. If clinicians were uncertain whether antibiotics were required, they favoured ‘erring on the side of caution’:
the easy default is to give an antibiotic and if you’re confident or overconfident or deluded or whatever, you sometimes hold. —P52, consultant, hospital 1, focus group
it’s 48 hours [until culture results come back]. I think you’ve got more tendency to try and prescribe something [antibiotics] just because it’s going to be… Until you know exactly there’s nothing going on. —P47, early-career trainee, hospital 4, VBI
I think they [intensivists] would be always being erring on the side of caution, you wouldn’t even stop it [antibiotics] if there is any suspicion of risk. —P40, pharmacist, hospital 2, focus group
Clinicians’ perceptions of antibiotic necessity outweighing antibiotic-related concerns underscore erring on the side of caution. Contextual factors also influenced this inclination to prescribe in uncertainty. We describe both themes in the following sections.
Clinician perceptions of antibiotic necessity outweighing concerns
Perceptions of the necessity to prescribe were related to beliefs that, in uncertainty, antibiotics provide protection for patients and clinicians. Clinicians were aware of and concerned about AMR, whereas they seldom mentioned concerns about the potential for antibiotics resulting in patient harm as key considerations. Concerns about antibiotic harm (individual and societal) were rarely prioritised to a degree where they outweighed perceived necessity, enabling clinicians to ‘be brave’ by withholding or stopping antibiotics. This encouraged antibiotic prescription and continuation in an approach characterised by erring on the side of caution. Table 3 shows supporting quotes.
Supporting quotations for clinician perceptions theme
Antibiotic necessity: prescribing protects patients against adverse consequences
When discussing antibiotic prescription, clinicians used the language of protection against adverse consequences rather than of actively ‘curing’ patients of infections. Decisions to start or continue antibiotics were influenced by the perception that antibiotics were necessary to prevent patient deterioration and mortality from infections (quote 1, table 3). Continuing antibiotics, rather than stopping early, was perceived as necessary to prevent AMR (quote 2, table 3). If clinicians were more certain of whether a patient had a bacterial infection or if they felt the course was completed and the antibiotics had led to clinical improvement, most were confident to stop (or withhold further) antibiotics. However, a minority viewed prescribing antibiotics as necessary ‘just in case’, despite believing that they were not currently required (quotes 2–3, table 3).
Antibiotic necessity: prescribing protects clinicians against adverse consequences
Clinicians believed that prescribing antibiotics was necessary to protect themselves when retrospectively defending their decision. Under uncertainty, prescribing or continuing antibiotics was generally perceived to be most defensible. Some consultants recounted interrogations in the coroner’s court about why they stopped or did not prescribe antibiotics (quote 4, table 3). None described being questioned for starting or continuing antibiotics.
Prescribing consistent with particular policies was perceived as defensible. One frequently raised national policy was Sepsis Six, which states that if a patient is thought to be septic, clinicians must prescribe empiric antibiotics within an hour.31 Some clinicians thus felt pressured to start antibiotics urgently because they believed that this behaviour was the most defensible (quote 5, table 3). This 60 min target is also a National Institute for Health and Care Excellence quality standard.32
Concerns about prescribing’s adverse consequences: AMR and antibiotic toxicity
Clinicians’ predominant concern was AMR; they were aware of resistance and valued protecting antibiotic choice and efficacy. Despite perceiving AMR as important, these concerns were over-ridden by perceptions of antibiotic necessity to protect the patient and the clinician (quote 6, table 3). AMR concerns were moderated by perceptions of personal responsibility and accountability. Clinicians saw antibiotics as preventing consequences for which they were immediately responsible, with safeguarding the patient perceived as the over-riding priority. They saw preventing AMR as distal to this aim and less of an immediate priority. There was variation between clinicians regarding the importance of AMR in prescribing decisions for individual patients. Some doctors saw strong links between their own prescribing and AMR (quote 7, table 3), whereas a minority felt less personally responsible for AMR and doubted whether resistance would occur (quote 8, table 3).
Unlike AMR, antibiotic toxicity concerns were infrequent. Strikingly, 3 out of 35 clinicians raised antibiotic-related adverse effects in their VBI. The remainder did not mention potential antibiotic side effects as a decision-making consideration.
Balancing necessity and concerns: ‘being brave’ versus ‘being burnt’
In uncertainty, clinicians were motivated to prescribe antibiotics empirically to protect against undesirable consequences. Nonetheless, they also valued using antibiotics carefully to protect their unit’s ecology. In contrast to prescribing and continuing antibiotics when uncertain, clinicians referred to withholding and stopping potentially unnecessary antibiotics as ‘bravery’ (quote 9, table 3). Framing ‘conservative’ prescribing as bravery illustrates clinicians’ expectations of adverse consequences resulting from not prescribing; this language highlights clinicians’ strong beliefs about antibiotics’ necessity despite acknowledgement of antibiotic-related concerns.
Bravery was believed to improve with clinical experience. Consultants described a ‘gut feeling’ they used to make decisions (quote 10, table 3); trainees recognised bravery’s benefits but worried about possible consequences of not prescribing (quote 11, table 3).
Negative experiences may over-ride this bravery. Previously ‘being brave’ with antibiotics but experiencing negative consequences may stifle clinicians’ bravery with future patients (quote 12, table 3). ‘Being burnt’ appears to have motivated consultants to revert to prescribing or continuing antibiotics in future patients in uncertainty. Experiencing adverse personal consequences after not prescribing may strengthen antibiotic necessity perceptions, discouraging bravery in future decisions.
Contextual factors
The decision-making context moderated clinicians’ necessity and concerns perceptions. It could either reinforce or over-ride inclinations to prescribe in uncertainty. Contextual factors include decision-making in-hours versus out-of-hours, input from external team members and ICU prescribing norms.
Table 4 shows supporting quotations.
Supporting quotations for contextual factors theme
Decision-making in-hours versus out-of-hours
In-hours, clinicians felt more confident to withhold antibiotics in uncertainty. On weekdays, consultant intensivists typically made antibiotic decisions with clinical microbiology involvement. Early-career and middle-grade trainees reported having little input (quotes 13–14, table 4). In-hours decisions were seen as more judicious than out-of-hours decisions, with clinicians having higher thresholds to prescribe antibiotics during ‘core hours’ (quote 15, table 4).
For out-of-hours prescribing, consultants provide contingency ‘SOS plans’ for early-career and middle-grade trainees, to whom decision-making responsibility falls. If trainees felt confident, they could prescribe without input; otherwise, they were expected to contact on-call ICU and microbiology consultants. Some perceived variation in consultants’ expectations about being called and worried about disturbing them at night (quote 16, table 4).
If trainees felt unable to access consultant support, they were likely to start or continue antibiotics empirically. Many viewed prescribing antibiotics as ‘safest’, favouring broad-spectrum antibiotics which they believed were less risky than narrow spectrums (quote 17, table 4). These beliefs illustrate trainees’ strong necessity beliefs out-of-hours; they also anticipated that consultants would overturn inappropriate prescriptions in-hours (quote 14, table 4).
Input from external team members
Clinicians reported that external team members—generally clinical microbiologists and pharmacists—often increased intensivists’ confidence about withholding or stopping potentially unnecessary antibiotics. These ‘antimicrobial stewards’ would challenge potentially inappropriate antibiotic decisions, remind clinicians about local AMR rates and reach a consensus about antibiotics with consultant intensivists (quote 18, table 4). Consultant intensivists appreciated these negotiations and occasionally would await this input before making decisions.
There were some points of tension regarding clinical microbiology advice. As microbiologists did not usually examine patients, certain clinicians worried that microbiology recommendations relied on potentially inaccurate or incomplete information from ICU trainees (quote 19, table 4). Similarly, certain consultants expressed concerns that some trainees followed microbiology recommendations without checking or understanding the rationale (quote 20, table 4). Trainees valued microbiology input, but some felt deskilled in their independent prescribing abilities because of this support (quotes 20–21, table 4).
Other external team members would forcefully advocate inappropriate decisions, which included starting, adding and continuing potentially unnecessary antibiotics. For instance, one surgeon would insist on multiple days of prophylaxis, although local practice was 24 hours (quote 22, table 4). Although ICU consultants had the ultimate decision, none reported over-ruling the external party. Rather, they would negotiate to encourage an appropriate decision (quote 23, table 4). Discussion outcomes varied—some successfully persuaded more appropriate decisions (quote 24, table 4), whereas others acquiesced to external pressure because they feared possible consequences or were unable to convince resolute individuals (quotes 22 and 25, table 4).
ICU prescribing norms
Local norms influenced clinicians’ prescribing. These include informal norms referring to what clinicians believed was locally encouraged and prescribed, official institutional guidelines and AMS policies (table 1), and clinicians’ attitudes towards policies in terms of adhering to recommendations.
Consultants shaped informal norms and taught or modelled them to trainees. Following these norms and prescribing consistent with colleagues were believed to signal that one’s decisions were defensible. Thus, local norms likely affected anticipated interpersonal prescribing consequences and clinicians’ necessity perceptions of protecting themselves with prescriptions.
In hospitals 1 and 4, hasty empiric prescribing was discouraged in favour of identifying the source of infection before prescribing (quote 26, table 4). Hospitals 2 and 4 also banned certain broad-spectrum agents, aiming to prevent AMR development (quote 27, table 4).
Other informal norms arguably motivated suboptimal antibiotic practices. Middle-grade trainees in hospital 2 described patients receiving potentially unnecessary antibiotics, patients receiving broader-spectrum antibiotics than required, and an unwillingness to stop antibiotics until after a 5-day course. These trainees reported reluctantly following these norms; they would prefer to use fewer broad-spectrum antibiotics and to stop antibiotics sooner if patients had clinically improved (quotes 28–29, table 4).
Units also differed in attitudes towards institutional guidelines. Clinicians in hospitals 2, 3 and 4 believed guidelines must be followed, with consultants sometimes reprimanding guideline deviations. Conversely, hospital 1 clinicians believed that guidelines did not have to be strictly followed (quotes 27 and 30–31, table 4). Variation in adherence beliefs may result from whether clinicians saw guidelines as flexible enough to individualise patient care. Clinicians in units with strict adherence beliefs tended to see guidelines as sufficiently tailored for their patient population, whereas doctors in units with less stringent adherence norms tended to see guidelines as less tailored to individual patients.
Discussion
This is the first study applying NCF to explain ICU antibiotic decision-making. Prescribing decisions were usually made in uncertainty and high stakes due to the significant consequences of antibiotic undertreatment and overtreatment.
Antibiotic decisions were influenced by clinicians’ perception of the necessity to prescribe relative to their concerns about the consequences of doing so. Necessity perceptions were strongly influenced by beliefs that antibiotics would protect patients from deterioration and clinicians from ethical, legal and reputational consequences of undertreatment. Similar beliefs were identified by a systematic review of determinants of hospital antibiotic prescribing.10
Consistent with previous studies,10 our participants commonly cited AMR as a concern. However, AMR was perceived as more distal relative to antibiotic necessity as proximal protection. Similarly, few clinicians identified antibiotic toxicity concerns as key decision-making contributors. Clinicians’ strong necessity beliefs and low concerns translated into favouring prescribing or continuing empiric antibiotics, termed ‘erring on the side of caution’.
A loss aversion bias may augment this inclination to prescribe. This heuristic is where subjective losses outweigh equivalent potential gains when there are perceived risks and uncertain outcomes, incentivising individuals to behave in a way that minimises their likelihood of experiencing penalties.33 34 Clinicians’ inclination to prescribe is thus understandable given the immediacy and severity of consequences associated with antibiotic undertreatment compared with those associated with overtreatment. Clinicians are also individually responsible for the consequences associated with undertreatment, whereas the consequences associated with overtreatment are collective. This finding is consistent with previous assertions that the severe consequences of undertreatment for individuals motivate hospital antibiotic overprescription.18
Context affected clinicians’ inclination to prescribe in uncertainty. Like prior research, prescribing in-hours versus out-of-hours,35 input from certain external team members36 and prescribing norms37 were perceived to influence decision-making. Similarly, prescribers’ capabilities,38 past experience39 and external policy40 may affect this behaviour (figure 1). Further research should explore the relationships between these factors.

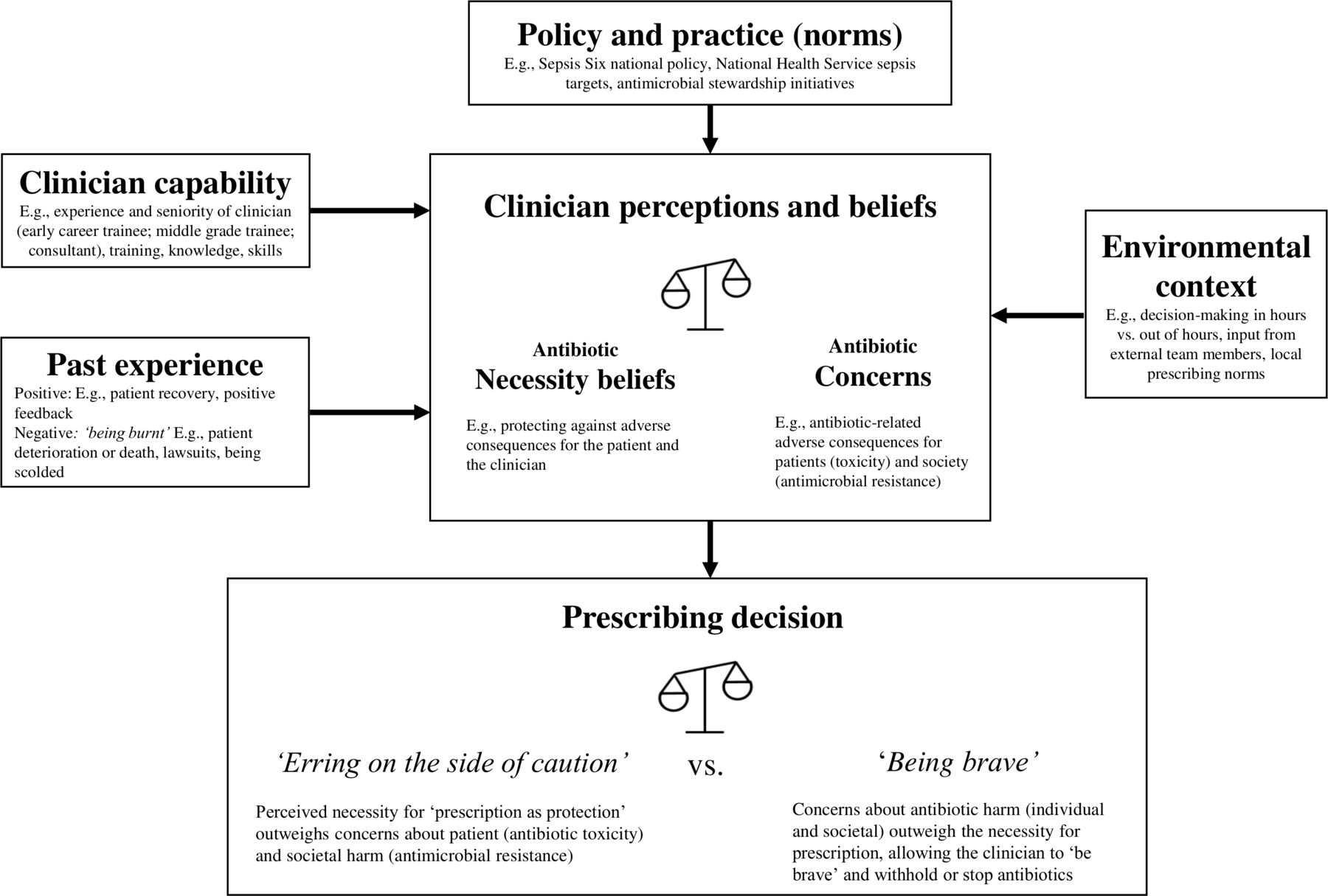{kind=link}
Factors influencing intensive care unit clinicians’ antibiotic prescribing in clinical uncertainty.
A repeatedly stated view was that ‘complete antibiotic courses’ militated against resistance. While the view is valid (eg, in tuberculosis),41 it is questionable in the ICU where standard treatment courses (eg, for pneumonias) have been progressively shortened42 and early termination or de-escalation minimises selection pressure on gut flora, which (rather than the proximate infection) is the likely source of future resistance. If there is no pathogen, completing the course has no possible merit and may cause collateral harm.
Quality and safety recommendations
Clinicians’ perceptions of the proximal need for antibiotics appear to outweigh their antibiotic-related concerns, leading to favouring overprescription in uncertainty. This behaviour is understandable; however, inappropriate empiric antibiotics may increase the risk of death43 and may promote AMR. Our participants recognised AMR’s threat; however, they viewed it as distal and did not prioritise it during decision-making.
Our findings have implications for AMS intervention development in ICUs. Interventions designed to increase AMR awareness are less likely to be effective than approaches that address clinicians’ necessity concerns evaluation when making prescribing decisions for individual patients. Our participants were concerned about distal AMR, yet prioritised their proximal need to protect against the consequences of not prescribing. Thus, interventions raising clinicians’ concerns about potential antibiotic-related harms to the patient are more likely to reduce antibiotic necessity perceptions than general AMR-related messages.
New technology may help reconcile clinicians’ beliefs about the necessity to prescribe/not prescribe. Molecular diagnostics can detect bacteria, viruses and antibiotic resistance genes within hours,44 rather than the 48–72 hours needed for laboratory culture. Having molecular diagnostic results may encourage clinicians to prescribe narrower-spectrum antibiotics than ordinarily used for empiric therapy, stop antibiotics if a virus and/or no bacterial pathogens are found, and de-escalate to narrow-spectrum antibiotics once a pathogen is identified. Nevertheless, given the potential consequences of undertreatment, clinicians may not trust negative results and may continue empiric antibiotics. In context, clinicians’ antibiotic necessity perceptions may explain findings of a lack of difference in intensivist prescribing with and without a highly sensitive rule-out test (ie, one advising discontinuing antibiotics because an infection was unlikely).45 Novel information may be insufficient to over-ride established decision-making beliefs; confidence in such systems and interventions increasing the defensibility of non-prescribing should be developed to encourage behaviour change.
Contextual factors can moderate the preference of erring on the side of caution. ICU consultants and microbiologists should continue creating SOS plans to follow out-of-hours and should ensure these accord with AMS principles. Antimicrobial stewards may experience barriers to participation in antibiotic decision-making (eg, limited consultant contact)46; such obstacles should be assessed and addressed locally. Units should also create norms promoting AMS practices (eg, restricting specific broad-spectrum antibiotics).
Limitations
This study has limitations. VBIs are self-reports about clinicians’ prescribing intentions without real patient-related or clinician-related consequences. Therefore, participants may answer differently in vignette decisions from how they would have acted with actual patients (eg, in terms of withholding antibiotics). While we intentionally designed vignettes with no correct answers to encourage reflection in uncertainty, future research using vignettes with ‘correct’ responses may better understand factors associated with inappropriate prescribing.
We investigated prescribing in English ICUs. We recognise that Hulscher and colleagues’ review12 included national culture, and that developed and developing nations have differing drivers to AMR development.47 More research should explore antibiotic decision-making in other cultural contexts, including the ‘open ICU’ model, where patients remain under the care of their primary physician or surgeon rather than intensivists; this model, which is nowhere followed in the UK, has less central control and has been associated with higher infection rates.48
We sampled from four hospitals; staff may not fully represent English ICUs. However, these hospitals were selected to ensure diversity and participants would have trained at multiple institutions, so attitudes and behaviours would have evolved from a wider footprint.
Our focus groups included two microbiologists and one infectious disease doctor. Our focus was on ICU bedside clinician decision-making; future studies should explore specialist decision-making.
Conclusion
This is the first study exploring antibiotic decision-making in ICU using NCF. When making antibiotic decisions, clinicians must balance important consequences for the individual patient, themselves and the society, under high-stakes and uncertain conditions. Our findings indicate that clinicians favoured erring on the side of caution—prescribing or continuing empiric antibiotics in uncertainty to protect against possible consequences of undertreatment. Clinicians viewed antibiotics’ necessity (ie, protection for their patients and themselves) as outweighing concerns about antibiotic toxicity and AMR. Stewardship initiatives are more likely to be effective if they address clinicians’ perceptions of antibiotic necessity and increase concerns about antibiotics’ potential harmful effects for individual patients.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This research received ethical approval from the Camden and Kings Cross Research Ethics Committee (16/LO/1618).
Acknowledgments
We would like to thank all ICU staff who were involved in organising or participating in the research. We also thank Norwich Clinical Trials unit and our Patient and Public Involvement group. This research is supported by researchers and infrastructure at the National Institute for Health Research University College Hospitals and Imperial Biomedical Research Centres. YJ is a Health Foundation Improvement Science Fellow.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at This work was scheduled to be presented at the European Congress of Clinical Microbiology and Infectious Diseases conference in April 2020; this conference was cancelled due to the COVID-19 outbreak. This work was presented at the virtual International Symposium on Intensive Care and Emergency Medicine conference on September 15-18, 2020 and at the International Society for Medication Adherence conference on November 10-20, 2020.
Collaborators INHALE WP2 Study Group: authors and their affiliations as above; and Julie Barber and Laura Shallcross, University College London; Jeronimo Cuesta, North Middlesex Hospital; Mark Peters and Nigel Klein, Great Ormond St Hospital and UCL Great Ormond St Institute of Child Health NIHR Biomedical Research Centre; Parvez Moondi, Norfolk and Norwich University Hospitals NHS Foundation Trust; Justin O’Grady, Quadram Institute and University of East Anglia; Juliet High, Charlotte Russell and David Turner, Norwich Clinical Trials Unit, University of East Anglia; and Suveer Singh, Chelsea and Westminster Hospital NHS Foundation Trust.
Contributors This study was conceptualised and designed by RH, SJB, TWR, DB, VIE, DML and VG. Vignettes and interview guides were written by SJB, DB and TWR. Focus groups and interviews were conducted by NB and YJ. Data were analysed by AMP and NB, with input from YJ, SJB, TWR and RH. The manuscript was written by AMP, with input from the remaining authors.
Funding This paper presents independent research funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research Programme (Reference Number: RP-PG-0514-20018). The views expressed are those of the authors and not necessarily those of the National Health Service, the NIHR, or the Department of Health and Social Care.
Competing interests VIE reports personal fees and non-financial support from bioMerieux, personal fees from Curetis and non-financial support from Oxford Nanopore Technologies, outside the submitted work. DML reports personal fees from Accelerate, Allecra, Antabio, Astellas, Beckman Coulter, bioMerieux, Cepheid, Centauri, Entasis, Johnson & Johnson, Meiji, Melinta, Menarini, Mutabilis, Nordic, ParaPharm, QPEX, Roche, Shionogi, Tetraphase, Wockhardt, Zambon, Cardiome and Eumedica. He also reports grants and personal fees from VenatoRx; personal fees and other (shareholder) from GlaxoSmithKline; personal fees and other (stock options) from TAZ; grants, personal fees and other (shareholder) from Merck/MSD and Pfizer; and other (shareholder) from Perkin Elmer and Dechra. All are outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.